



Diffuse Large B-Cell Lymphoma of the Axilla Clinically Mimicking Hidradenitis Suppurativa
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Hidradenitis suppurativa (HS) is a chronic inflammatory disease that primarily affects intertriginous areas. Its heterogeneous and sometimes nonspecific presentation can lead to diagnostic uncertainty, particularly in unilateral, treatment-resistant lesions. Cutaneous lymphomas, although rare, may mimic HS both clinically and radiologically, leading to delays in appropriate diagnosis and therapy. Case Report. A 60-year-old male presented with a 7-month history of a painful, draining axillary lesion that was initially managed as HS. Despite prolonged antibiotic and intralesional corticosteroid treatment, the lesion progressed, with increasing edema and limited arm and hand mobility. Magnetic resonance imaging revealed a multilobular mass with necrosis and matted lymph nodes. Histopathologic examination of a punch biopsy identified diffuse large B-cell lymphoma, not otherwise specified, germinal center B-cell subtype. Due to reduced ejection fraction from recent myocardial infarction, rituximab monotherapy was initiated, resulting in clinical improvement. Wound necrosis was managed with negative pressure wound therapy. Conclusion. This case highlights the critical need to consider lymphomas in the differential diagnosis of atypical or refractory HS-like presentations. Prompt histopathologic evaluation in such cases enables accurate diagnosis and timely initiation of appropriate oncologic treatment, which ultimately may lead to improved patient outcomes.
Hidradenitis suppurativa (HS) is a chronic inflammatory disease characterized by inflammatory nodules, sinus tract formation, and scarring, especially of the axillary, inguinal, and inframammary areas and buttocks.1 The disease manifests to varying degrees, ranging from mild localized cases to severe generalized involvement.2 Existing literature emphasizes the need to consider cutaneous malignancies in the differential diagnosis, especially in cases featuring unilateral, treatment-resistant lesions.3-5 The present report details a case that was initially misdiagnosed as HS but was ultimately recognized as diffuse large B-cell lymphoma (DLBCL).
Case Presentation
A 60-year-old male presented to the dermatology department with painful, erythematous, draining lesions in the left axilla that had persisted for approximately 7 months (Figure 1). The lesions had gradually enlarged over time, prompting the patient to seek care from his primary physician, followed by several consultations at general surgery clinics. At the time of presentation, the patient exhibited weight loss over the preceding 3 months, which was attributed to a recent myocardial infarction.

The initial ultrasonographic examination revealed irregular, hypoechoic collections accompanied by surrounding edema, indicating the presence of a subcutaneous abscess. Despite receiving several topical antiseptics and antibiotics combined with multiple courses of prolonged oral antibiotics (eg, doxycycline), the patient reported persistent symptoms. He was hospitalized to receive parenteral antibiotics, including ampicillin-sulbactam, for 1 week, along with intralesional corticosteroid injections. The lesion worsened, with progressive edema, limited arm and hand mobility, and persistent drainage. The antibiotic regimen was switched to cefoperazone-sulbactam and linezolid, but the patient’s condition continued to deteriorate.
Laboratory tests were performed to exclude infection. Results of bacterial tissue cultures, fungal cultures, mycobacterial cultures, mycobacterial polymerase chain reaction, and acid-fast bacilli staining were negative. Magnetic resonance imaging (MRI) identified a multilobular mass with central necrosis and multiple matted lymph nodes. The mass extended into the skin and subcutaneous tissue but did not invade the bone or muscle structures.
