


A Contemporary Algorithm to Guide Percutaneous Coronary Intervention in High-Risk Spontaneous Coronary Artery Dissection
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Spontaneous coronary artery dissection (SCAD) is increasingly recognized as a cause of acute myocardial infarction, especially in women and young patients. The majority of SCAD cases can be managed conservatively, but failure to revascularize in the setting of reduced coronary flow, ongoing ischemia, or hemodynamic instability can result in extensive infarction, heart failure, or death. Higher complication rates have historically been reported with percutaneous coronary intervention in SCAD because of iatrogenic dissection, non-luminal wiring, and hematoma propagation. The authors propose an algorithm for managing cases of high-risk SCAD in the cardiac catheterization laboratory where intervention is required to restore coronary flow and limit the infarction. The methods described include options to recanalize the vessel with cutting balloons and strategies for non-luminal wire position.
Introduction
Once thought to be an uncommon condition, the prevalence of spontaneous coronary artery dissection (SCAD) in women younger than 50 years presenting with a myocardial infarction (MI) has been reported to be as high as 35%.1 The incidence of ST-elevation MI (STEMI)-SCAD in the Canadian SCAD Registry was 27.9% according to 2019 data.2 A detailed discussion of the etiology, diagnosis, and conservative management of SCAD is beyond the scope of this article and has been described elsewhere.1 Two alternative pathophysiological mechanisms underlying SCAD have been described in the past: the inside-out and the outside-in theories.3 The inside-out theory describes a tear in the intimal layer of the coronary artery with subsequent hematoma formation in the subintimal (SI) space causing luminal compromise. Currently, the outside-in phenomenon is thought to be the primary mechanism and occurs because of rupture of the vasa vasorum with hematoma formation in the arterial wall. This hematoma may then rupture into the true lumen.1
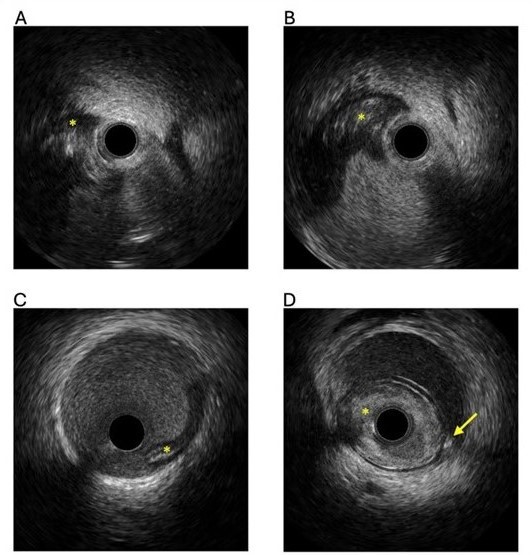
The diagnosis of SCAD is based on clinical presentation and the recognition of well-described patterns seen on coronary angiography. Intravascular imaging (Figure 1) can assist with diagnosis, but carries risk of extending the dissection. With improvement in resolution, coronary computed tomography angiography (CCTA) is increasingly being used, but coronary angiography remains the gold standard for SCAD diagnosis.
MANAGEMENT OF SCAD
Most SCAD cases can be managed conservatively, with the vessel healing over time. The 2021 American Heart Association/American College of Cardiology/Society of Cardiovascular Angiography and Intervention (AHA/ACC/SCAI) Guidelines recommend avoiding routine percutaneous coronary intervention (PCI) in the setting of SCAD unless there is hemodynamic instability or ongoing ischemia despite conservative treatment (2b indication).4 However, invasive management, most commonly with PCI, is sometimes required because of ongoing ischemia, ventricular arrhythmias, hemodynamic compromise, or shock. Failure to perform coronary revascularization in these situations can result in extensive infarction, heart failure, and, in some cases, death. The aims of PCI in this setting are to (1) restore and stabilize flow to the myocardium, (2) control and avoid extension of the dissected segment and hematoma, and (3) limit ischemia and infarction. The recently published 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline by Rao et al does not make specific recommendations for guideline-directed revascularization strategies in SCAD, which is a reflection of the challenges with the heterogeneity of this challenging condition.5 The 2023 ESC Guidelines give a 1c recommendation for PCI in SCAD with ongoing ischemia, a large area of myocardium at jeopardy, and reduced flow.6
ST-elevation is present in up to 50% of acute coronary syndrome (ACS) patients with SCAD.7 Despite this, PCI is less likely to be undertaken in ACS patients presenting with SCAD. In the Canadian SCAD Registry of 750 patients, only 14.1% underwent PCI. Lobo et al demonstrated similar findings, with STEMI-SCAD patients less likely to undergo acute revascularization (70% vs 97%).8 The medical management strategies of ACS in SCAD patients and discussion regarding the role of CCTA, antiplatelet agents, beta-blockers, and screening for fibromuscular dysplasia (FMD) are beyond the scope of this paper.
