Long-Segment Honeycomb-Like Structure of the Right Coronary Artery Presenting With Acute Coronary Syndrome
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00187. Epub June 30, 2026.
A 60-year-old man presented with typical anginal chest pain. High-sensitivity troponin T levels were elevated. Transthoracic echocardiography demonstrated inferior wall hypokinesia. The patient was admitted with a diagnosis of non-ST-segment elevation myocardial infarction (NSTEMI).
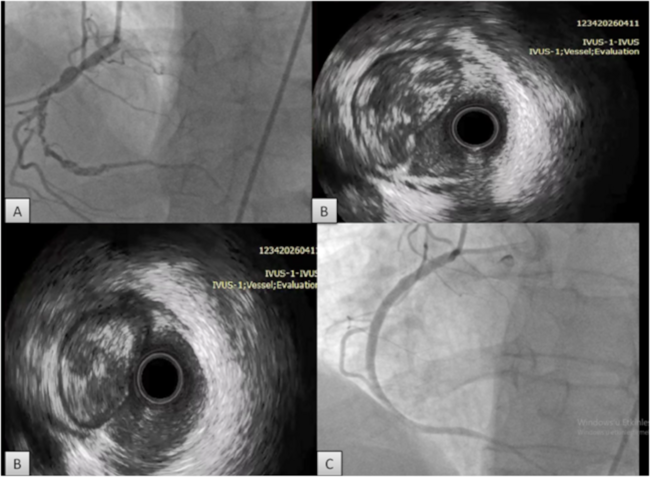
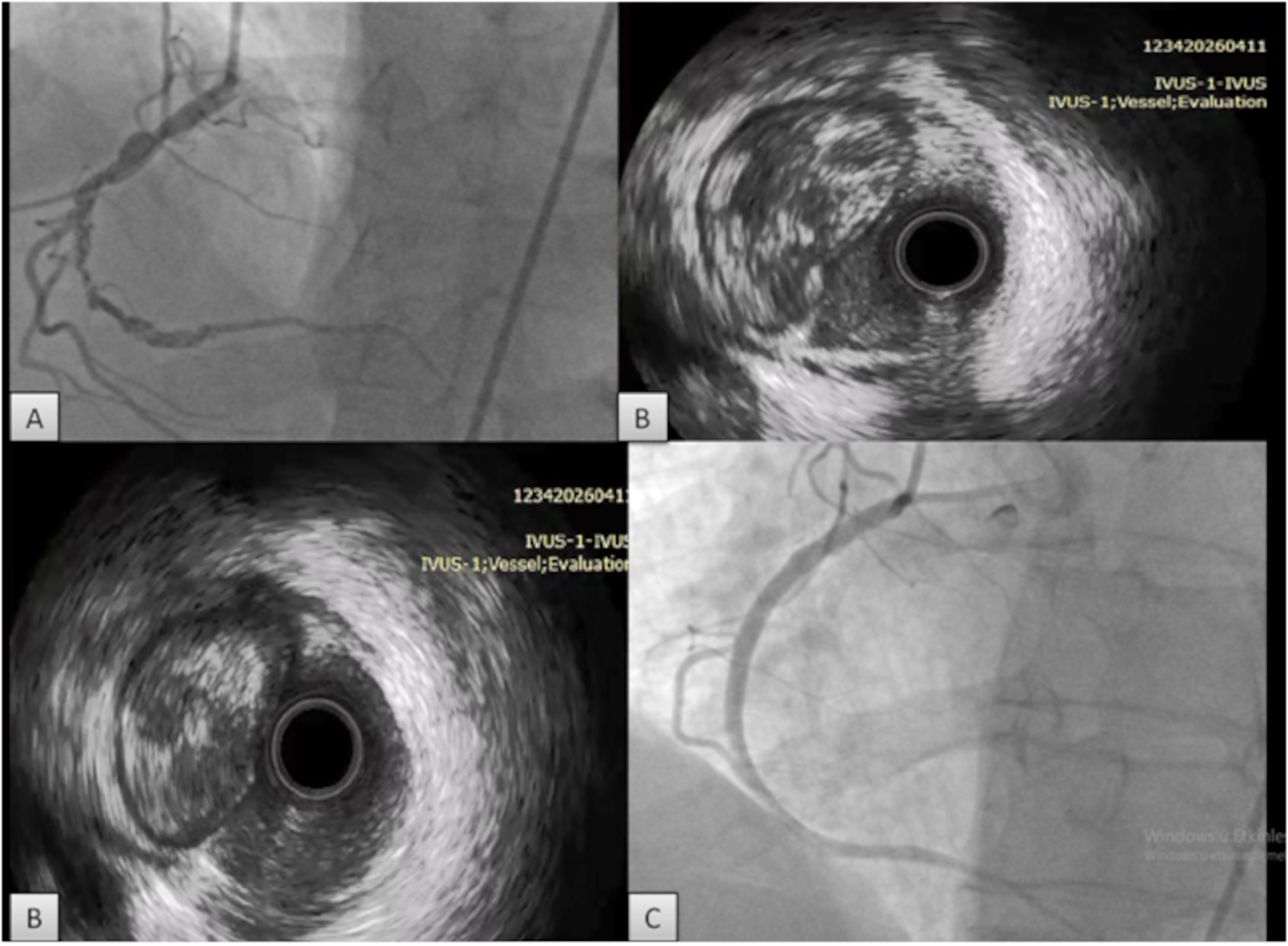
Coronary angiography demonstrated a long-segment, irregular filling defect with diffuse haziness in the right coronary artery (RCA) (Figure A, Video 1). Initial attempts to cross the lesion using a workhorse guidewire, followed by Fielder XT (ASAHI INTECC) and PILOT 200 (Abbott) guidewires, were unsuccessful. Lesion crossing was ultimately achieved using a microcatheter-supported Gaia 2 guidewire (ASAHI INTECC).
Intravascular ultrasound (IVUS) imaging revealed multiple communicating luminal channels separated by thin septa, consistent with a recanalized thrombus, forming a honeycomb-like structure (HLS) (Figure B, Video 2). Following multiple predilatations to fenestrate the septal structures, successful percutaneous coronary intervention (PCI) of the RCA was performed, resulting in an optimal final angiographic result (Figure C, Video 3).
Previous IVUS and optical coherence tomography studies suggest that HLS represents spontaneous recanalization of an organized thrombus, resulting in a characteristic spiderweb or honeycomb-like appearance.¹ We report a long-segment HLS presenting as NSTEMI with chronic total occlusion (CTO)-like procedural features during PCI.