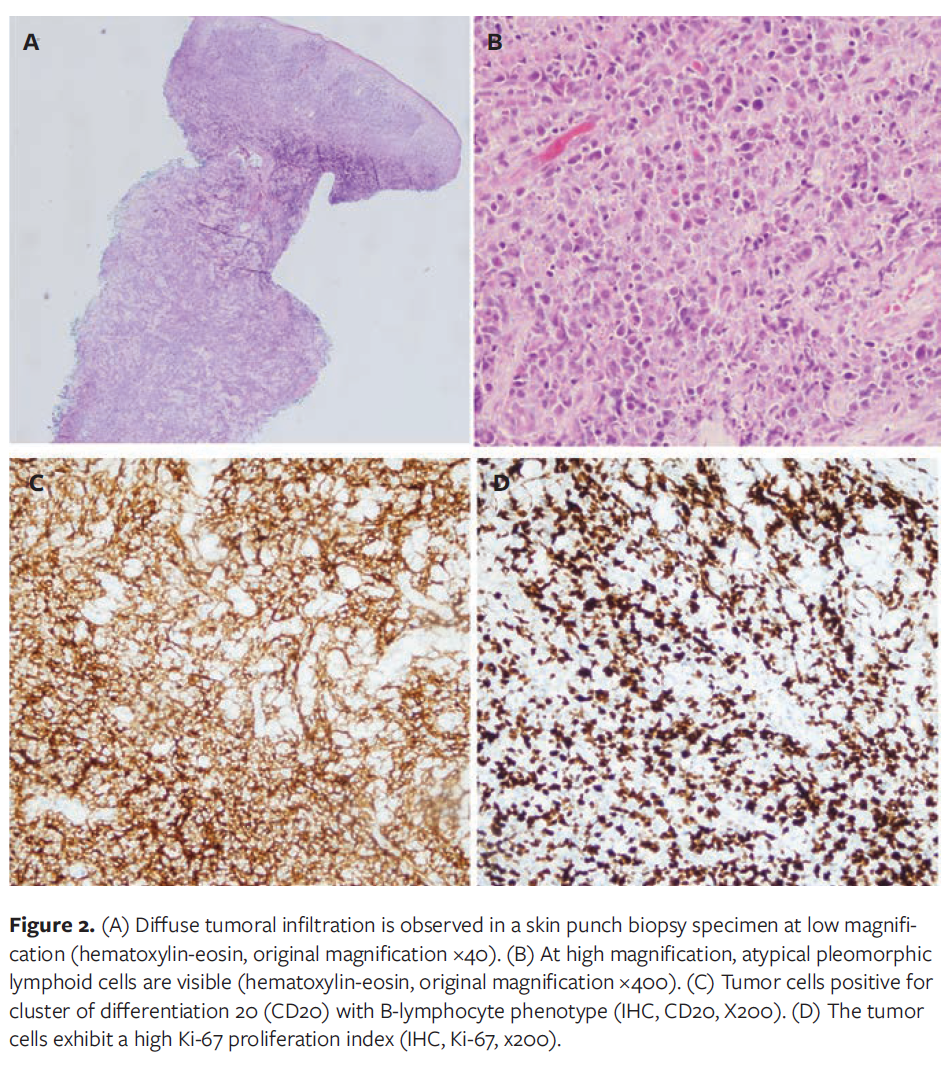
Histopathologic examination of skin punch biopsy material from the affected area revealed neoplastic lymphoid infiltration composed of medium- and large-sized atypical cells arranged in a diffuse pattern with high mitotic figures (Figure 2A, 2B). The infiltration extended from the superficial dermis to the subcutis. Neoplastic lymphoid cells were positive for cluster of differentiation (CD) 20 (Figure 2C), PAX5, BCL6, and CD10, and were negative for BCL2, Cyclin D1, SOX11, CD30, MYC, and Epstein–Barr virus-encoded latent membrane protein 1 on immunohistochemical study. The Ki-67 proliferation index was 80% (Figure 2D). Chromogenic in situ hybridization was negative for Epstein–Barr encoding region. The diagnosis was DLBCL not otherwise specified, germinal center B-cell subtype. Positron emission tomography–computed tomography indicated minimal bone marrow involvement.
The patient’s current ejection fraction was reduced due to a very recent myocardial infarction. The therapeutic regimen included only rituximab to avoid further cardiotoxicity of different combination agents.6 Although the patient’s restricted range of motion improved within the first week of rituximab administration, he experienced substantial necrosis within the lesional area. To facilitate wound healing, negative pressure wound therapy was implemented as an adjuvant approach.7 During the first month of treatment, the patient demonstrated clinical improvement with reduced edema and functional recovery in the left upper extremity (Figure 3). The patient continues to receive rituximab therapy and maintains a stable overall condition.

Discussion
The present case underscores the diagnostic challenge of differentiating between HS and malignancies such as DLBCL, which can mimic the clinical presentation of chronic inflammatory skin conditions. The patient in the present report initially exhibited a typical HS lesion. The negative tissue culture results and the MRI findings depicting multiple lymph nodes were not sufficient to exclude HS, because both may occur during HS disease management. However, the progressive disease course with lack of response to various antibiotic treatments and corticosteroids, as well as hand edema, coupled with the emergence of systemic symptoms, such as weight loss, raised significant concerns for a possible malignancy.
According to the North American clinical management guidelines for HS, diagnosis is primarily clinical.8 However, atypical features such as unilateral involvement, older age at onset, rapidly progressive disease, or failure to respond to standard therapy should prompt consideration of alternative diagnoses and histopathologic evaluation. In the present case, the patient’s older age at presentation, unilateral axillary involvement, rapid progression, systemic weight loss, and poor response to conventional management were not fully consistent with typical HS patterns and supported the decision for early biopsy to exclude malignancy.
Malignant proliferating wounds can present with clinical features such as nodules, abscesses, and draining lesions that may mimic HS.3-5 Previous studies have documented cases of malignancies misdiagnosed as HS, including instances of plasmablastic lymphoma that were obscured by preexisting HS.9 The most critical consideration is that a misdiagnosis of HS may not only delay the correct diagnosis but also result in the initiation of biologic therapies that could potentially worsen an underlying, unrecognized malignancy.6 In cases of suspected HS with an atypical clinical course, unilateral involvement, or failure to respond to standard therapies, timely histopathological examination is valuable for early diagnosis and appropriate treatment.
