Transapical Device Closure of a Submitral Left Ventricular Pseudoaneurysm After Mitral Valve Replacement
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00203. Epub July 6, 2026.
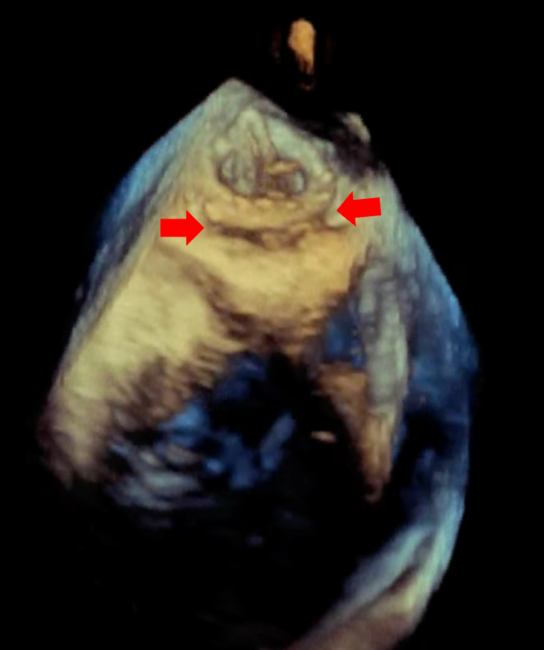
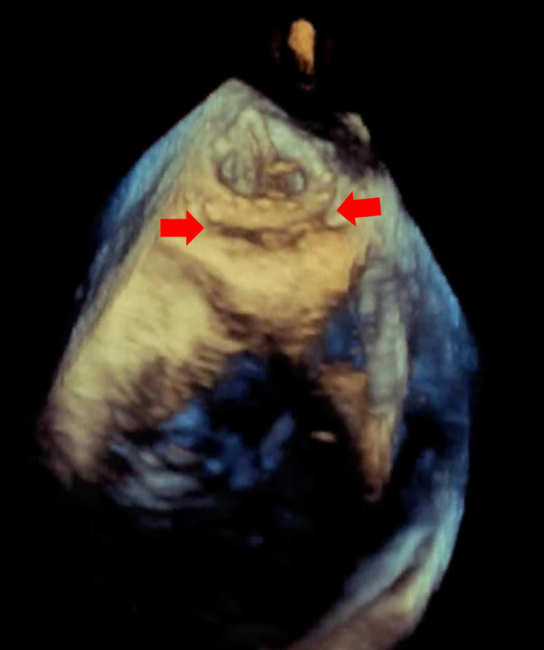
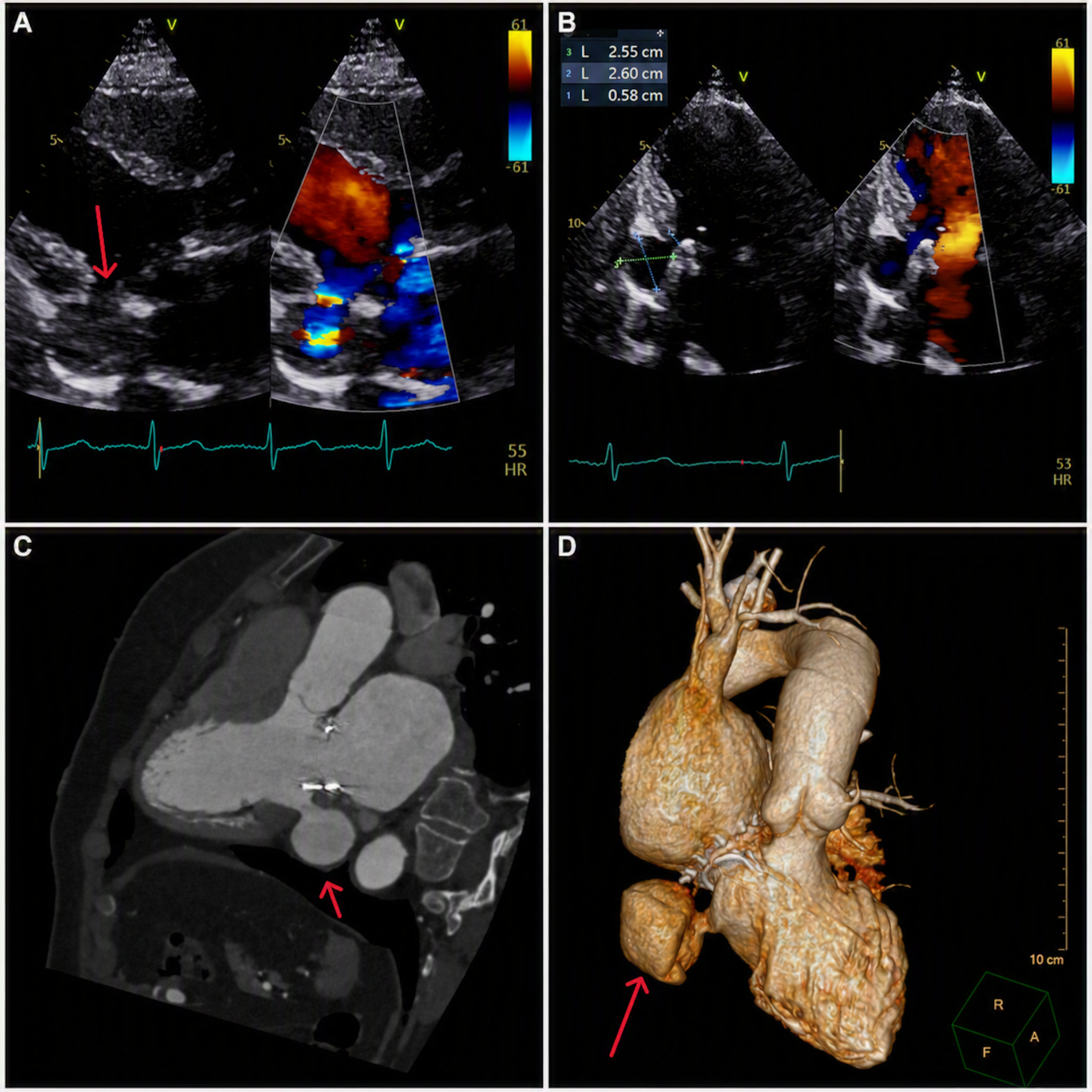
A 69-year-old woman with rheumatic severe mitral stenosis, treated 14 months earlier by minimally invasive bioprosthetic mitral valve (MV) replacement, presented with exertional dyspnea. Transthoracic echocardiography showed a submitral left ventricular (LV) pseudoaneurysm communicating with the LV cavity through a narrow neck; color Doppler demonstrated flow across the defect (Figure 1A, Video 1). Apical 3-chamber echocardiography measured the pseudoaneurysm cavity and neck (Figure 1B). Cardiac computed tomography confirmed the submitral/subannular location adjacent to the mitral prosthesis and defined its relation to the LV cavity (Figure 1C and D).
