


Diagnostic Performance of Angiography-Derived Coronary Physiology in Transcatheter Aortic Valve Implantation Pathway: A Systematic Review and Diagnostic Accuracy Meta-Analysis
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00141. Epub July 10, 2026.
Key Clinical Summary
- The diagnostic accuracy of angiography-derived coronary physiology in patients undergoing transcatheter aortic valve implantation (TAVI) remains uncertain because severe aortic stenosis and post-TAVI hemodynamic changes affect physiological assessment.
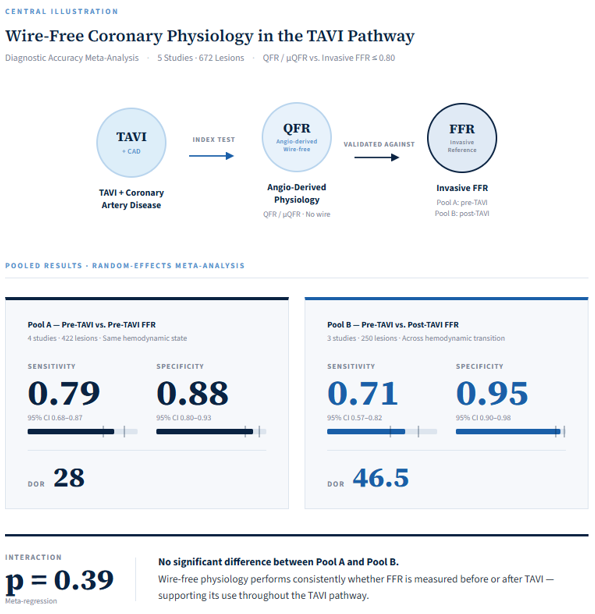
- Before TAVI, pooled sensitivity was 0.79 and specificity 0.88; with post-TAVI fractional flow reserve (FFR) as the reference, specificity increased to 0.95 but sensitivity reduced to 0.71.
- Overall discrimination was similar (Youden index 0.67 vs 0.66; P = .39), supporting potential use in the TAVI pathway while underscoring the need for prospective validation.
Abstract
Objectives. Coronary artery disease affects nearly half of patients undergoing transcatheter aortic valve implantation (TAVI), but the accuracy of angiography-derived, wire-free coronary physiology in severe aortic stenosis remains uncertain. The authors evaluated its diagnostic performance for detecting fractional flow reserve (FFR)-defined significant stenoses in TAVI candidates and assessed whether accuracy differed when invasive FFR was measured before vs after TAVI.
Methods. A diagnostic accuracy meta-analysis was performed including studies reporting lesion-level comparisons between angiography-derived physiology (threshold ≤0.80) and invasive FFR (≤0.80) in patients undergoing TAVI evaluation. All included studies evaluated quantitative flow ratio (QFR) or Murray-law-based QFR; no eligible studies using FFRangio or vFFR were identified. Pooled sensitivity and specificity were calculated using random-effects models. Diagnostic odds ratios (DOR), likelihood ratios, and post-test probabilities were derived. Meta-regression evaluated the impact of FFR timing (CRD420261332222).
Results. Five studies met inclusion criteria. Four studies (422 lesions) contributed to the primary analysis and 3 studies (250 lesions) to the secondary analysis. In the primary analysis, pooled sensitivity was 0.79 (95% CI, 0.68-0.87) and specificity 0.88 (95% CI, 0.80-0.93) (DOR 28). In the secondary analysis, sensitivity was 0.71 (95% CI, 0.57-0.82) and specificity 0.95 (95% CI, 0.90-0.98) (DOR 46.5), with comparable global discrimination (Youden index 0.66 vs 0.67). Meta-regression showed no significant interaction by reference timing (P = .39).
Conclusions. Angiography-derived coronary physiology demonstrates good diagnostic performance in patients undergoing TAVI evaluation, with comparable overall discrimination when referenced to both pre- and post-TAVI FFR, although interpretation is limited by the absence of a stable reference standard across hemodynamic states.
Introduction
Coronary artery disease (CAD) is present in nearly half of patients undergoing transcatheter aortic valve implantation (TAVI), and optimal management of concomitant coronary lesions remains a central component of contemporary structural heart care.1 Recent randomized evidence has reinforced the importance of physiology-guided strategies in this population. In the TCW trial, fractional flow reserve (FFR)-guided percutaneous coronary intervention (PCI) combined with TAVI was noninferior—and superior for selected outcomes—compared with surgical aortic valve replacement and coronary artery bypass grafting in patients with severe aortic stenosis and complex coronary disease.2 Furthermore, data from the NOTION-3 trial demonstrated that deferral of lesions with an FFR of greater than 0.80 was associated with favorable long-term outcomes, whereas conservative management of an FFR of less than or equal to 0.80 lesions was linked to higher cardiovascular risk, supporting the clinical validity of the 0.80 threshold in the TAVI setting.3 Together, these studies establish invasive FFR as a clinically meaningful tool in patients with severe aortic stenosis.