Although HLS is generally considered a manifestation of spontaneous thrombus recanalization, extensive lesions may exhibit CTO-like behavior during intervention.² In the present case, the long lesion length and multiple septal partitions likely contributed to difficulty crossing the guidewire, necessitating microcatheter support and CTO-oriented crossing strategies. Recognition of this entity is important, as advanced CTO techniques may occasionally be required for successful revascularization.
Affiliations and Disclosures
Burcu Kodal, MD; Ali Nail Kaya, MD; Aziz Inan Celik, MD
From the Department of Cardiology, Heart Center, Gebze Fatih State Hospital, Kocaeli, Turkey.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient(s) for intervention(s) described in the manuscript and for the publication thereof, including any and all images.
Address for correspondence: Burcu Kodal, MD, Gebze Fatih State Hospital, Department of Cardiology, Osman Yilmaz Neighborhood, Istanbul Street, 127, Kocaeli 41400, Turkey. Email: burcu_kodal@hotmail.com
References
- Toutouzas K, Karanasos A, Stathogiannis K, et al. A honeycomb-like structure in the left anterior descending coronary artery: demonstration of recanalized thrombus by optical coherence tomography. JACC Cardiovasc Interv. 2012;5(6):688-689. doi:10.1016/j.jcin.2012.01.024
- Souteyrand G, Valladier M, Amabile N, et al. Diagnosis and management of spontaneously recanalized coronary thrombus guided by optical coherence tomography - lessons from the French "Lotus Root" registry. Circ J. 2018;82(3):783-790. doi:10.1253/circj.CJ-17-0810