When the Left Ventricle Dances: Ballerina Foot Appearance in Hypertrophic Cardiomyopathy
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00152. Epub May 27, 2026.
A 30-year-old man presented with acute onset chest pain followed by an episode of syncope. He had no prior history of hypertension, diabetes, or any other known cardiac disease. A 12-lead electrocardiogram (ECG) showed left ventricular (LV) hypertrophy, with deep T-wave inversions in the lateral leads, suggestive of an LV strain pattern. A 2-dimensional echocardiogram revealed asymmetric septal hypertrophy with normal LV function with a significant resting LV outflow tract (LVOT) gradient of 70 mm Hg.
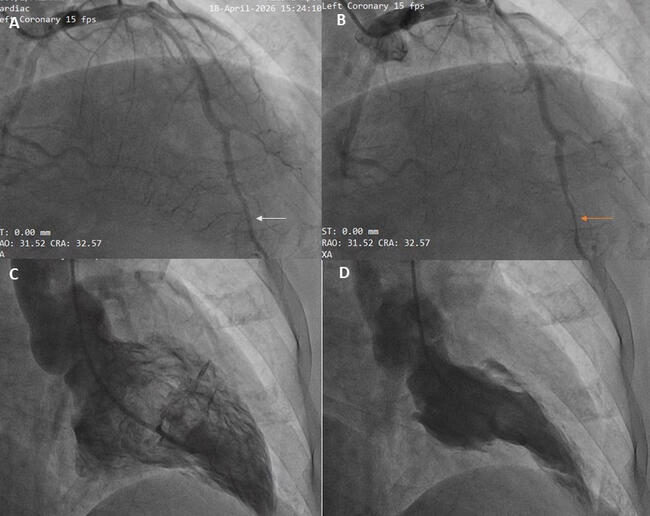
After obtaining informed consent, the patient was taken up for a coronary angiography. The epicardial coronary arteries were normal. However, a myocardial bridge was noted in the distal left anterior descending artery LAD (Figure A and B, Video 1). LV angiogram demonstrated a markedly hypercontractile LV, with the near obliteration of the cavity in systole resembling a “ballerina foot,” a configuration reported in association with hypertrophic cardiomyopathy (Figure C and D, Video 2).
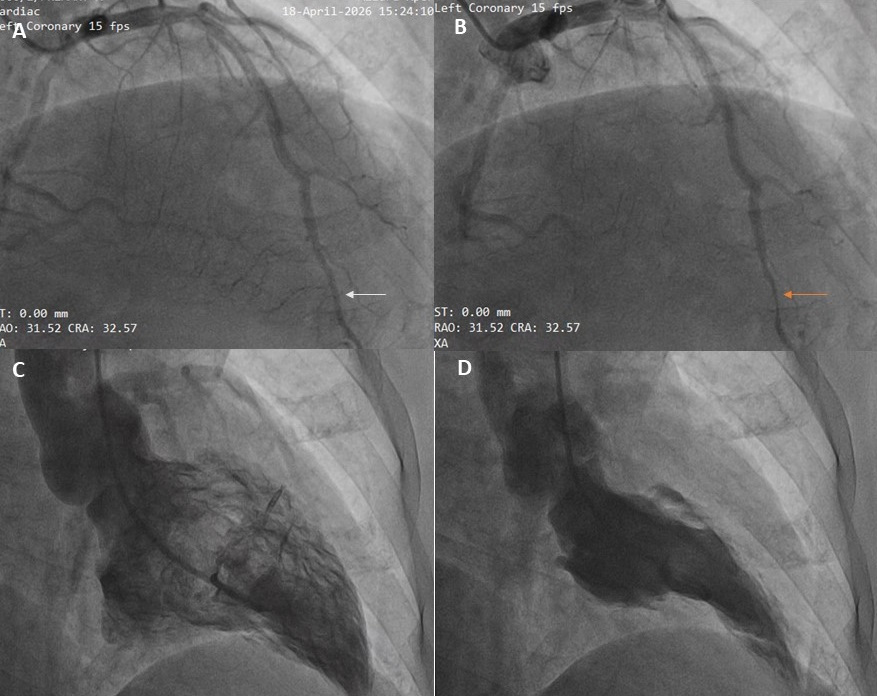
The “ballerina foot” appearance on LV angiography depicts exaggerated contraction in the basal and mid-cavity regions with significant hypertrophy in the basal septum. Although echocardiography remains the primary diagnostic method, these characteristic angiographic patterns can still help in consolidating the diagnosis by providing useful morphological clues.
This case emphasizes the importance of correlating ECG, echocardiographic, and angiographic findings, and acts as a reminder of less common but identifiable imaging signs in hypertrophic cardiomyopathy.
Affiliations and Disclosures
Mohit Gupta, MD; Anwar Hussan Ansari, MD, DM; Puneet Gupta, MD, DM; Anunay Gupta, MD, DM; Devesh Kumar, MD, MRCP, DM
From the Department of Cardiology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and for the publication of thereof, including photographs.
Address for correspondence: Devesh Kumar, MD, MRCP, DM, Department of Cardiology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi 110029, India. Email: devesh2.dk@gmail.com