Left Ventricular Ejection Fraction Recovery Persists Beyond Six Months After Chronic Total Occlusion Percutaneous Intervention: Insights Across the Spectrum of Ischemic Cardiomyopathy
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00207. Epub July 7, 2026.
Chronic total occlusions (CTOs) are frequently encountered in ischemic cardiomyopathy with reduced left ventricular ejection fraction (LVEF).1 While CTO percutaneous coronary intervention (PCI) has been associated with LVEF improvement in heart failure with reduced ejection fraction (HFrEF), prior studies have largely been single-center and have not examined how baseline LV dysfunction severity influences recovery trajectory.2,3 The temporal impact of CTO PCI on LVEF recovery and association with hard outcomes remains poorly understood.4 We sought to examine LVEF recovery, all-cause mortality, and all-cause hospitalization following CTO PCI across 3 prespecified LVEF strata over prespecified periods of time in a large, real-world cohort of patients with cardiomyopathy.
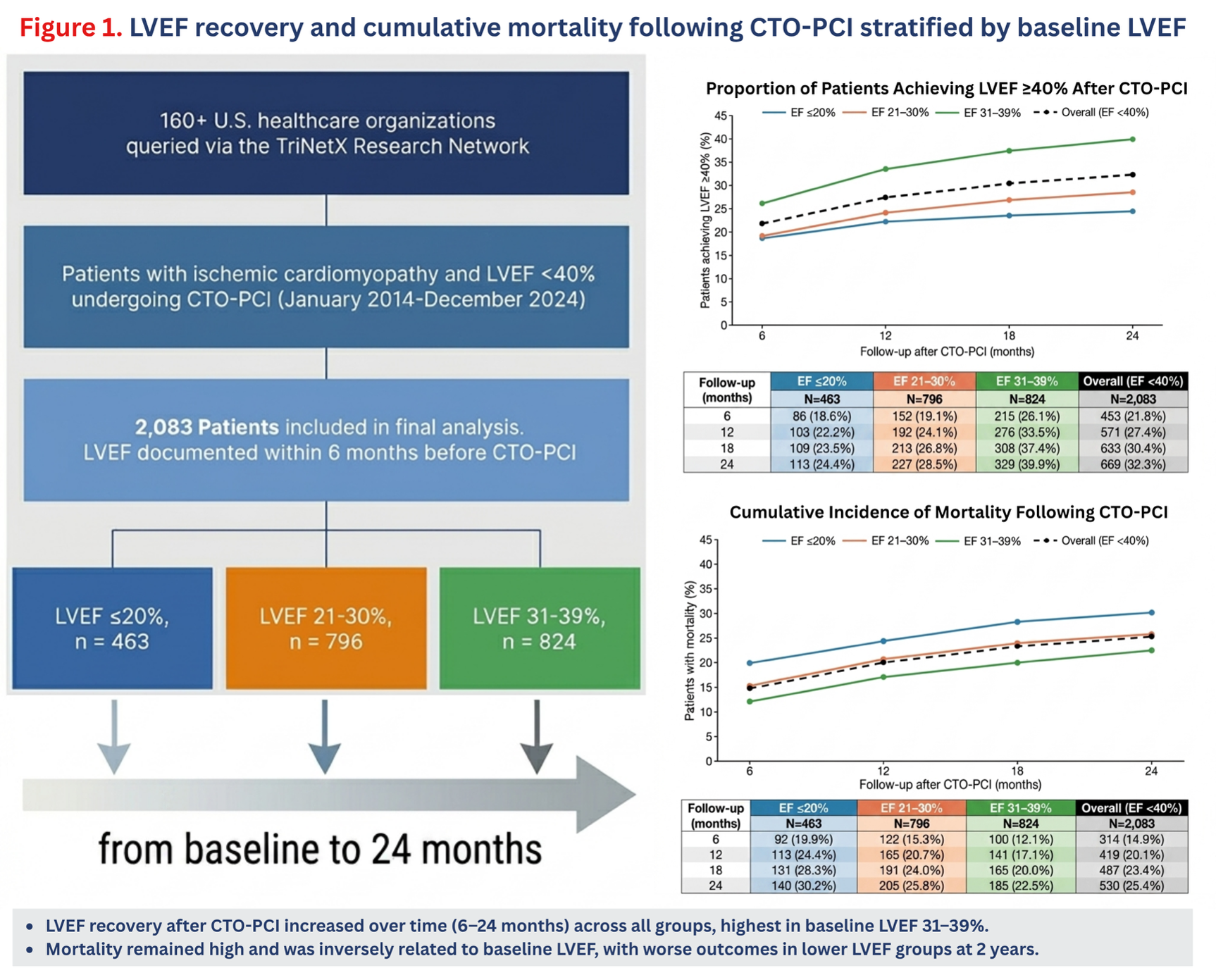
Through TriNetX, a federated electronic health record network of over 160 US healthcare organizations, we identified patients with ischemic cardiomyopathy who underwent CTO PCI between January 2014 and December 2024. CTO PCI was identified using Current Procedural Terminology (CPT) codes, and ischemic cardiomyopathy was defined using International Classification of Diseases, Tenth Revision (ICD-10) codes with a documented LVEF below 40% within 6 months before the procedure. Patients were stratified into 3 groups: LVEF less than or equal to 20%, LVEF from 21% to 30%, and LVEF from 31% to 39%. The primary outcome was LVEF recovery, defined as a documented LVEF of greater than or equal to 40% at 6, 12, 18, and 24 months post-procedure. Secondary outcomes included cumulative all-cause mortality and all-cause hospitalization at the same time points.