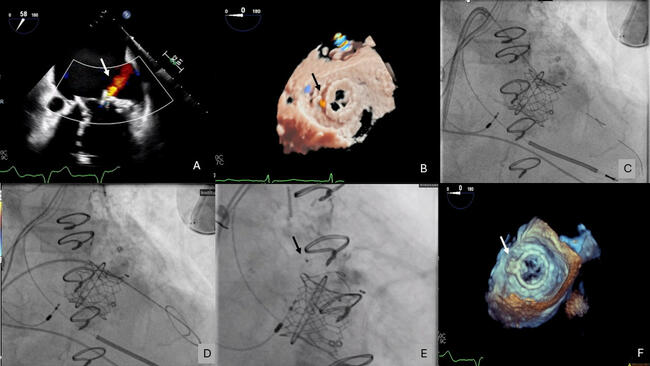
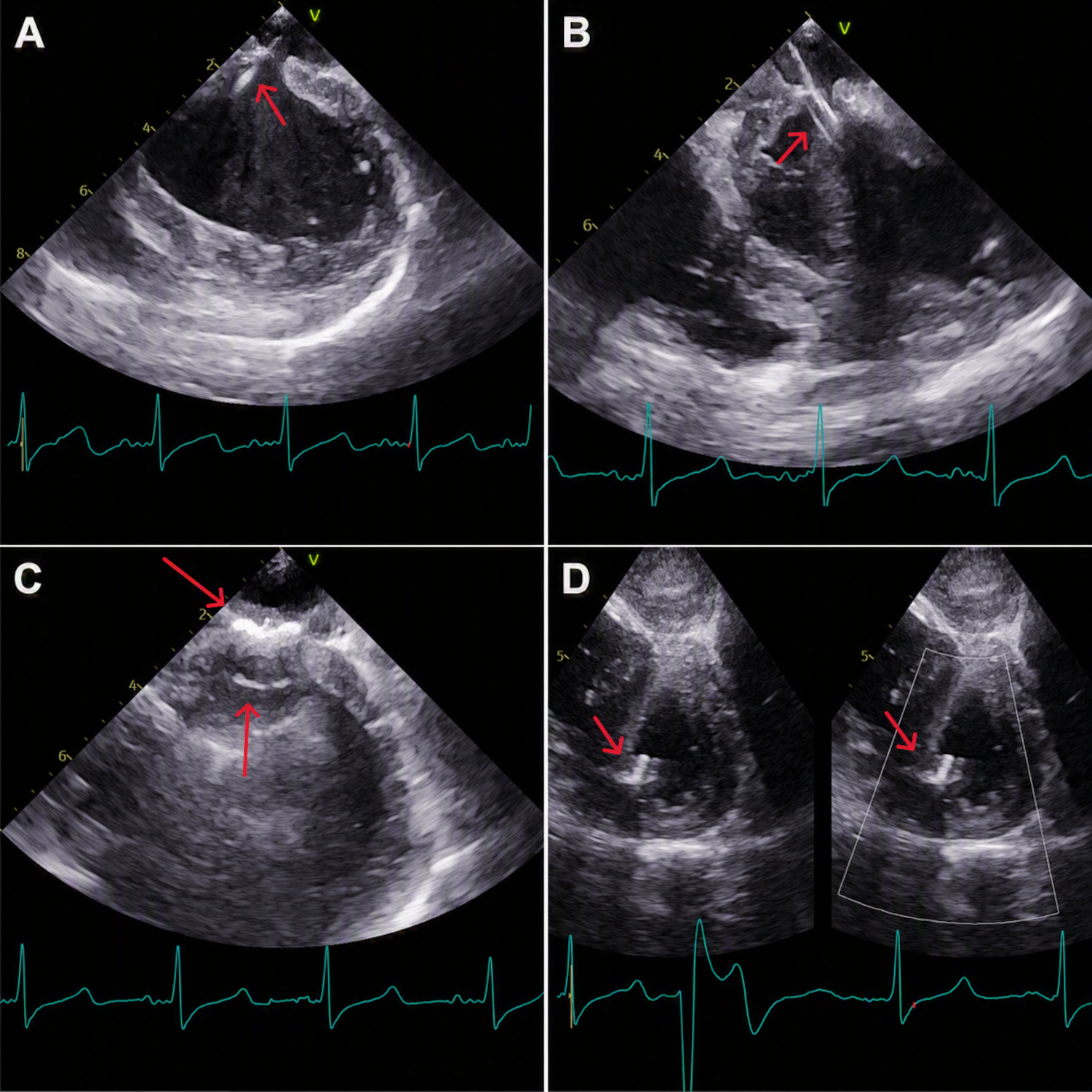
After joint cardiac team discussion, transapical device closure was selected because the pseudoaneurysm had a discrete neck and the transapical route provided the most direct trajectory for coaxial crossing and device deployment. The procedure was performed under fluoroscopic and echocardiographic guidance. During LV apical puncture, simultaneous left coronary angiography (CAG) was performed to delineate the left anterior descending artery and avoid coronary injury (Video 2). The pseudoaneurysm neck was crossed under combined transesophageal echocardiographic and fluoroscopic guidance, and the catheter was positioned within the pseudoaneurysm cavity (Figure 2A and B, Video 3). A 10-mm HeartR muscular ventricular septal defect occluder (Lifetech Scientific) was deployed across the pseudoaneurysm neck, with both discs positioned on either side of the defect, and was released after stable positioning was confirmed (Figure 2C, Video 4). The transapical LV access site was then closed with a 6/4-mm Cera patent ductus arteriosus occluder (Lifetech Scientific) (Figure 2D).