Despite this, important physiologic considerations remain. Severe aortic stenosis is characterized by chronic pressure overload, impaired coronary flow reserve, and microvascular remodeling, all of which may influence coronary hemodynamics. Relief of valvular obstruction following TAVI has been shown to modify invasive physiological indices in selected patients, raising uncertainty regarding the interpretation and optimal timing of coronary functional assessment within the TAVI pathway.4,5
Angiography-derived coronary physiology enables wire-free computational estimation of lesion-specific flow limitation based on standard angiographic images and has demonstrated good diagnostic accuracy compared with invasive fractional flow reserve in stable coronary artery disease populations.6-8 By avoiding pressure-wire manipulation and pharmacologic hyperemia, these computational techniques may offer procedural advantages during complex structural interventions. However, because angiography-derived indices are derived from mathematical modeling of coronary flow rather than direct hyperemic pressure measurements, it remains uncertain whether their diagnostic performance is preserved within the altered hemodynamic environment of severe aortic stenosis or across the transition from pre- to post-TAVI states.
Although several observational studies have evaluated angiography-derived physiology in patients undergoing TAVI assessment, available data remain limited and heterogeneous, particularly with respect to the timing of invasive FFR measurement. A focused quantitative synthesis within a strictly defined TAVI pathway population has not been performed.
Accordingly, we conducted a diagnostic accuracy meta-analysis to evaluate the performance of angiography-derived coronary physiology for detecting FFR-defined functionally significant stenoses in patients undergoing TAVI evaluation. We further examined whether diagnostic performance differs according to the timing of invasive FFR measurement (pre- versus post-TAVI), thereby assessing the hemodynamic robustness of wire-free physiological assessment within contemporary TAVI workflows.
Methods
Study design and registration
We performed a systematic review and diagnostic accuracy meta-analysis to evaluate the performance of angiography-derived (wire-free) coronary physiology for identifying functionally significant coronary stenoses in patients undergoing TAVI. The review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Diagnostic Test Accuracy (PRISMA-DTA) statement and the Meta-analysis of Observational Studies in Epidemiology (MOOSE) recommendations. The review was prospectively registered in the PROSPERO international register of systematic reviews (CRD420261332222). As only published aggregate data were analyzed, institutional review board approval and patient consent were not required.
Eligibility criteria
Eligible studies enrolled adult patients with severe aortic stenosis undergoing coronary evaluation as part of TAVI work-up. Studies were required to assess angiography-derived coronary physiology, including quantitative flow ratio (QFR), Murray-law-based QFR (μQFR), FFRangio, and vFFR, using an ischemic threshold of less than or equal to 0.80, and to use pressure-wire fractional flow reserve (FFR ≤0.80) as the reference standard. Only studies providing sufficient information to reconstruct lesion-level diagnostic contingency tables (true positives, false positives, false negatives, and true negatives) were included. No eligible studies evaluating FFRangio or vFFR in the TAVI setting were identified during the systematic search. Studies focusing exclusively on prognostic outcomes without invasive physiological validation, those using non-hyperemic pressure ratios as the sole reference standard in the primary analysis, studies not clearly conducted in a TAVI pathway population, or those lacking extractable diagnostic data were excluded. When overlapping cohorts were identified, the most comprehensive dataset was retained. The unit of analysis was per-lesion.
Information sources and search strategy
A systematic search of PubMed (National Institutes of Health), Embase (Elsevier), and Web of Science (Clarivate) was performed from January 1, 2015, through April 2025. The search start date was chosen to coincide with the initial clinical validation of angiography-derived coronary physiology indices, as no studies applying these techniques in the TAVI setting were anticipated before this period. The search strategy combined terms related to angiography-derived coronary physiology and TAVI, including “quantitative flow ratio”, “QFR”, “μQFR”, “FFRangio”, “vFFR”, “angiography-derived FFR”, “wire-free physiology”, “aortic stenosis”, and “TAVI” or “TAVR.” No language restrictions were applied. Reference lists of eligible articles and relevant reviews were screened manually to identify additional studies. Two investigators independently screened titles, abstracts, and full texts for eligibility, with disagreements resolved by consensus.
Data extraction
Data were independently extracted by 2 reviewers using a standardized form. Extracted variables included study design, country, enrollment characteristics, lesion and angiographic characteristics, analyzability rates, index test details (including software platform when available), reference standard timing relative to TAVI, and hyperemia protocol when reported. Lesion-level diagnostic classification data were extracted directly when reported or reconstructed from published figures and diagnostic performance metrics when mathematically consistent and uniquely determined.
Outcome definitions
Primary outcome
The primary endpoint was the pooled sensitivity and specificity of pre-TAVI angiography-derived coronary physiology (≤0.80) for detecting functionally significant stenoses defined by a pre-TAVI FFR of less than or equal to 0.80. This analysis included only studies in which both the index test and reference standard were measured before TAVI.
Secondary outcomes
A prespecified secondary analysis evaluated the diagnostic accuracy of pre-TAVI angiography-derived physiology for predicting post-TAVI FFR-defined ischemia (FFR ≤0.80). This analysis was designed to explore the potential impact of severe aortic stenosis and its hemodynamic relief on invasive coronary physiology measurements.
Risk of rias assessment
Risk of bias and applicability were assessed using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS)-2 tool across the domains of patient selection, index test, reference standard, and flow and timing. Assessments were performed independently by 2 reviewers, with discrepancies resolved through consensus.