The study was performed in accordance with the Declaration of Helsinki. Ethical approval was not required for this human study because all patient data within the TriNetX is deidentified in accordance with the Health Insurance Portability and Accountability Act Privacy guideline. Thus, this study was exempt from institutional review board approval. Patient consent was not required as this study was based on publicly available data.
A total of 2083 patients met the inclusion criteria: 463 with an LVEF of less than or equal to 20%, 796 with an LVEF from 21% to 30%, and 824 with an LVEF from 31% to 39%. The mean age was 67 years, and 76.7% of patients were male. LVEF recovery increased over time across all groups from 6 to 24 months. In the lowest EF group (LVEF ≤20%), the mean LVEF was 29.01 ± 13.71, 29.09 ± 13.53, 29.20 ± 13.42, and 29.25 ± 13.62% at 6, 12, 18, and 24 months, with recovery rates of 18.6%, 22.2%, 23.5%, and 24.4%, respectively. Among patients in the mid-EF group (LVEF 21%-30%), the mean LVEF was 32.87 ± 11.94, 33.9 ± 11.94, 34.04 ± 12.75, and 34.21 ± 13.14%, with rates of 19.1%, 24.1%, 26.8%, and 28.5%, respectively. The highest recovery was seen in the highest EF group (LVEF 31%-39%), with a mean LVEF of 37.80 ± 11.74, 38.60 ± 12.30, 38.95 ± 12.26, and 39.36 ± 12.17%, and rates of 26.1%, 33.5%, 37.4%, and 39.9%, respectively. Overall, 32.3% of the entire cohort achieved an LVEF of greater than or equal to 40% by 24 months, with a mean LVEF of 34.89 ± 13.14%.
In our study, the higher EF tier (31%-39%) was associated with the highest recovery rate. There are multiple possible explanations. First, with significantly lower baseline LVEF, the likelihood of a predominantly nonischemic culprit of cardiomyopathy increases, and the presence of a CTO might be a bystander to the primary etiology. Second, in patients with myocardial scarring, which can be present in the CTO-supplied myocardial territories, recovery is unlikely.5 Finally, long-standing ischemic cardiomyopathy may lead to irreversible adverse remodeling, favoring earlier revascularization.
Our study showed continued recovery in LVEF. The percentage of patients who improved from 6 months to 24 months was 13.8% (35% of recovered patients) in the highest EF group (LVEF 31%-39%), 9.1% (32% of recovered patients) in the mid-EF group (LVEF 21%-30%), and 5.8% (25% of recovered patients) in the lowest EF group (LVEF <20%). This aligns with prior data showing delayed hibernating myocardium recovery extending up to 36 months post-revascularization,5 a critical consideration for trial design given that 25% to 35% of LVEF improvement occurs beyond 6 months.
Cumulative mortality was associated with baseline LVEF (Figure). At 24 months, mortality was 30.2% in the lowest EF group (LVEF ≤20%), 25.8% in the mid-EF group (LVEF 21%-30%), and 22.5% in the highest EF group (LVEF 31%-39%), with an overall 2-year mortality of 25.4%. This is in keeping with prior data showing that lower LVEF is independently associated with mortality in patients undergoing CTO PCI.4 The duration of LV dysfunction before the procedure was unavailable; longstanding, unrecognized cardiomyopathy with irreversible remodeling may partly explain the lower recovery rates and higher mortality in the group with an LVEF of less than or equal to 20%.
This study has several limitations. As a retrospective observational analysis, causality cannot be established. Technical success of CTO PCI, vessel territory, and procedural details were not available. The cause of death was not captured. LVEF documentation relied on available clinical records, and timing of assessment within the 6-month window may introduce variability. Prospective randomized data examining CTO PCI in ischemic cardiomyopathy stratified by severity of LV dysfunction are needed to confirm these findings.
