

Severe Coronary Vasospasm Mimicking STEMI After Drug-Coated Balloon Angioplasty
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00129. Epub June 1, 2026.
A 54-year-old man with coronary artery disease with multiple prior percutaneous coronary interventions (PCI), hypertension, paroxysmal atrial fibrillation on apixaban, hyperlipidemia, prior cerebrovascular accident with residual right-sided hemiparesis, and active tobacco use presented with 1 hour onset of sudden severe substernal chest pain. Two weeks earlier, angiography had shown mild non-obstructive left anterior descending artery (LAD) and left circumflex artery (LCx) disease, 2 patent stents in the mid-right coronary artery (RCA) and patent ductus arteriosus (PDA) with 50% in-stent restenosis (ISR), and 80% stenosis between the stents at the proximal edge of the distal stent.
He underwent plain old balloon angioplasty followed by drug-coated balloon angioplasty for distal RCA ISR. On presentation, initial high-sensitivity troponin was less than 4 ng/L, which later rose to 86 ng/L. Initial electrocardiogram (ECG) showed anterolateral ST-segment elevation concerning for ST-segment elevation myocardial infarction (STEMI), but a repeat ECG shortly thereafter showed resolution despite persistent severe chest pain. He declined sublingual nitroglycerin because of prior intolerance.
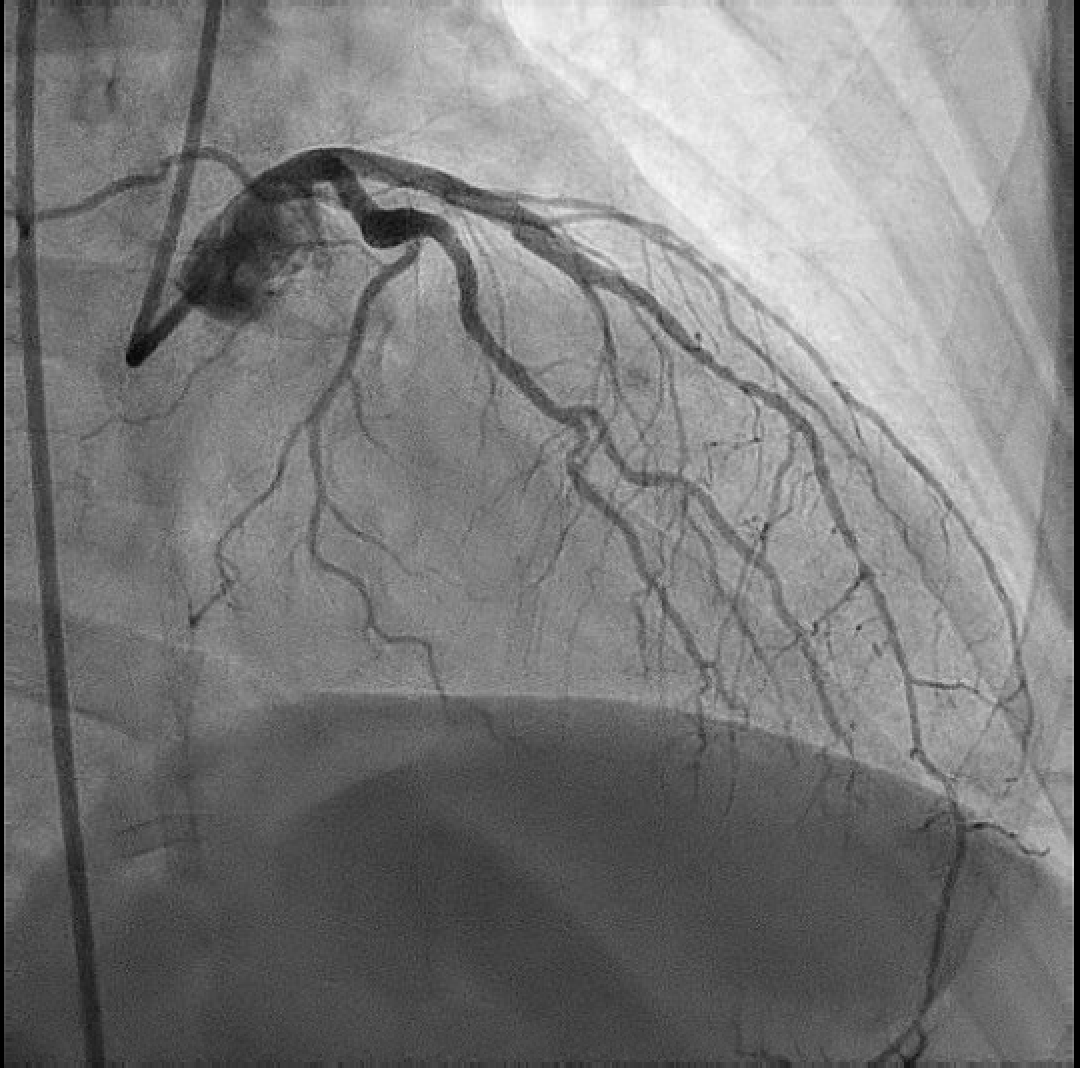
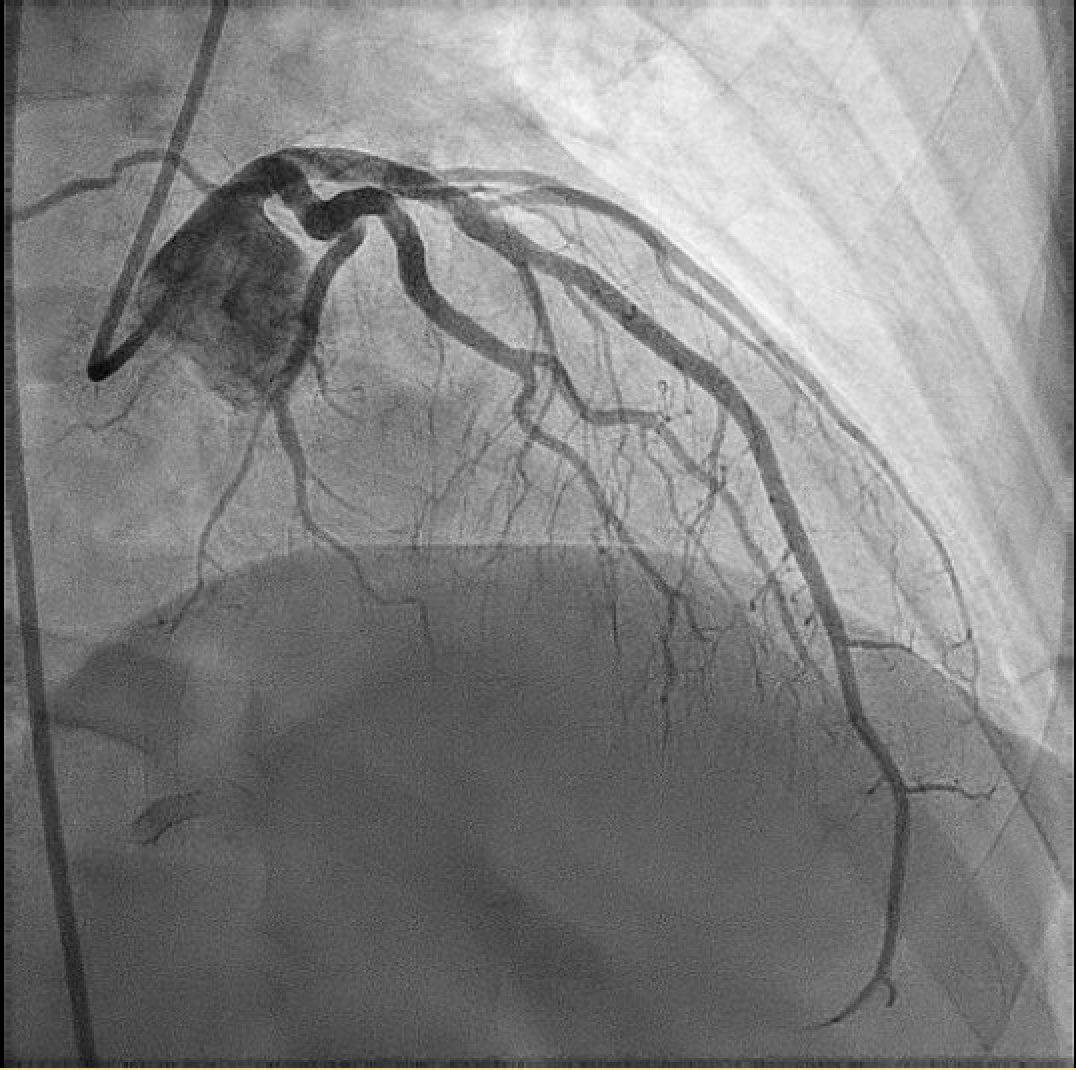