CORONARY REVASCULARIZATION FOR SCAD
Patients who undergo PCI for SCAD have similar, if not better, outcomes post-discharge compared with those managed conservatively.8,9 Alfonso et al compared outcomes of SCAD vs non-SCAD patients (n = 65 957) who underwent primary PCI between 2016 and 2020.10 Patients with SCAD (0.5%) were younger and more often female. In-hospital mortality and 30-day readmission rates were similar in both groups, supporting the use of primary PCI in selected SCAD patients. In SCAD patients who underwent stenting, longer stents were frequently used, with 1 study reporting a mean total stent length of 46 mm.11
Despite comparable clinical outcomes, PCI in SCAD has been associated with higher procedural complication rates and less favorable outcomes. While Hassan et al7 reported completely successful PCI in only 34.7% of STEMI-SCAD patients with 5.3% of cases requiring bail-out surgery, Lobo et al reported PCI success in 62%.8 The most common PCI-related complications are iatrogenic guide-catheter dissection, non-luminal wiring and/or ballooning, and propagation of the dissection or hematoma.12 Even if the initial stenting is successful, there is a risk of developing subsequent stent malapposition because of stent undersizing and hematoma resorption, which may increase the risk of stent failure.
Coronary artery bypass grafting (CABG) has been described in observational studies and case series as an option for patients with extensive SCAD with ongoing ischemia, left main stem (LMS) involvement, or unsuccessful PCI with ongoing ischemia. However, there is higher risk of acute graft closure, which has been reported in up to 30% of cases.13 Vein grafts are often preferred to preserve the left internal mammary artery conduit for potential later use. In extensive dissection, extended arteriotomy to treat the dissection and intraluminal hematoma has been reported.14 Patients who undergo CABG at their initial event are not protected against recurrent SCAD or the need for subsequent target vessel revascularization.13
PCI FOR SCAD: WHEN AND HOW?
PCI should be undertaken in SCAD patients with ongoing ischemia, high-risk anatomy (involvement of the LMS or proximal vessels), hemodynamic instability, or ventricular arrhythmias. Restoration of antegrade flow can be achieved with balloon dilatation, cutting balloon (CB) angioplasty, stenting, or re-entry techniques in the setting of non-luminal wiring.
We describe strategies to perform PCI in the setting of SCAD with a discussion on management of the SI space, decompressing hematoma, and assisting with re-entry to the true lumen. Generic PCI recommendations in all cases are the following:
1) Radial access is reasonable if operators are experienced in radial PCI. Early switch to femoral access is encouraged if guide engagement via radial access is challenging. Femoral access should be performed under ultrasound guidance because of the potential presence of FMD in the ileofemoral arteries.
2) Passive catheters are recommended, and catheters that are more likely to cause dissection, such as Amplatz Left guide catheters, should be avoided or used with care.
3) Limited antegrade contrast injections should be used when SCAD is suspected to reduce the risk of hydraulic extension of the dissection and hematoma.