Statistical analysis
Diagnostic accuracy was synthesized using study-level 2×2 contingency data (true positives, false positives, false negatives, and true negatives). Sensitivity and specificity were pooled separately using random-effects models applied to logit-transformed proportions. Diagnostic odds ratios (DORs) were derived from pooled sensitivity and specificity. Likelihood ratios and post-test probabilities were also calculated (using standard methods) to translate pooled sensitivity and specificity into terms more directly applicable at the bedside. Additional global performance metrics, including balanced accuracy and Youden's index, were calculated to provide complementary measures of discriminatory performance. Given the absence of patient-level intraclass correlation coefficients in the original reports, adjustment for within-patient clustering was not feasible; this represents a recognized methodological limitation common to lesion-level diagnostic accuracy meta-analyses in interventional cardiology.
To evaluate whether diagnostic performance differed according to reference timing (pre- vs post-TAVI FFR), a meta-regression analysis was performed using reference timing as a study-level covariate. Interaction effects were assessed on the logarithmic scale of the DOR, and statistical significance was defined as a 2-sided P-value of less than 0.05. Given the limited number of eligible studies anticipated in this field, this analysis was considered exploratory and expected to be underpowered to detect modest interaction effects.
Prespecified sensitivity analyses included (1) leave-one-out influence analysis to assess the stability of pooled estimates; (2) exclusion of small studies, defined as those contributing fewer than 40 lesions, to evaluate the potential influence of small-cohort estimates on pooled results; (3) restriction to studies evaluating classical QFR, excluding those using Murray-law-based computational variants, to assess robustness across distinct algorithmic platforms; and (4) exclusion of studies performing angiography-derived computation from a single angiographic projection, to evaluate the potential impact of non-standard image acquisition on pooled diagnostic performance. All analyses were conducted using R (R Foundation for Statistical Computing). Study-level confidence intervals for sensitivity and specificity were calculated using the Wilson score method.
Results
Study selection
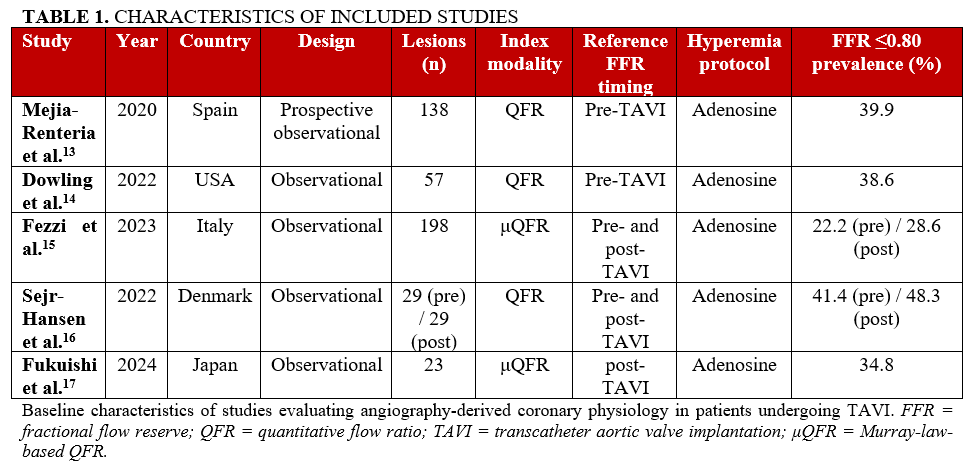
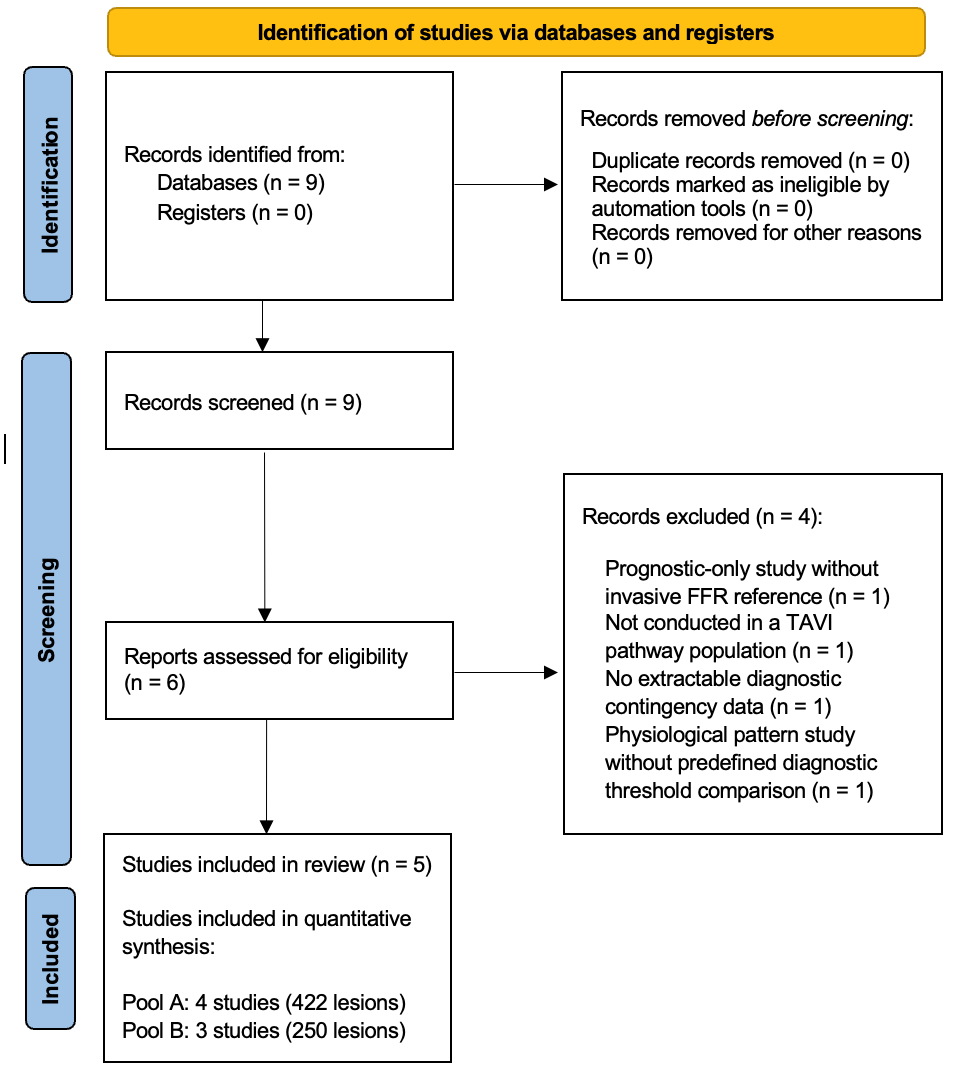
