The Use of Over-the-Counter Aerosolized Triamcinolone Acetonide in the Treatment of Peristomal Pyoderma Gangrenosum: A Case Series
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Peristomal pyoderma gangrenosum (PPG) is a rare neutrophilic dermatosis characterized by painful ulcerations near an abdominal stoma. While topical therapy is a key component of its often multimodal management, many agents risk compromising ostomy seal integrity, thus limiting their effectiveness. Over-the-counter aerosolized steroids may offer a promising alternative, combining anti-inflammatory benefit with minimal disruption to appliance adhesion. Case Series. The cases of 5 patients who developed PPG between 2 weeks and 10 years after surgical creation of an ostomy are presented. Three patients had underlying inflammatory bowel disease, although multiple inflammatory triggers were identified across the cohort. All patients incorporated triamcinolone acetonide 55 mcg/spray into their treatment regimens. Each case demonstrated complete resolution of PPG without disruption of the ostomy appliance adhesion. Conclusion. This case series underscores the potential of over-the-counter aerosolized steroids as both adjunctive and primary therapy in the treatment of PPG. Their ease of access, cost-effectiveness, and compatibility with ostomy systems make them especially appealing for early intervention. Thus, over-the-counter aerosolized steroids represent a practical and promising addition to current PPG management strategies.
Peristomal pyoderma gangrenosum (PPG) is a rare neutrophilic dermatosis characterized by painful, rapidly progressing ulcers with violaceous, undermined borders near an abdominal stoma. While its exact pathophysiology remains unclear, PPG is believed to result from a combination of genetic predisposition and immune dysregulation, leading to an autoinflammatory-like response that may follow trauma.1 Diagnosis is primarily clinical, relying on characteristic history and morphology, though multiple diagnostic frameworks, such as the PARACELSUS score, Su criteria, and Delphi criteria, may assist PPG diagnosis.2
Stoma-related complications are common, with 1 study showing that 73% of patients had reported some form of peristomal skin morbidity interfering with normal ostomy appliance function.3 Given these challenges, dedicated ostomy care services—often led by specialized nurses—play a crucial role in the prevention, early recognition, and management of peristomal complications. PPG management typically necessitates a multimodal approach, including optimizing ostomy and wound care, controlling local inflammation with topical therapies, and addressing underlying systemic disease.1 Because the condition can progress between initial recognition and specialist evaluation, accessible over-the-counter treatments to manage local inflammation could significantly improve patient outcomes.
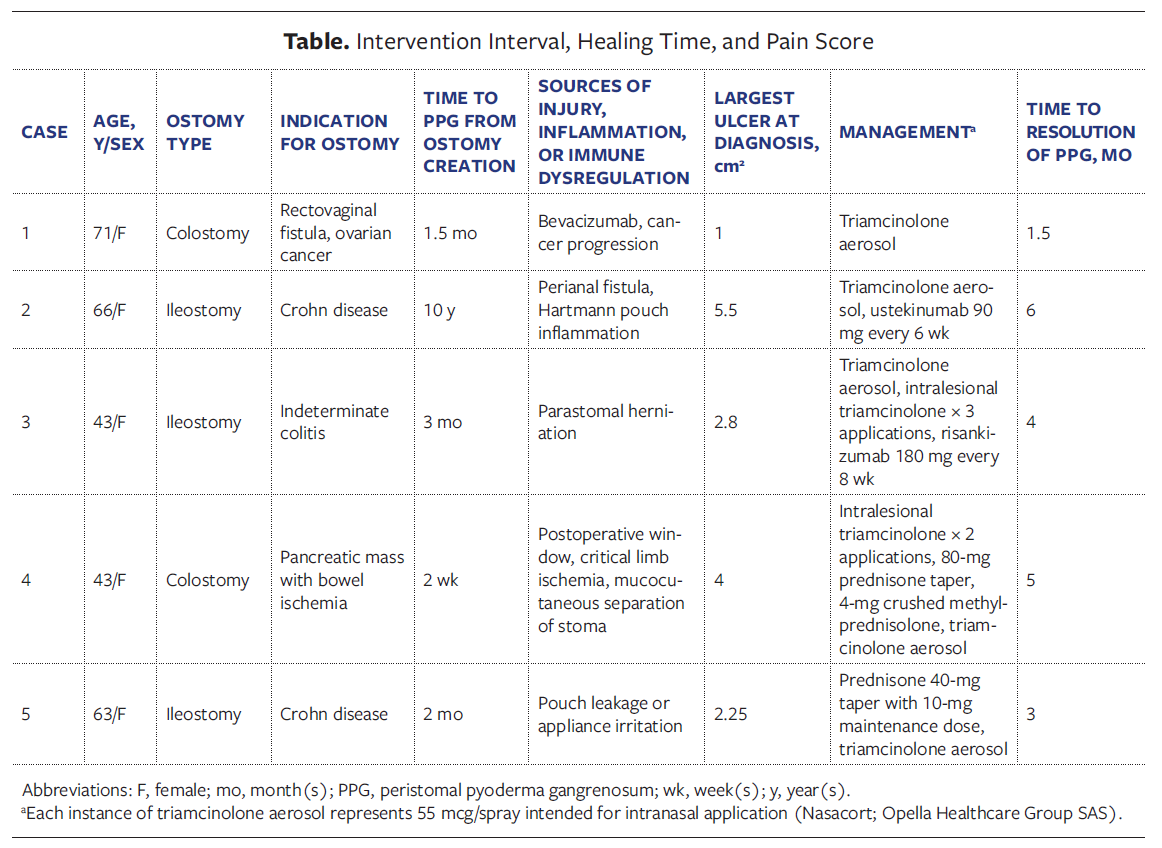