Given recent PCI, dynamic ECG changes, and ongoing pain, urgent repeat catheterization was performed. Angiography revealed diffuse sequential narrowing of the mid-to-distal LAD and a diagonal branch with a reversible “string-of-pearls” appearance (Figure 1, Video 1). The lesions improved dramatically after intracoronary nitroglycerin and adenosine, confirming severe coronary vasospasm rather than fixed obstructive disease (Figure 2, Video 2). Because of multisegmental involvement, vasculitis was considered. However, renal angiography showed smooth, non-tortuous vessels. Symptoms resolved by hospital day 2, and he was discharged on isosorbide mononitrate, ranolazine, and carvedilol.
This case highlights the potential role of procedure-related endothelial dysfunction in precipitating coronary vasospasm and the importance of considering coronary vasospasm as a STEMI mimic after recent PCI.
Affiliations and Disclosures
Kit Yee Chu, DO, PhD1; Zain Abidi, DO2; Ghassan Dalloul, MD, FACC2
From the Departments of 1Internal Medicine and 2Cardiology, Corewell Health Farmington Hills, Farmington Hills, Michigan.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and for the publication thereof, including any images.
Address for correspondence: Kit Yee Chu, DO, PhD, Department of Internal Medicine, Corewell Health Farmington Hills, Farmington Hills, MI 48336, USA. Email: Alice.chu@corewellhealth.org