In conclusion, among patients with ischemic cardiomyopathy undergoing CTO PCI, a significant proportion achieved LVEF recovery to greater than or equal to 40%, with rates rising progressively from 6 to 24 months across all LVEF strata. Recovery was greatest in those with an LVEF from 31% to 39%, though meaningful improvement was observed even with an LVEF of less than or equal to 20%. Mortality was inversely related to baseline LVEF and remained substantial at 2 years across all groups. These findings highlight baseline LVEF as an important predictor of outcomes after CTO PCI and support the need for prospective trials examining revascularization across the full spectrum of LV dysfunction.
Affiliations and Disclosures
Adham Ramadan, MD1; Mohamed Doma, MD2; Bryan Cogar, MD3; Kambis Mashayekhi, MD4; Margaret B. McEntegart, MD, PhD5; Khaldoon Alaswad, MD6; Gregor Leibundgut, MD7; Stephane Rinfret, MD8; Emmanouil S. Brilakis, MD, PhD9; Michael Megaly, MD, MS3
From 1Boston Medical Center, Boston, Massachusetts; 2Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts; 3Integris Baptist Medical Center, Oklahoma City, Oklahoma; 4Mediclin Heart Centre Lahr, Lahr, Germany; 5Columbia University Medical Center, New York, New York; 6Henry Ford Hospital, Detroit, Michigan; 7University Hospital Basel, Basel, Switzerland; 8Georgia Heart Institute/Northeast Georgia Health System, Gainesville, Georgia; 9Minneapolis Heart Institute and Minneapolis Heart Institute Foundation, Minneapolis, Minnesota.
Disclosures: Dr Mashayekhi receives consulting/speaker/proctoring honoraria from Abbott Vascular, Abiomed, ASAHI INTECC, AstraZeneca, Biotronik, Boston Scientific, Cardinal Health, Daiichi Sankyo, Medtronic, Shockwave Medical, Teleflex, and Terumo. Dr McEntegart receives consulting/speaker honoraria from Abbott Vascular, Biosensors, Boston Scientific, Medtronic, Shockwave Medical, and Teleflex. Dr Alaswad receives consulting/speaker honoraria from Boston Scientific and Teleflex. Dr Leibundgut receives consulting/speaker/proctoring honoraria from Johnson & Johnson, ASAHI INTECC, Novartis, Teleflex, Boston Scientific, Cordis, Terumo, B. Braun, and IMDS. Dr Rinfret serves as a consultant for Boston Scientific, Abiomed, Abbott Vascular, and SoundBite Medical Solutions. Dr Brilakis receives consulting/speaker honoraria from Abbott Vascular, the American Heart Association (associate editor, Circulation), Boston Scientific, the Cardiovascular Innovations Foundation (Board of Directors), Cordis, Elsevier, GE Healthcare, Heartflow, IMDS, Medtronic, Recor Medical, Shockwave, SIS Medical, Teleflex, and Terumo; research support from AngioWave, Boston Scientific, and GE Healthcare; is the owner of Hippocrates LLC and Systole LLC; and is a shareholder in Cleerly Health, LifeLens Technologies, Inc., MHI Ventures, Stallion Medical, and TrueVue, Inc. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Michael Megaly, MD, MS, Integris Baptist Medical Center, 3300 Northwest Expressway, Oklahoma City, OK 73112, USA. Email: michaelmegaly3@gmail.com; X: @MichaelMegalyMD, @AdhamGR97
References
1. Fefer P, Knudtson ML, Cheema AN, et al. Current perspectives on coronary chronic total occlusions: the Canadian Multicenter Chronic Total occlusions registry. J Am Coll Cardiol. 2012;59(11):991-997. doi:10.1016/j.jacc.2011.12.007
2. Megaly M, Zakhour S, Maki M, et al. Impact of chronic total occlusion PCI in Non-LAD coronary arteries on patients with cardiomyopathy. Am J Cardiol. 2025;249:9-15. doi:10.1016/j.amjcard.2025.04.004
3. Megaly M, Zakhour S, Karacsonyi J, et al. Outcomes of chronic total occlusion percutaneous coronary intervention of the left anterior descending artery. Am J Cardiol. 2023;193:75-82. doi:10.1016/j.amjcard.2023.01.049
4. Simsek B, Kostantinis S, Karacsonyi J, et al. Outcomes of chronic total occlusion percutaneous coronary intervention in patients with reduced left ventricular ejection fraction. Catheter Cardiovasc Interv. 2022;99(4):1059-1064. doi:10.1002/ccd.30097
5. Kirschbaum SW, Baks T, van den Ent M, et al. Evaluation of left ventricular function three years after percutaneous recanalization of chronic total coronary occlusions. Am J Cardiol. 2008;101(2):179-185. doi:10.1016/j.amjcard.2007.07.060