Percutaneous Management of Delayed Aortic Annular Rupture After Transcatheter Aortic Valve Implantation Complicated by Severe Aortic Regurgitation
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00158. Epub July 1, 2026.
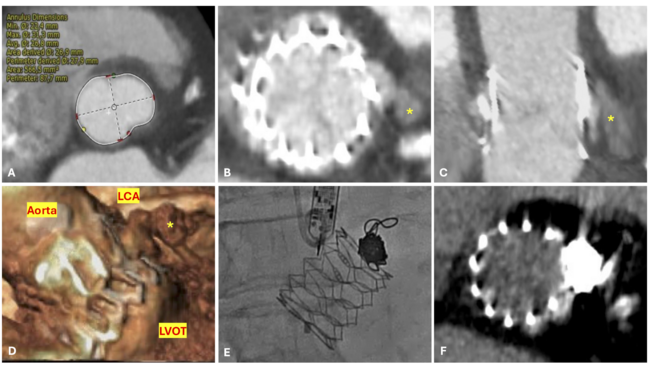
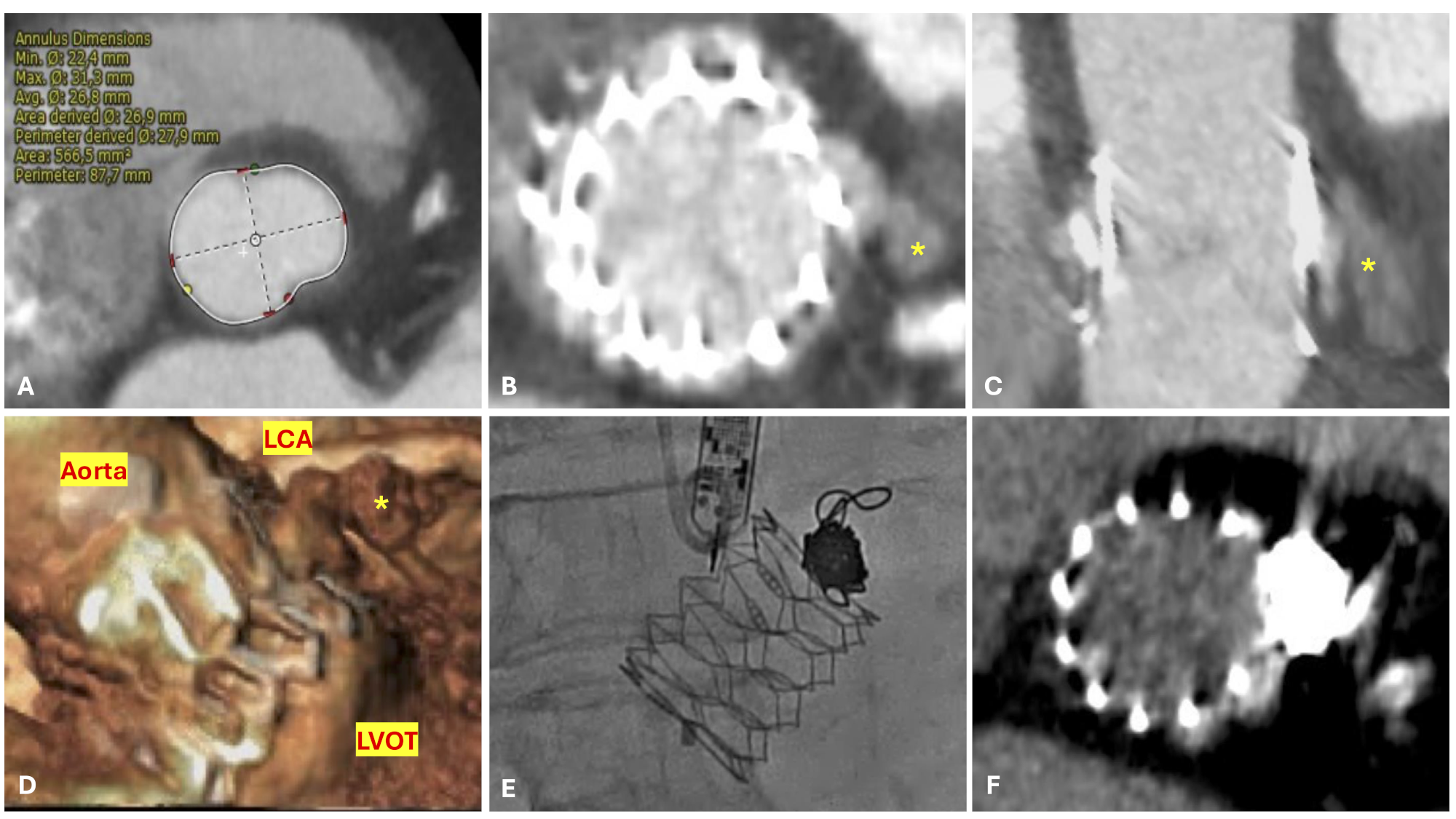
An 86-year-old woman with severe aortic stenosis and high surgical risk (Society of Thoracic Surgeons score 8.3%) was referred for transcatheter aortic valve implantation (TAVI). Preprocedural computed tomography (CT) confirmed transfemoral feasibility and showed severe, symmetrically distributed leaflet calcification, a moderately elliptical annulus with an area of 566.5 mm², and no relevant annular or left ventricular outflow tract (LVOT) calcification (Figure A). A 27.5-mm Myval OctaPro+ valve (Meril Life Sciences) was implanted with approximately 5% intended oversizing, achieving satisfactory hemodynamic results with mild aortic regurgitation (AR) (Video 1).
Three hours after TAVI, the patient developed cardiogenic shock. Echocardiography revealed cardiac tamponade and severe AR (Video 2). After emergent pericardiocentesis, urgent CT demonstrated aortic annular rupture with pseudoneurysm at the level of the left coronary sinus (LCS) (Figure B-D). Owing to prohibitive surgical risk, a bail-out percutaneous strategy was undertaken, with coil embolization of the pseudoaneurysm.
Aortic angiography demonstrated new-onset severe AR with clear contrast extravasation through the LCS (Video 3). Under fluoroscopic and transesophageal echocardiography guidance, the pseudoaneurysm was engaged from the femoral access using a 6F Judkins Left (JL) 4 guiding catheter. Given the proximity to the left main coronary