The systematic search identified 9 potentially eligible studies. After duplicate removal and screening of titles and abstracts, 6 full-text articles were assessed for eligibility. Four studies were excluded: 1 for absence of invasive FFR as reference standard, 1 for evaluation of borderline lesions outside a defined TAVI diagnostic pathway, 1 for lack of extractable lesion-level 2×2 diagnostic data, and 1 for analysis of physiological pattern changes without predefined diagnostic threshold comparison.9-12 Five studies met criteria for qualitative synthesis (Table 1). Four studies, comprising 422 lesions, contributed to the primary meta-analysis (pre-TAVI angiography-derived physiology vs pre-TAVI FFR),13-16 while 3 studies, comprising 250 lesions, contributed to the secondary analysis (pre-TAVI index vs post-TAVI FFR).15-17 One study contributed data to both analytical pools. The study selection process is detailed in Figure 1.
Study characteristics
All included studies were observational cohorts published between 2020 and 2024.13-17 Diagnostic assessment was performed at the lesion level. Sample sizes ranged from 29 to 198 lesions per study. All studies evaluated angiography-derived physiology using QFR or μQFR with a uniform ischemic threshold of less than or equal to 0.80. Invasive FFR (≤0.80) served as the reference standard in all analyses.
In the primary analytical pool, both index and reference measurements were performed prior to valve implantation during the same procedural session.13-16 In the secondary pool, invasive FFR was obtained after TAVI,15-17 introducing a physiologically distinct reference condition following relief of valvular obstruction. Across studies, the prevalence of FFR-defined functionally significant stenoses ranged from 22% to 41% in Pool A and from 25% to 48% in Pool B.
Primary analysis: pre-TAVI angiography-derived physiology vs pre-TAVI FFR (Pool A)
Across the 4 studies included in the primary analysis,13-16 a total of 128 lesions (30.3%) were classified as functionally significant by invasive FFR. The aggregated lesion-level totals were 103 true positives, 30 false positives, 25 false negatives, and 264 true negatives (Table 2, Figure 2A).
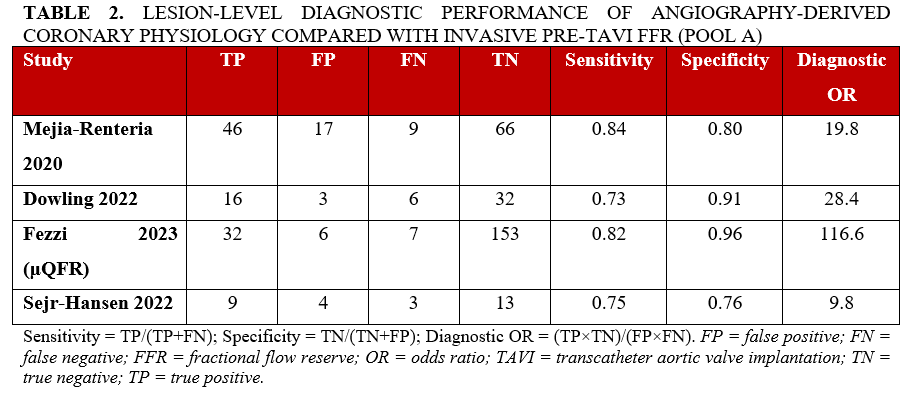
Using a random-effects model, pooled sensitivity was 0.79 (95% confidence interval [CI], 0.68-0.87) and pooled specificity was 0.88 (95% CI, 0.80-0.93). The corresponding DOR was 28. Derived likelihood ratios were positive (LR+) 6.6 and negative (LR–) 0.24. At a pretest probability of 30.3%, a positive test result increased the post-test probability of FFR-defined ischemia to 74.2%, whereas a negative test result reduced it to 9.4%. Study-level sensitivity and specificity estimates with corresponding Wilson CIs are presented in Supplemental Tables 1 and 2.