4) The primary goal is to wire the distal true lumen and restore normal flow to the distal vessel. A non-hydrophilic workhorse guidewire with low tip load is preferred for wiring the true lumen, as it carries lower risk of entering and extending the dissection. The SUOH 03 wire (ASAHI INTECC) has a very low tip load (0.3 g) and was developed for tortuous collateral tracking during chronic total occlusion (CTO) PCI. Gasparini et al described successful use of the SUOH 03 wire in 92% of 75 cases with either iatrogenic or spontaneous vessel dissection.15 Signs of suboptimal wire position include resistance to guidewire advancement or the formation of a sigmoid/knuckle shape (appearing to “wrap” around the vessel architecture and propensity to form a knuckle), especially in non-atherosclerotic vessels. Conversely, easy guidewire advancement and entry into multiple side branches suggests true lumen position. Determining luminal vs SI guidewire position can be challenging in the presence of extensive dissections or pre-existing atheroma.16
5) Intravascular ultrasound (IVUS) should be used (if available) in cases of high-risk SCAD with a Thrombolysis in Myocardial Infarction (TIMI) flow of less than 3. IVUS will confirm the wire position (luminal/non-luminal), assess the extent of the dissection and hematoma, and allow accurate measurement of the vessel size to guide stent selection and balloon sizing (Figure 1). Optical coherence tomography (OCT) provides very helpful high-resolution images of SCAD in ambiguous lesions (Type 3 SCAD) and in distal SCAD with diagnostic uncertainty. Of note, OCT requires contrast injection that may create or propagate the dissection planes in very proximal SCAD with reduced flow. In 1 study of 65 patients with SCAD, 7.9% experienced an angiographic complication with OCT use.17 The optimal mode of intravascular imaging in SCAD has not been defined, but IVUS in high-risk cases (proximal SCAD with no flow) reduces the risk of extension of the dissection plane. Intravascular imaging has vital roles in the management of coronary artery disease and has IA level of evidence for the use in PCI in anatomically complex lesions, bifurcations, and long lesions.18 In CTO PCI, meta-analysis data has demonstrated reduced stent thrombosis with IVUS-guided vs angiographic-guided PCI.19