artery, a second JL3.5 guiding catheter was advanced via right radial access to protect the left coronary artery. A standard 0.014-inch coronary guidewire was then positioned in the pseudoaneurysm, and a LANTERN microcatheter (Penumbra, Inc.) was advanced to enable coil delivery. After multiple failed attempts due to coil prolapse into the aorta or LVOT, a 12-mm × 60-cm Ruby Coil (Penumbra, Inc.) was successfully deployed, achieving effective aortic sealing with residual mild AR (Figure E, Video 4).
Follow-up CT confirmed complete rupture sealing (Figure F), and transthoracic echocardiogram showed adequate valve competence (Video 5). The patient was discharged 5 days later and remained asymptomatic at the 3-month follow-up.
Affiliations and Disclosures
Caterina Cavazza, MD1; Francesco Contorni, MD1; Carolina Moretti, MD2; Manfredi Arioti, MD2; Andrea Casadei, MD3; Annamaria Di Cesare, MD1,4; Samuela Carigi, MD1; Filippo Ottani, MD1
From the 1Emergency and Cardiology Department, Infermi Hospital Rimini, Romagna Local Health Authority, Rimini, Italy; 2Emergency and Cardiology Department, Santa Maria delle Croci Hospital, Romagna Local Health Authority, Ravenna, Italy; 3Radiology Department, Infermi Hospital Rimini, Romagna Local Health Authority, Rimini, Italy; 4Department of Life, Health and Enviromental Sciences, University of L'Aquila, L’Aquila, Italy.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for intervention described in the manuscript and for the publication thereof, including any and all images.
Address for correspondence: Francesco Contorni, MD, Emergency and Cardiology Department, Infermi Hospital Rimini, Romagna Local Health Authority, Rimini, Italy. Email: francesco.contorni@auslromagna.it