Secondary analysis: pre-TAVI angiography-derived physiology vs post-TAVI FFR (Pool B)
In the secondary analysis,15-17 72 of 250 lesions (28.8%) were classified as functionally significant by post-TAVI FFR. Aggregated lesion-level totals were 48 true positives, 7 false positives, 24 false negatives, and 171 true negatives (Table 3, Figure 2B).
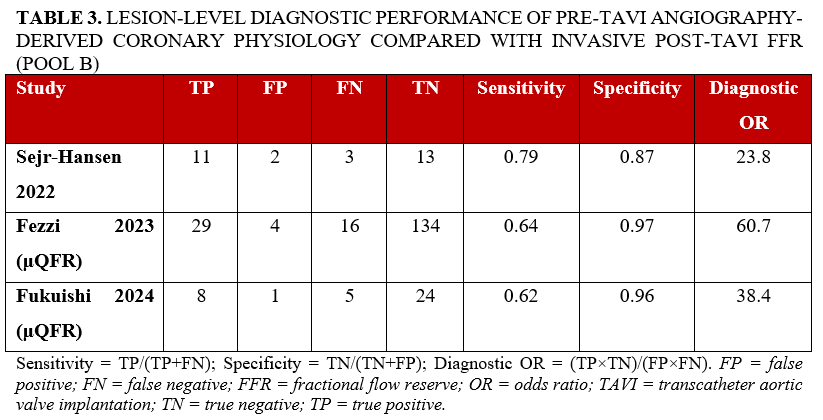
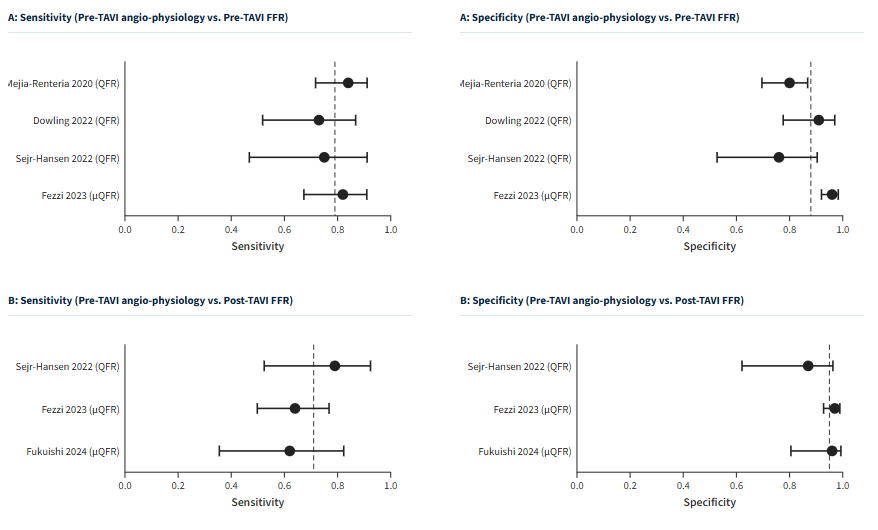
Random-effects pooling yielded a sensitivity of 0.71 (95% CI, 0.57-0.82) and a specificity of 0.95 (95% CI, 0.90-0.98). The pooled DOR was 46.5. Derived likelihood ratios were LR+ 14.2 and LR– 0.31. At a pretest probability of 28.8%, a positive test result increased the post-test probability of post-TAVI FFR-defined ischemia to 85.2%, whereas a negative test result reduced it to 11.1%. Individual study-level diagnostic estimates are detailed in Supplemental Tables 3 and 4. Compared with the primary analysis, specificity was higher whereas sensitivity was modestly lower when post-TAVI FFR served as the reference standard.
Comparative interpretation across hemodynamic states
Across both analytical conditions, pooled specificity remained high despite the transition from pre- to post-TAVI reference states (0.88 vs 0.95), whereas pooled sensitivity was numerically lower when post-TAVI FFR served as the reference (0.79 vs 0.71). The corresponding pooled DORs were 28 in Pool A and 46.5 in Pool B (Table 2). Balanced accuracy was similar across pools (0.84 vs 0.83), and Youden’s index remained comparable (0.67 vs 0.66), supporting consistent global discrimination.
In exploratory meta-regression analysis using reference timing (pre- vs post-TAVI FFR) as a study-level covariate, no statistically detectable modification was observed, although the analysis was underpowered (interaction effect on log DOR: β = 0.52 ± 0.61, P = .39). On the multiplicative scale, this corresponded to a relative DOR of 1.68 (95% CI, 0.51-5.56) for post- vs pre-TAVI reference timing.
Sensitivity analyses
Leave-one-out analyses demonstrated stability of pooled estimates, with sensitivity ranging from 0.77 to 0.82 and specificity varying by less than 0.02 across iterations, indicating that no single study exerted disproportionate influence on the pooled result. Exclusion of the smallest cohort (fewer than 40 lesions) increased pooled sensitivity from 0.79 to 0.82, while specificity remained unchanged. Restricting the analysis to classical QFR studies (excluding Murray-law-based μQFR) yielded pooled sensitivity of 0.79 and specificity of 0.87, consistent with the primary analysis, confirming robustness of pooled estimates across distinct computational platforms. Exclusion of the study performing angiography-derived computation from a single angiographic projection did not materially alter pooled sensitivity or specificity estimates.