TREATMENT OPTIONS IF THE WIRE IS IN THE TRUE LUMEN
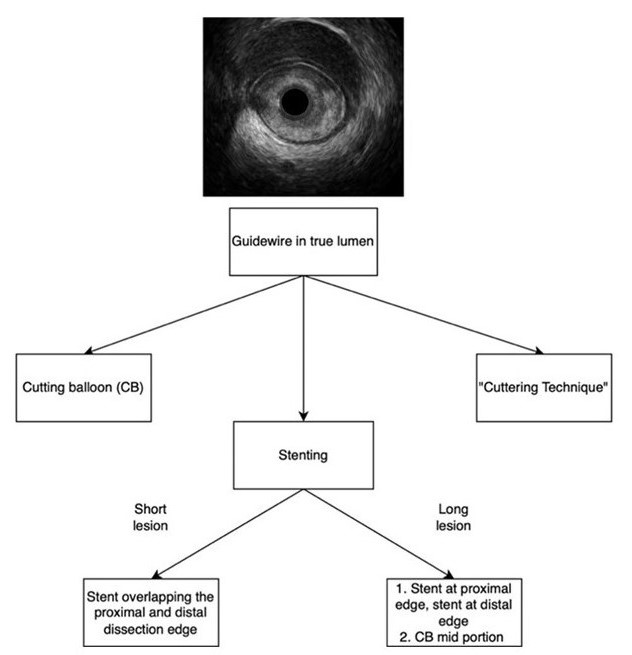
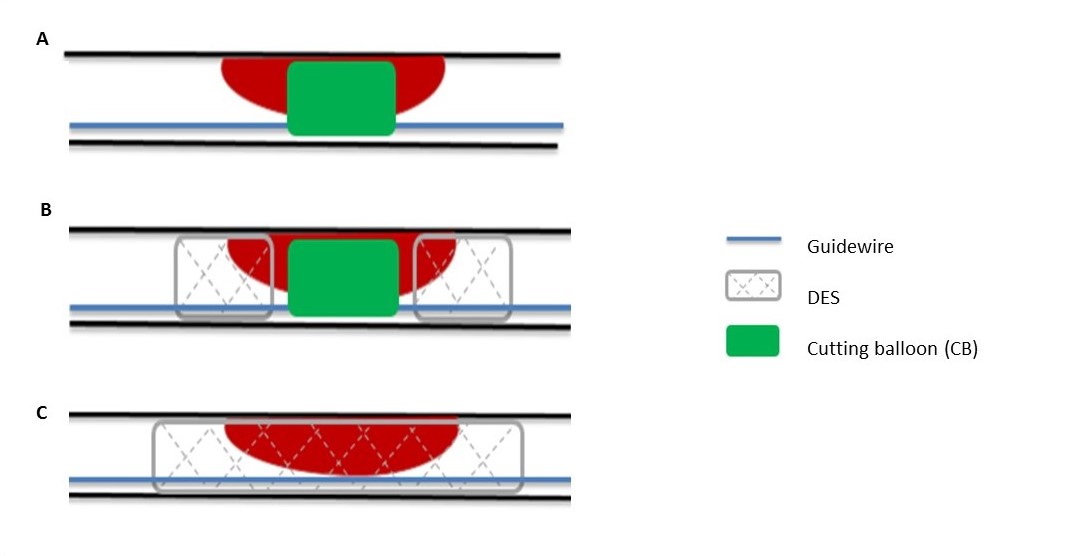
If distal vessel true lumen wiring (confirmed by IVUS if available) is achieved, options for restoration of flow include the following (Figures 2 and 3):
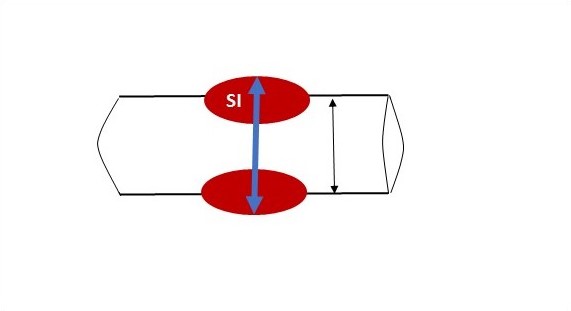
1) CBs: These devices have been successfully used to decompress iatrogenic SI hematomas during CTO PCI and in SCAD. Maricic et al reported restoration of TIMI-3 flow by CB use alone in 93.8% of 32 SCAD cases.20 By creating a fenestration in the intima, the CB can allow decompression of the hematoma, thus increasing the diameter of the previously compressed lumen and allowing restoration of flow (Figure 3A). In addition to resolving acute ischemia, this can also mitigate the later risk of stent malapposition once the hematoma has resolved. Consensus opinion has been to use low-pressure inflations to reduce the risk of vessel perforation. However, in some cases, low-pressure inflation may not be sufficient to create adequate fenestrations to achieve adequate decompression.18 Our recommendation is to use a CB sized 1:1 based on the lumen of the distal reference (on IVUS or angiogram) inflated to nominal pressure. However, in long segments of dissection/hematoma in tapering vessels, the CB may need to be sized based on an average measurement of the proximal and distal lumen (Figure 4).
2) “Cuttering Technique”: This is a recently described modification of the CB technique described by Gasparini et al.21 The CB is sized 1:1 to the reference vessel lumen, advanced to the maximum area of luminal compression, and inflated to nominal pressure. While inflated, it is carefully advanced along the dissection with small, controlled oscillating movements. The balloon can be deflated by 2 to 4 atm to facilitate further tracking. Successful “cuttering” is demonstrated by fenestrations on IVUS or the resolution of contrast staining on angiography. A second wire can be placed in the aorta to stabilize the guide and reduce the risk of inadvertent guide intubation, which may occur when trying to advance a bulkier CB.