Population-based studies have shown an increased risk of lymphoma in patients with HS, possibly related to chronic inflammation and immune dysregulation. Tannenbaum et al10 demonstrated increased odds of non-Hodgkin lymphoma, Hodgkin lymphoma, and cutaneous T-cell lymphoma in patients with HS. However, these data primarily describe lymphoma occurring in patients with established HS rather than lymphoma presenting with HS-like clinical features, as seen in the current case. Thus, clinicians should remain alert to lymphoma both as a comorbidity in HS and as a rare HS mimic and should consider biopsy when clinical features are discordant or the course is atypical.10
Histopathologic examination is essential to confirm the diagnosis of DLBCL. In the present case, immunohistochemistry and molecular tests identified characteristic markers of the DLBCL not otherwise specified subtype, emphasizing the significance of biopsy in challenging and atypical cases.11 The management of DLBCL typically involves combination chemotherapy, frequently incorporating rituximab. However, in the present case, rituximab monotherapy was selected due to the patient’s cardiac comorbidities.6,12 Although this approach is less conventional, it was considered appropriate given the patient’s unique circumstances.
Limitations
As with all single-patient case reports, the findings may not be generalizable to broader patient populations. Additionally, the lack of long-term follow-up data limits the ability to evaluate disease progression, sustained remission, or relapse over time.
Conclusion
This case highlights the importance of considering malignancy in patients with unilateral, treatment-resistant lesions that mimic HS. Early biopsy and multidisciplinary evaluation are essential for accurate diagnosis and correct, timely intervention.
Author and Public Information
Authors: Nedim Uysal, MD; Ismail H. Unal, MD; Mukerrem Safalı, MD; Ayca Atas, MD; and Aysenur Botsalı, MD
Affiliations: University of Health Sciences, Gülhane Training and Research Hospital, Ankara, Turkey
Funding: The authors received no financial support for this work.
Disclosures: The authors disclose no financial or other conflicts of interest.
Ethics Statement: Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Corresponding Author: Aysenur Botsalı, MD; University of Health Sciences, Gülhane Training and Research Hospital, Etlik, General Dr. Tevfik Sağlam Cd. No:1, Ankara, Turkey 06010; abotsali@hotmail.com
Manuscript Accepted: March 18, 2026
References
- Sabat R, Alavi A, Wolk K, et al. Hidradenitis suppurativa. Lancet. 2025;405(10476):420-438. doi:10.1016/S0140-6736(24)02475-9
- Sabat R, Jemec GBE, Matusiak Ł, Kimball AB, Prens E, Wolk K. Hidradenitis suppurativa. Nat Rev Dis Primers. 2020;6(1):18. doi:10.1038/s41572-020-0149-1
- Pecora V, Samynathan A, Rosenfeld A, Tariq Z, Saardi K. Cutaneous metastases mimicking hidradenitis suppurativa: a diagnostic challenge. Wounds. 2025;37(2):63-67. doi:10.25270/wnds/24155
- Baig IT, Nguyen QD, Hickson MAS, Ciurea A. Metastatic adenocarcinoma mimicking hidradenitis suppurativa. JAAD Case Rep. 2022;27:91-93. doi:10.1016/j.jdcr.2022.07.026
- Caputo V, Citterio A, Rongioletti F. Uncommon neoplasms mistakenly diagnosed as hidradenitis suppurativa: report of three consecutive cases. Clin Dermatol. 2024;42(6):641-645. doi:10.1016/j.clindermatol.2024.09.019
- Martínez-Banaclocha N, Martínez-Madueño F, Caballé B, et al. A descriptive study of 103 primary cutaneous B-cell lymphomas: clinical and pathological characteristics and treatment from the Spanish Lymphoma Oncology Group (GOTEL). Cancers (Basel). 2024;16(5):1034. doi:10.3390/cancers16051034
- Putri IL, Adzalika LB, Pramanasari R, Wungu CDK. Negative pressure wound therapy versus conventional wound care in cancer surgical wounds: a meta-analysis of observational studies and randomised controlled trials. Int Wound J. 2022;19(6):1578-1593. doi:10.1111/iwj.13756
- Alikhan A, Sayed C, Alavi A, et al. North American clinical management guidelines for hidradenitis suppurativa: a publication from the United States and Canadian Hidradenitis Suppurativa Foundations: Part I. Diagnosis, evaluation, and the use of complementary and procedural management. J Am Acad Dermatol. 2019;81(1):76-90. doi:10.1016/j.jaad.2019.02.067
- Preis S, Kain A, Biedermann T, Volz T. Plasmablastic lymphoma masked by hidradenitis suppurativa. JAAD Case Rep. 2022;27:13-15. doi:10.1016/j.jdcr.2022.06.016
- Tannenbaum R, Strunk A, Garg A. Association between hidradenitis suppurativa and lymphoma. JAMA Dermatol. 2019;155(5):624-625. doi:10.1001/jamadermatol.2018.5230
- Barbati ZR, Charli-Joseph Y. Unveiling primary cutaneous B-cell lymphomas: new insights into diagnosis and treatment strategies. Cancers (Basel). 2025;17(7):1202. doi:10.3390/cancers17071202
- Linschoten M, Kamphuis JAM, van Rhenen A, et al. Cardiovascular adverse events in patients with non-Hodgkin lymphoma treated with first-line cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) or CHOP with rituximab (R-CHOP): a systematic review and meta-analysis. Lancet Haematol. 2020;7(4):e295-e308. doi:10.1016/S2352-3026(20)30031-4