Risk of bias
Risk of bias was assessed using the QUADAS-2 tool (Supplemental Table 5). The index test and reference standard domains were judged at low risk in all 5 included studies. In the patient selection domain, 2 studies were classified as low risk and 3 as having some concerns, primarily reflecting observational design and potential selection bias. In the flow and timing domain, 2 studies were judged at low risk and 3 studies as having some concerns, corresponding to cohorts in which post-TAVI FFR served as the reference standard, introducing temporal separation between index computation and invasive physiological measurement. No study was judged to be at high risk of bias in any domain.
Discussion
In this meta-analysis, we provide, for the first time in a focused quantitative synthesis, evidence regarding the diagnostic performance of angiography-derived (wire-free) coronary physiology in patients with severe aortic stenosis undergoing TAVI evaluation. The principal findings are threefold. First, angiography-derived physiology demonstrated great diagnostic accuracy when compared with invasive FFR measured prior to valve implantation, with pooled sensitivity of 0.79 (95% CI, 0.68-0.87) and specificity of 0.88 (95% CI, 0.80-0.93). Second, when post-TAVI FFR served as the reference standard, specificity increased to 0.95 (95% CI, 0.90-0.98) while sensitivity was numerically reduced to 0.71 (95% CI, 0.57-0.82), with overall global discriminatory capacity remaining comparable across both conditions (Youden index 0.67 vs 0.66). Third, exploratory meta-regression analysis did not demonstrate a statistically significant interaction between reference timing and overall diagnostic performance, although the absence of a statistically significant interaction should be interpreted cautiously given the limited number of studies and the lack of a stable reference standard across hemodynamic states. In practical terms, these data indicate that angiography-derived physiology may correctly identify roughly 4 in 5 functionally significant lesions and rule out roughly 9 in 10 non-significant lesions when performed before valve implantation, which is a performance in line with what interventional cardiologists already expect from QFR in non-TAVI populations.
Severe aortic stenosis is characterized by chronic pressure overload, altered coronary flow dynamics, and microvascular remodeling. These pathophysiologic changes have raised concerns regarding the reliability of pressure-wire–based physiological assessment in the pre-TAVI setting.3,18 Relief of valvular obstruction may modify coronary hemodynamics and potentially alter invasive FFR classification. Within this context, the present analysis suggests that angiography-derived physiology demonstrates comparable discriminatory performance when referenced to both pre- and post-TAVI FFR.
Notably, pooled specificity remained consistently high despite the transition from pre- to post-valve hemodynamic states, while sensitivity was numerically but not significantly lower when post-TAVI FFR served as the comparator, as reflected by widely overlapping confidence intervals and a non-significant meta-regression interaction. These findings suggest that angiography-derived physiology maintains comparable discriminatory performance relative to invasive FFR across different reference conditions and are consistent with recent pooled invasive physiology data demonstrating only modest post-TAVI changes in FFR values and high concordance between pre- and postprocedural measurements, despite stable microvascular resistance parameters.18
The observed pattern of simultaneously increasing specificity and numerically decreasing sensitivity when transitioning from pre- to post-TAVI FFR as the reference standard warrants mechanistic consideration. In the pre-TAVI hemodynamic state, reduced coronary perfusion pressure, elevated left ventricular end-diastolic pressure, and microvascular remodeling collectively lower FFR values, potentially classifying borderline lesions as hemodynamically significant. Following valve implantation, normalization of transvalvular gradients and restoration of coronary perfusion pressure unmask the true non-significance of these borderline lesions, reclassifying them from FFR-positive to FFR-negative. This reference standard reclassification effect simultaneously increases true negatives, thereby improving specificity, and increases false negatives for the pre-TAVI angiography-derived index, thereby numerically reducing sensitivity. Critically, this phenomenon likely reflects—at least in part—changes in the invasive reference standard following TAVI, rather than solely differences in index test performance, and is consistent with the non-significant meta-regression interaction observed across analytical pools.
The optimal timing of coronary physiological assessment in patients undergoing TAVI remains debated.2,3 Some operators advocate deferring physiological evaluation until after valve implantation to avoid potential confounding effects of severe stenosis-related hemodynamics. However, delaying coronary decision-making may complicate procedural planning and extend patient management pathways. Our findings suggest that angiography-derived physiology may be considered into pre-TAVI coronary evaluation. The preserved specificity and maintained global discriminatory capacity observed in this analysis indicate that wire-free physiological assessment performed prior to valve implantation provides clinically meaningful information without requiring postprocedural reassessment. High specificity across both hemodynamic conditions suggests that angiography-derived physiology may be particularly reliable for ruling-in functionally significant stenoses in the TAVI population. These data support consideration of a streamlined, single-stage diagnostic strategy in appropriately selected patients.