3) Stenting: When CB use and hematoma decompression alone do not restore flow, or in very proximal lesions with concern for retrograde dissection extension to the left main or the aorta, stenting can be used. Stents should be sized 1:1 with the reference vessel lumen (in a similar approach to CB sizing). Undersized stents increase the risk of malapposition and stent failure when the hematoma resorbs. In long segments of SCAD, shorter stents can be deployed to cover the proximal and distal ends of the dissection, with the section in between decompressed with a CB (Figure 3B). Stenting of the entire SCAD segment can be done with the stent extending beyond the proximal and distal edges of the dissection (Figure 3C). Balloon predilatation should be avoided in SCAD to avoid extension of the dissection. Similarly, high-pressure post-dilation should not be performed to avoid propagation or expansion of intramural hematoma. If hematoma decompression is not performed or is unsuccessful, implantation of a stent can result in significant underexpansion, which cannot be resolved and may even be exacerbated by post-dilation. There are reports of successful drug-coated balloon (DCB) use in SCAD PCI, but the data is limited, and there is not a sound rationale for their use.22
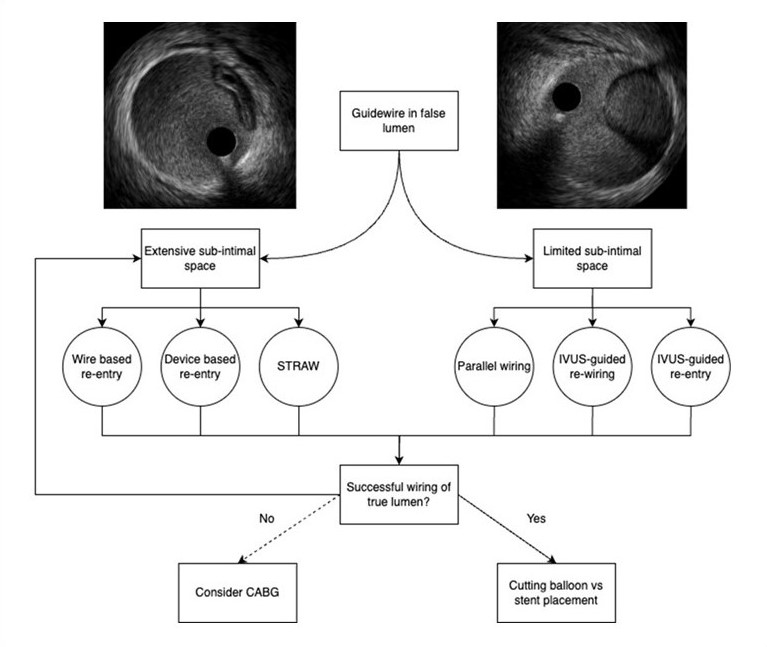
TREATMENT OPTIONS IF THE WIRE IS IN THE FALSE LUMEN
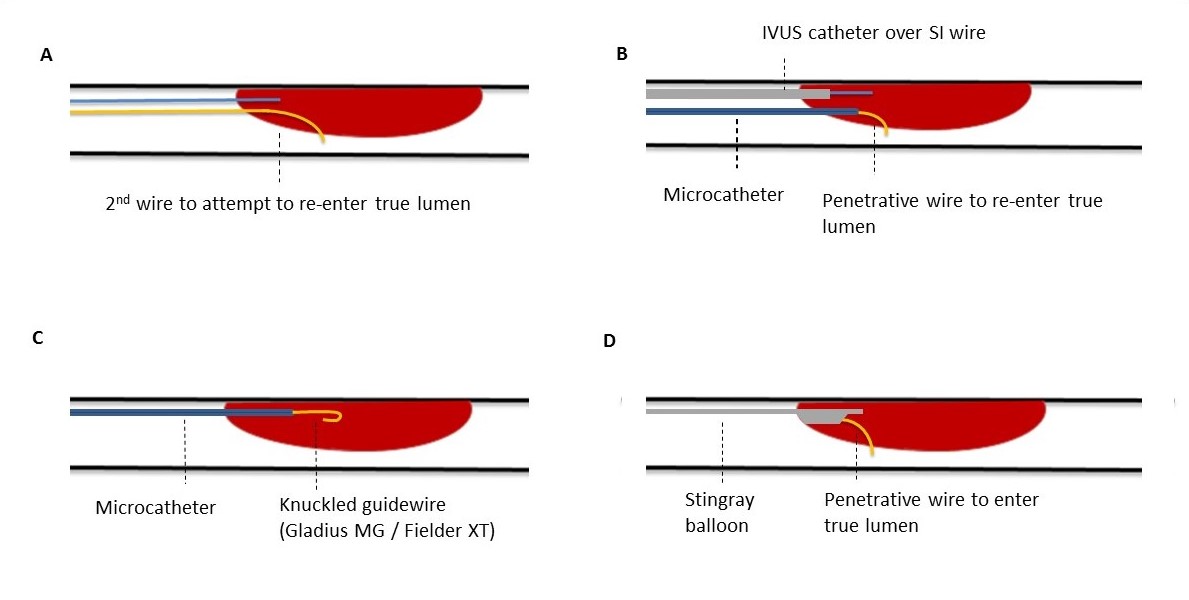
If the guidewire enters the false lumen, several well-described CTO PCI strategies can be used for true lumen re-entry (Figure 5 and 6). It is important to note that these techniques are extrapolated from CTO PCI, and the successful use of the techniques described below in SCAD is based on case reports and the personal experience of the authors.
1) Parallel-wiring: The initial wire is left in place as a marker of the false lumen followed by manipulation of a second wire, workhorse wire, or moderately penetration directional guidewire (eg, Gaia [ASAHI INTECC]) over a single- or dual-lumen microcatheter to access the true lumen (Figure 6A).