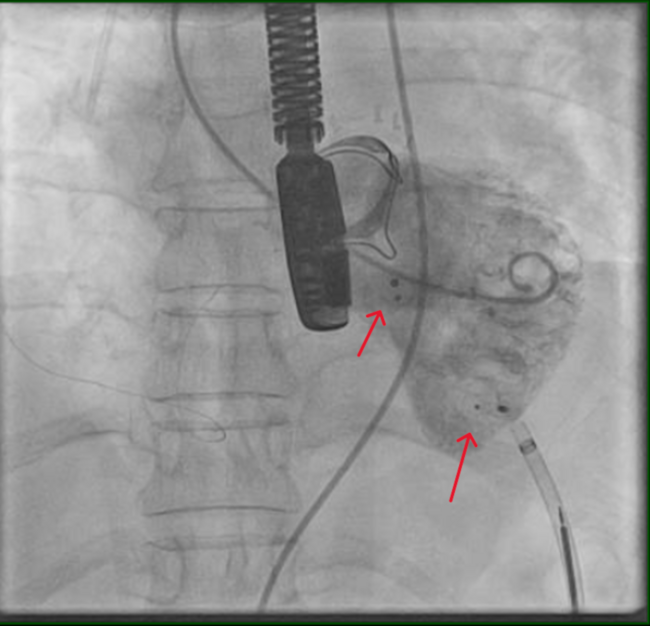
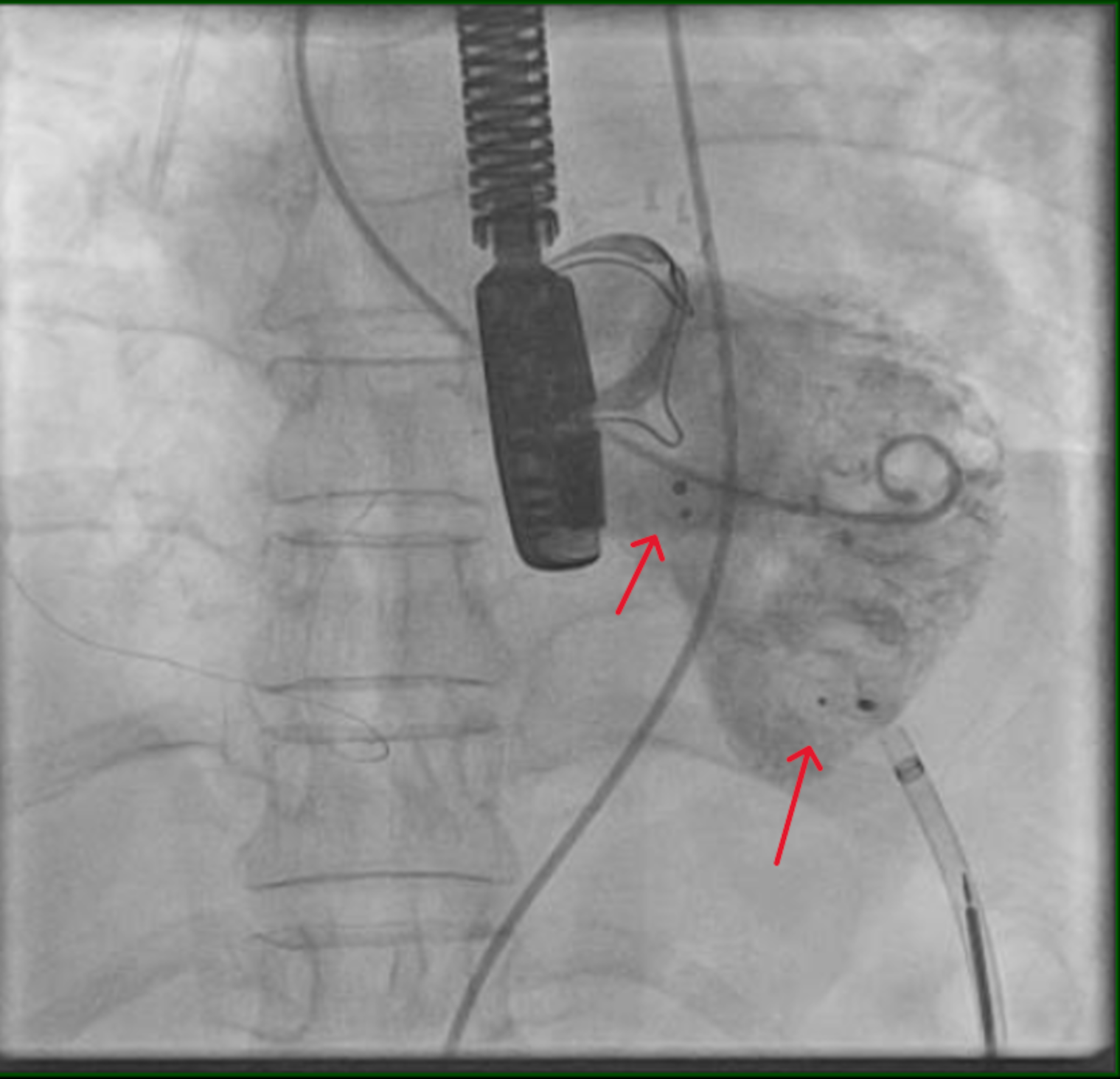
Final LV angiography in left anterior oblique cranial projection showed both devices in position, with no residual opacification of the pseudoaneurysm or access site leak (Figure 3, Video 5). At the 6-month follow-up, echocardiography showed both occluder devices in situ, no residual flow, and normal prosthetic MV function (Video 6).
LV pseudoaneurysm after MV replacement is rare and may be associated with progressive enlargement, rupture, thromboembolism, or compression of adjacent structures. Percutaneous closure has been reported as a feasible alternative in selected patients with suitable anatomy, particularly when redo surgery is undesirable.1-3 This case highlights the value of multimodality imaging for anatomical definition, left CAG during apical puncture for procedural safety, and planned closure of both the pseudoaneurysm neck and the transapical access site.
Affiliations and Disclosures
Muzamil Yousuf Lone, MD; Sumanyu Suresh, MD; Bijulal Sasidharan, MD, DM
From the Department of Cardiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, Kerala, India
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for intervention(s) described in the manuscript and for the publication thereof, including any and all images.
Address for correspondence: Muzamil Yousuf Lone, MD, Department of Cardiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, Kerala, India. Email: loneappu1995@gmail.com; X: @muzamil19951995
References
1. Kim I, Oakley L, Shah A, Makkar RR. Percutaneous closure of left ventricular pseudoaneurysm using simultaneous transseptal and transapical approach: a case report. Eur Heart J Case Rep. 2021;5(9):ytab311. doi:10.1093/ehjcr/ytab311
2. Bezgin T, Celik AI, Baytugan NZ, Karakoyun S, Cagdas M. A guidewire-free approach for percutaneous closure of left ventricular pseudoaneurysm. J Invasive Cardiol. 2024;36(5). doi:10.25270/jic/23.00278
3. Basman C, Kaple R, Yoon SH, et al. Transcatheter closure of a complex paravalvular leak associated with a large ventricular pseudoaneurysm. J Invasive Cardiol. 2025;37(5). doi:10.25270/jic/24.00351