Previous individual studies have reported variable concordance between pre- and post-TAVI invasive physiology, reflecting the complex interplay between epicardial stenosis severity and microvascular adaptation in severe aortic stenosis.18 Individual study-level sensitivity estimates ranged from 0.62 to 0.84 and specificity from 0.76 to 0.97, reflecting cohort-level heterogeneity in lesion prevalence, angiographic acquisition protocols, and algorithmic platforms. By synthesizing available lesion-level data across cohorts, the present analysis provides a broader quantitative perspective and suggests that angiography-derived physiology demonstrates consistent performance within this evolving hemodynamic environment. Notably, the pooled specificity and DORs observed in the present analysis are consistent with or exceed those reported in individual studies, suggesting that lesion-level heterogeneity across cohorts does not materially impair the overall discriminatory performance of wire-free physiological assessment.
Importantly, this study focuses specifically on TAVI pathway populations and avoids extrapolation from mixed aortic stenosis cohorts. This TAVI-specific restriction enhances clinical relevance and provides a focused synthesis directly applicable to contemporary structural heart practice. In practice, these findings support incorporating angiography-derived physiology as an initial triage step during pre-TAVI angiographic assessment: lesions classified as non-significant (QFR/μQFR >0.80) can likely be deferred with reasonable confidence given high specificity, while positive results, particularly borderline ones, may still warrant invasive FFR confirmation given the more modest sensitivity. This staged approach could reduce pressure-wire use and procedural time without meaningfully increasing missed functionally significant disease
Future directions
Prospective studies incorporating paired pre- and post-TAVI invasive FFR measurements in the same lesions are needed to determine whether the observed sensitivity/specificity shift reflects true reclassification of lesion significance after relief of valvular obstruction, or measurement variability of the reference standard itself. Such studies should also evaluate whether a prospective outcomes trial of QFR-guided PCI within the TAVI pathway can safely streamline coronary decision-making without requiring postprocedural reassessment.
Limitations
Several limitations merit consideration. First, the number of included studies was modest and all were observational, risking confounding, selection bias, and publication bias against small negative studies. Second, analysis was performed at the lesion level without adjustment for within-patient clustering, which may overestimate precision, a limitation common to lesion-level diagnostic meta-analyses given the frequent absence of patient-level intraclass correlation coefficient data. Third, FFR-defined stenosis prevalence varied considerably across studies (22%-48%), which may introduce spectrum bias; pooled estimates should be interpreted within this range rather than applied uniformly. Fourth, 3 studies used classical QFR and 2 used μQFR, and one relied on single-view computation, which carries inherently lower reproducibility than dual-projection approaches, representing a source of variability not fully resolved by aggregate analysis, though sensitivity analyses restricting to classical QFR were consistent with the primary results. Fifth, the meta-regression on reference timing was exploratory and underpowered (5 studies); the non-significant interaction (P= .39) should be read as inconclusive rather than as evidence of equivalence, and the proposed mechanism, reclassification of borderline lesions after normalization of transvalvular gradients and perfusion pressure, remains physiologically plausible but speculative.
In addition, this study assessed diagnostic accuracy against an invasive FFR reference rather than clinical outcomes; whether physiology-guided decision-making improves long-term outcomes in TAVI patients remains to be established prospectively. Finally, all included studies used adenosine-induced hyperemia for invasive FFR, with no data available using instantaneous wave-free ratio (iFR) or other non-hyperemic indices; generalizability of these findings to iFR-based workflows, or to angiographic labs using reduced contrast volumes or single-view acquisition, may therefore be limited.
Conclusions
In patients with severe aortic stenosis undergoing TAVI evaluation, angiography-derived coronary physiology demonstrates good diagnostic performance compared with invasive FFR. Comparable overall discriminatory capacity was observed when referenced to both pre- and post-TAVI FFR, with no statistically significant interaction by FFR timing, although this analysis was underpowered and interpretation is limited by the absence of a stable reference standard across hemodynamic states. These findings support the consideration of wire-free physiological assessment as part of pre-TAVI coronary evaluation strategies. Prospective studies evaluating its clinical impact in the TAVI pathway are warranted.
Affiliations and Disclosures
From the 1Department of Cardiology, HFR - Fribourg Cantonal Hospital and University, Fribourg, Switzerland; 2Institut Cardiovasculaire Paris-Sud, Hôpital Jacques Cartier, Massy, France; 3Center for Coronary Artery Disease, Minneapolis Heart Institute and Minneapolis Heart Institute Foundation, Abbott Northwestern Hospital, Minneapolis, Minnesota; 4Department of Cardiology, Guy's and St Thomas' NHS Foundation Trust, Harefield Hospital, London, United Kingdom; 5Service of Cardiology, Geneva University Hospital, Geneva, Switzerland.