2) IVUS-guided rewiring or re-entry: An IVUS catheter is advanced into the SI space over the initial guidewire and is used to either (a) guide a second guidewire into the true lumen or (b) re-enter into the true lumen. Real-time IVUS supports the former by defining the proximal entry of the dissection and demonstrating true lumen entry without contrast injections. This is often done with a low tip load wire, but occasionally jacketed wires and dual lumen or angled microcatheters may be advantageous in accessing an eccentric tract. A wire with high penetration force (eg, Gaia Next 3 [ASAHI INTECC] or Conquest Pro 12 [ASAHI INTECC]) is usually used for re-entry (Figure 6B) to cross the dissection plane into the true lumen. Re-entry can be hindered by the presence of a large SI hematoma: using the SI transcatheter withdrawal (“STRAW technique”) can be helpful to re-expand the luminal target.23 A microcatheter is advanced over the wire in the false lumen, the wire is removed, and then blood is aspirated from the false lumen while withdrawing the microcatheter slowly to a more proximal position. Blocking the inflow to the SI space with a balloon or guide extension is important because, if there is significant inflow, the SI hematoma will reaccumulate. STRAW requires an adjunctive technique for re-entry and is not itself a definitive treatment.
3) Wire-based re-entry with STAR (Subintimal Tracking and Re-entry): a polymer-jacketed guidewire is knuckled and advanced distally until it hopefully re-enters into the true lumen (Figure 6C). The Gladius MG wire (ASAHI INTECC) and soft, polymer-jacketed wires, such as the Fielder XT (ASAHI INTECC), are the most commonly used for knuckling. Re-entry most commonly occurs at bifurcations; however, it is unpredictable. Observing a decrease in the knuckle size during wire advancement usually signifies true lumen re-entry. Very distal advancement should be avoided to limit propagation of the dissection beyond significant side branches and reduce the risk of perforation. After successful re-entry, a small balloon should be inflated at the re-entry site to improve antegrade flow. Unlike IVUS-guided rewiring or re-entry, which have significant learning curves, STAR can be successfully taught and performed by non-CTO operators.
A variation of this approach, known as the “mini-STAR” technique, employs a smaller dissection plane and softer, low-penetration force wires to facilitate controlled re-entry while minimizing propagation of the dissection. Unlike conventional STAR, which typically relies on stiffer wires and creates a broader SI track, mini-STAR aims to reduce trauma to the vessel wall. This technique may be especially advantageous in SCAD cases where vessel fragility is pronounced, and extensive dissection must be avoided. This has been used successfully in SCAD cases.24
4) Device-based re-entry: The Stingray balloon (Boston Scientific) is a flat, over-the-wire balloon with 2 side exit ports that was developed specifically for re-entry from the SI space into the true lumen during CTO PCI (Figure 6D). It has been successfully used in cases of high-risk SCAD along with the STRAW technique to aspirate hematoma and facilitate re-entry into the true lumen.24
Once the true lumen is re-entered, options to restore flow to the distal vessel are CB inflation (or semi-compliant balloon if a CB is not available), proximal and distal edge stenting with fenestration of the mid-section, or full stent coverage as described earlier in the text.
The aim of these algorithms is to reduce the complication rate of PCI in SCAD, preserve as much myocardium as possible, and avoid stent undersizing with the associated risk of stent failure. We also aim to generate discussion on how, as a speciality, we can standardize our PCI approach and strategy in high-risk SCAD.
CONCLUSIONS
SCAD is an increasingly recognized cause of ACS, especially in young women. While conservative management is preferred in most patients, coronary revascularization is sometimes required in cases of ongoing ischemia, hemodynamic instability, proximal vessel involvement, or left main dissection. We have described pragmatic strategies that can be undertaken by interventional cardiologists when managing a SCAD patient with a high-risk clinical presentation in the cardiac catheterization lab. These strategies include guidewire selection, steps for CB use, the important role of IVUS, techniques to re-enter the true lumen, and modification of the SI space. Of note, the algorithms described in this document are based on expert opinion and case experience and are not validated in guidelines. The aim is to provide guidance on how to optimize the success of coronary revascularization in this high-risk cohort of patients who may otherwise be at risk of extensive infarction. A prospective, multicenter study to validate this algorithm and standardize the approach to PCI in SCAD would be a welcome next step for the cardiology community and our patients.