Challenges remain in selecting appropriate local therapies for PPG. The primary goal of topical treatment is to reduce local inflammation while maintaining ostomy seal integrity. However, many topical medication vehicles risk disrupting adhesion and may cause pain due to high alcohol content.3 Thus, there is a need for effective topical regimens that preserve appliance success, minimize pain, and are consistently cost-effective across insurance providers. The senior author (B.H.K.) previously reported on the use of topical powders,4 but the present study is a larger case series using aerosolized triamcinolone acetonide in the management of PPG. These cases explore the potential role of over-the-counter aerosolized steroids, specifically triamcinolone acetonide (55 mcg/spray) intended for intranasal application (Nasacort; Opella Healthcare Group SAS), as part of a treatment strategy for PPG in 5 patients (Table). In all cases, triamcinolone acetonide was recommended at an approximate dose of 1 to 2 sprays per 4 cm2 of affected skin at the time of ostomy appliance changes. Because appliance change schedules varied, application frequency was patient-
specific. This study was approved by The Ohio State University institutional review board (No. 2021H0072).
Cases
Case 1
A 71-year-old female with ovarian cancer treated with bevacizumab and paclitaxel developed 2 peristomal ulcerations near her colostomy 1.5 months after undergoing a transverse colectomy for a rectovaginal fistula. She was diagnosed with PPG, scoring 19 on the PARACELSUS scale (PG highly likely with score ≥10). At the time of diagnosis, the ulcers measured 1 cm² and 0.36 cm². Imaging revealed no evidence of colitis but did show new, progressive metastases in the liver and lungs. Treatment with triamcinolone aerosol, applied every 2 days to 3 days, was initiated, and cancer treatment was discontinued. After 2 weeks, the ulcers had completely granulated, and within 1.5 months, they had fully resolved. The patient continued intermittent triamcinolone aerosol use for an additional 2 months with no relapse peristomal disease.
Case 2
A 66-year-old female with Crohn disease, a pilonidal cyst, and biopsy-proven pyoderma gangrenosum in the gluteal folds with a perianal fistula developed ulcerations around her ileostomy while being treated with ustekinumab 90 mg every 8 weeks. She reported severe pain and difficulty maintaining a seal due to wound drainage and was switched to methylene blue–impregnated dressings. Although she was initially advised to start clobetasol, cost concerns prevented its use. One month later, the ulceration had worsened, measuring 2.5 cm × 2.2 cm × 0.2 cm at the inferior margin of the stoma. Treatment was escalated to ustekinumab 90 mg every 6 weeks and application of triamcinolone aerosol with ostomy appliance changes. Over the course of 3 months the peristomal ulcerations improved, with complete resolution by 6 months on the combined triamcinolone aerosol and ustekinumab regimen. Of note, imaging before and after treatment revealed inflammation of the Hartmann pouch and persistence of the perianal fistula.