Disclosures: Dr Skalidis is supported by grant from the Gottfried and Julia Bangerter-Rhyner Foundation and from the Professor Dr Max Cloëtta Foundation. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Ioannis Skalidis, MD, PhD, Institut Cardiovasculaire Paris Sud, 6 Avenue du Noyer Lambert, Massy 91300, France. Email: Skalidis7@gmail.com
References
- Tomii D, Pilgrim T, Borger MA, et al. Aortic stenosis and coronary artery disease: decision-making between surgical and transcatheter management. Circulation. 2024;150(25):2046-2069. doi:10.1161/CIRCULATIONAHA.124.070502
- Kedhi E, Hermanides RS, Dambrink JE, et al; TCW study group. TransCatheter aortic valve implantation and fractional flow reserve-guided percutaneous coronary intervention versus conventional surgical aortic valve replacement and coronary bypass grafting for treatment of patients with aortic valve stenosis and complex or multivessel coronary disease (TCW): an international, multicentre, prospective, open-label, non-inferiority, randomised controlled trial. Lancet. 2025;404(10471):2593-2602. doi:10.1016/S0140-6736(24)02100-7
- Jørgensen TH, Engstrøm T, Jabbari R, et al. Fractional flow reserve to guide revascularization in patients with coronary artery disease undergoing TAVR. JACC Cardiovasc Interv. 2025;18(23):2925-2936. doi:10.1016/j.jcin.2025.10.015
- Pesarini G, Scarsini R, Zivelonghi C, et al. Functional assessment of coronary artery disease in patients undergoing transcatheter aortic valve implantation: influence of pressure overload on the evaluation of lesions severity. Circ Cardiovasc Interv. 2016;9(11):e004088. doi:10.1161/CIRCINTERVENTIONS.116.004088
- Minten L, McCutcheon K, Vanhaverbeke M, et al. Coronary physiological indexes to evaluate myocardial ischemia in patients with aortic stenosis undergoing valve replacement. JACC Cardiovasc Interv. 2025;18(2):201-212. doi:10.1016/j.jcin.2024.10.024
- Tsigkas G, Bozika M, Papafaklis MI, et al. Coronary angiography-based wire-free FFR methods. Hellenic J Cardiol. 2025:S1109-9666(25)00235-0. doi:10.1016/j.hjc.2025.10.004
- Salinas-Casanova JA, Jiménez-Franco VA, Jerjes-Sanchez C, et al. Diagnostic performance of quantitative flow ratio for the assessment of non-culprit lesions in myocardial infarction (QFR-OUTSMART): systematic review and meta-analysis. Catheter Cardiovasc Interv. 2025;105(2):308-320. doi:10.1002/ccd.31293
- Skalidis I, Noirclerc N, Meier D, et al. Head-to-head comparison of two angiography-derived fractional flow reserve techniques in patients with high-risk acute coronary syndrome: a multicenter prospective study. Int J Cardiol. 2024;399:131663. doi:10.1016/j.ijcard.2023.131663
- Demola P, Colaiori I, Bosi D, et al. Quantitative flow ratio-based outcomes in patients undergoing transcatheter aortic valve implantation quaestio study. Front Cardiovasc Med. 2023;10:1188644. doi:10.3389/fcvm.2023.1188644
- Kleczynski P, Dziewierz A, Rzeszutko L, Dudek D, Legutko J. Quantitative flow ratio for evaluation of borderline coronary lesions in patients with severe aortic stenosis. Rev Esp Cardiol (Engl Ed). 2022;75(6):472-478. doi:10.1016/j.rec.2021.04.008
- Zasada W, Mikołajczyk F, Jędrychowska M, et al. Comparison of FFR, iFR, and QFR assessment in patients with severe aortic stenosis and coronary heart disease. Postepy Kardiol Interwencyjnej. 2022;18(2):118-121. doi:10.5114/aic.2022.118527
- Fezzi S, Pesarini G, Flaim M, et al. Influence of physiological patterns of coronary disease on fractional flow reserve and instantaneous wave-free ratio changes in patients undergoing TAVI. Int J Cardiol. 2025;420:132761. doi:10.1016/j.ijcard.2024.132761
- Mejía-Rentería H, Nombela-Franco L, Paradis JM, et al; Collaborators. Angiography-based quantitative flow ratio versus fractional flow reserve in patients with coronary artery disease and severe aortic stenosis. EuroIntervention. 2020;16(4):e285-e292. doi:10.4244/EIJ-D-19-01001
- Dowling C, Michail M, Zhang JM, et al. Diagnostic performance of quantitative flow ratio, non-hyperaemic pressure indices and fractional flow reserve for the assessment of coronary lesions in severe aortic stenosis. Cardiovasc Diagn Ther. 2022;12(3):314-324. doi:10.21037/cdt-21-574
- Sejr-Hansen M, Christiansen EH, Ahmad Y, et al. Performance of quantitative flow ratio in patients with aortic stenosis undergoing transcatheter aortic valve implantation. Catheter Cardiovasc Interv. 2022;99(1):68-73. doi:10.1002/ccd.29518
- Fezzi S, Ding D, Scarsini R, et al. Integrated assessment of computational coronary physiology from a single angiographic view in patients undergoing TAVI. Circ Cardiovasc Interv. 2023;16(10):e013185. doi: 10.1161/CIRCINTERVENTIONS.123.013185
- Yuta F, Kawamori H, Toba T, et al. Diagnostic accuracy of Murray law-based quantitative flow ratio in patients with severe aortic stenosis undergoing transcatheter aortic valve replacement. Heart Vessels. 2024;39(8):735-745. doi:10.1007/s00380-024-02387-5
18. Gallinoro E, Scarsini R, Ancona MB, et al. Effect of TAVI on epicardial functional indices and their relationship to coronary microvascular function. Circ Cardiovasc Interv. 2025;18(6):e014940. doi:10.1161/CIRCINTERVENTIONS.124.014940