Affiliations and Disclosures
Sarah L. Fairley, PhD1; Emmanouil S. Brilakis, PhD2; Kathleen E. Kearney, MD3; Jacqueline Saw, MD4; Margaret B. McEntegart, MD5; Sarah J. Zaman, PhD6; Matthew D. Hordern, MBBS, PhD1; Patrick Pender, MD6; Shauna L. Newton, MD3; Scott A. Harding, MD1
From the 1Cardiology Department, Wellington Hospital, Riddiford St, Wellington, New Zealand; 2Minneapolis Heart Institute, Minnesota; 3Cardiology Department, University of Washington, Seattle, Washington; 4Division of Cardiology, University of British Columbia, Vancouver, British Columbia, Canada; 5Columbia University Irving Medical Centre, New York, New York; 6Westmead Applied Research Centre, University of Sydney, Sydney, Australia.
Disclosures: Dr Brilakis receives consulting/speaker honoraria from Abbott Vascular, the American Heart Association (associate editor, Circulation), Biotronik, Boston Scientific, Cardiovascular Innovations Foundation (Board of Directors), Cordis, CSI, Elsevier, GE Healthcare, Haemonetics, IMDS, Medtronic, SIS Medical, Teleflex, and Orbus Neich; research support from Boston Scientific and GE Healthcare; is the owner of Hippocrates LLC; and is a shareholder in LifeLens Technologies, Inc., MHI Ventures, Cleerly Health, Stallion Medical, and TrueVue, Inc. Dr Kearney receives consulting/honoraria from Abbott, Boston Scientific, Medtronic, Teleflex, ASAHI INTECC, and Philips Vascular. Dr Saw receives unrestricted research grant support from the Canadian Institutes of Health Research, the Heart & Stroke Foundation of Canada, the National Institutes of Health, the University of British Columbia Division of Cardiology, AstraZeneca, Abbott, Boston Scientific, and Servier; salary support from the Michael Smith Foundation of Health Research; speaker honoraria from AstraZeneca, Abbott, Boston Scientific, and Sunovion; consultancy and advisory board honoraria from AstraZeneca, Abbott, Boston Scientific, Baylis, Gore, and FEops; and proctorship honoraria from Abbott and Boston Scientific. Dr Harding receives grant/research support from ASAHI INTECC; proctoring fees/speaker honoraria from Boston Scientific, Abbott Vascular, Terumo Medical, Bio-Excel, Teleflex, and Getz Medical; and is a shareholder in Seigla Medical. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Sarah L. Fairley, Cardiology Department, Wellington Hospital, Riddiford St, Wellington 6021, NZ. Email: Sarah.Fairley@ccdhb.org.nz; X: @SarahFairley7
References
1. Dang Q, Burgess S, Psaltis PJ, Fairley S, Saw J, Zaman S. Spontaneous coronary artery dissection: a clinically oriented narrative review. NPJ Cardiovasc Dis. 2024;1(1):4. doi:10.1038/s44325-024-00004-y
2. Saw J, Starovoytov A, Humphries K, et al. Canadian spontaneous coronary artery dissection cohort study: in-hospital and 30-day outcomes. Eur Heart J. 2019;40(15):1188-1197. doi:10.1093/eurheartj/ehz007
3. Hayes SN, Kim ESH, Saw J, et al; American Heart Association Council on Peripheral Vascular Disease; Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Genomic and Precision Medicine; and Stroke Council. Spontaneous coronary artery dissection: current state of the science: a scientific statement from the American Heart Association. Circulation. 2018;137(19):e523-e557. doi:10.1161/CIR.0000000000000564
4. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(3):e18-e114. doi:10.1161/CIR.0000000000001038
5. Rao SV, O’Donoghue ML, Ruel M, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI guideline for the management of patients with acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2025;151(13):e771-e862. doi:10.1161/CIR.0000000000001309
6. Byrne RA, Rosselló X, Coughlan JJ, et al; ESC Scientific Document Group. 2023 ESC guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44(38):3720-3826. doi:10.1093/eurheartj/ehad191
7. Hassan S, Samuel R, Starovoytov A, Lee C, Aymong E, Saw J. Outcomes of percutaneous coronary intervention in patients with spontaneous coronary artery dissection. J Interv Cardiol. 2021;2021:6686230. doi:10.1155/2021/6686230
8. Lobo AS, Cantu SM, Sharkey SW, et al. Revascularization in patients with spontaneous coronary artery dissection and ST-segment elevation myocardial infarction. J Am Coll Cardiol. 2019;74(10):1290-1300. doi:10.1016/j.jacc.2019.06.065
9. Saw J, Starovoytov A, Aymong E, et al. Canadian spontaneous coronary artery dissection cohort study: 3-year outcomes. J Am Coll Cardiol. 2022;80(17):1585-1597. doi:10.1016/j.jacc.2022.08.759
10. Alfonso F, Fernández-Pérez C, del Prado N, et al. Primary percutaneous coronary intervention in patients with spontaneous coronary artery dissection vs coronary artery disease. JACC Cardiovasc Interv. 2023;16(15):1860-1869. doi:10.1016/j.jcin.2023.05.044
11. Kotecha D, Garcia-Guimaraes M, Premawardhana D, et al. Risks and benefits of percutaneous coronary intervention in spontaneous coronary artery dissection. Heart. 2021;107(17):1398-1406. doi:10.1136/heartjnl-2020-318914
12. Fahey JK, Chew A, Ihdayhid AR, et al. Women with spontaneous coronary artery dissection are at increased risk of iatrogenic coronary artery dissection. Heart Lung Circ. 2021;30:e23-e28. doi:10.1016/j.hlc.2020.11.009
13. Tweet MS, Eleid MF, Best PJM, et al. Spontaneous coronary artery dissection: revascularization versus conservative therapy. Circ Cardiovasc Interv. 2014;7(6):777-786. doi:10.1161/CIRCINTERVENTIONS.114.001659
14. O'Sullivan KE, Tong MZ, Weiss AJ, Bakaeen FG. Extensive spontaneous coronary artery dissection associated with thrombosis: a surgical challenge. JACC Case Rep. 2023;10:101752. doi:10.1016/j.jaccas.2023.101752
15. Gasparini GL, Bollati M, Chiarito M, et al. SUOH 03 guidewire for the management of coronary artery dissection: insights from a multicenter registry. J Interv Cardiol. 2023;2023:7958808. doi:10.1155/2023/7958808
16. Harding SA, Fairley SL. Catheter-induced coronary dissection: keep calm and don’t inject. JACC Case Rep. 2019;1(2):113-115. doi:10.1016/j.jaccas.2019.07.002
17. Jackson R, Al-Hussaini A, Joseph S, et al. Spontaneous coronary artery dissection: pathophysiological insights from optical coherence tomography. JACC Cardiovasc Imaging. 2019;12(12):2475-2488. doi:10.1016/j.jcmg.2019.01.015
18. Vrints C, Andreotti F, Koskinas KC, et al; ESC Scientific Document Group. 2024 ESC guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024;45(36):3415-3537. doi:10.1093/eurheartj/ehae177
19. Panuccio G, Abdelwahed YS, Carabetta N, et al. Clinical and procedural outcomes of IVUS-guided vs angiography-guided CTO-PCI: a systematic review and meta-analysis. J Clin Med. 2023;12(15):4947. doi:10.3390/jcm12154947
20. Maričić B, Perišić Z, Kostić T, et al. An analysis of published cases of cutting balloon use in spontaneous coronary artery dissection. Front Cardiovasc Med. 2023;9:1270530. doi:10.3389/fcvm.2023.1270530
21. Gaspirini GL, Maurina M, Regazzoli D, et al. The “cuttering (cutting-dottering balloon) technique” for treatment of flow-limiting coronary intramural hematoma. Catheter Cardiovasc Interv. 2024;104(5):952-958. doi:10.1002/ccd.31231
22. Wu S, Liu W, Zhao Y, et al. Revascularization treatment for spontaneous coronary artery dissection: a reconsideration of drug-coated balloons and bioresorbable vascular scaffold. Int J Cardiol. 2016;209:49-50. doi:10.1016/j.ijcard.2016.02.059
23. Matsuura S, Otowa K, Maruyama M, Usuda K. Successful revascularization with percutaneous coronary intervention using a combination of the subintimal transcatheter withdrawal technique and coronary artery fenestration for spontaneous coronary artery dissection. Clin Case Rep. 2021;9(11):e05045. doi:10.1002/ccr3.5045
24. Daniels DV, Pargaonkar VS, Nishi T, Tremmel JA. Antegrade dissection re-entry after subintimal wiring of an occluded vessel from spontaneous coronary artery dissection. JACC Case Rep. 2020;2(1):72-76. doi:10.1016/j.jaccas.2019.12.001