Case 3
A 43-year-old female with indeterminate colitis developed an inferior peristomal ulceration 1 week after noticing a parastomal hernia. She was quickly diagnosed with PPG and was started on triamcinolone aerosol and methylene blue–impregnated foam dressings. At the time, the ulcer measured 1.4 cm × 2 cm. She received 0.25 mL of 40 mg/mL triamcinolone injected intralesionally and was advised to continue triamcinolone aerosol and apply lidocaine spray as needed for pain. At 1-month follow-up, the ulcer had worsened, prompting a repeat of intralesional triamcinolone (0.1 mL of 40 mg/mL). One week later, risankizumab 180 mg was begun. After an additional week, improvement was observed, and a final intralesional injection of triamcinolone (2 mL of 15 mg/mL) was administered, with continued risankizumab on a schedule of every 8 weeks and triamcinolone aerosol application. Four months after the ulcer’s initial appearance, the wound had completely reepithelialized.
Case 4
A 43-year-old female with a pancreatic mass developed bowel ischemia requiring colostomy and developed peristomal ulcerations approximately 2 weeks after the procedure. At the time of ulcer appearance, the patient was hospitalized with critical limb ischemia and mucocutaneous separation of the stoma. Two months later she was evaluated by dermatology specialists, who identified 2 cribriform ulcerations surrounding the colostomy site measuring 1 cm × 4 cm and 1 cm × 2.5 cm, respectively. She received an intralesional triamcinolone (1 mL of 10 mg/mL) injection and began applying 4 mg crushed methylprednisolone tablets to the ulcerations every 2 days to 3 days. At 1-month follow-up, the lesions had not improved, prompting an increased dose of intralesional triamcinolone (1 mL of 20 mg/mL). A few weeks later, the patient presented to the emergency department with severe pain secondary to PPG and was discharged on a prednisone taper beginning at 80 mg. Systemic and crushed steroids were promptly discontinued by the patient due to nosebleeds and hyperglycemia. At follow-up in the dermatology department 4 months after PPG appearance, the ulcers had improved, and triamcinolone aerosol was initiated. One month later, the ulcers had resolved, and ostomy takedown was completed shortly after.
Case 5
A 63-year-old female with Crohn disease, psoriasis, and a 1-month history of irritation surrounding the stoma began developing ulcerations around her ileostomy site 2 months postoperative. At that time, the largest ulceration measured less than 2 cm in diameter, and she began prednisone (40 mg to start, tapering to a 10-mg maintenance dose) and methylene blue–impregnated dressings. Two months later, the patient presented to the dermatology department and was diagnosed with PPG, although significant improvement of the peristomal ulcerations was evident. Prednisone was discontinued, and triamcinolone aerosol was initiated, which led to wound resolution within 1 month.
Discussion
Evidence-based guidelines for managing PPG remain limited due to its rarity, clinical variability, and the inconsistent treatment responses in the literature, making standardized recommendations challenging. However, multiple reports have demonstrated favorable outcomes with a combination of steroids, immunomodulators, and biologics in variable formulations, along with stoma appliance optimization.5 The present case series demonstrates resolution of PPG in 5 patients, all of whom used aerosolized triamcinolone 55 mcg/spray as a component of their successful regimen.
Notably, none of the patients in the present study reported ostomy seal disruption due to the application of triamcinolone aerosol, which distinguishes it from other topical vehicles.3,6 This is important because the irritating effect of stoma leakage may provoke a pathergy-
like response, potentially counteracting the benefits of local anti-inflammatory treatment. Thus, triamcinolone aerosol offers multiple advantages, including rapid drying to maintain pouch adhesion and over-the-counter accessibility.
PPG is estimated to occur in 2% to 4% of patients with inflammatory bowel disease (IBD), and up to 69% of patients with PPG have a concurrent systemic disease flare.5 In the present series, 3 of 5 patients had underlying IBD, but many potential sources of inflammation were identified near ulcer appearance, including malignancy, Hartmann pouch inflammation, parastomal herniation, mucocutaneous separation, persistent exposure of effluent, perineal fistula, and ischemia. This variability highlights the individualized approach necessary in identifying sources of persistent trauma or immune dysfunction, which is crucial because outcomes differ by comorbidity.7
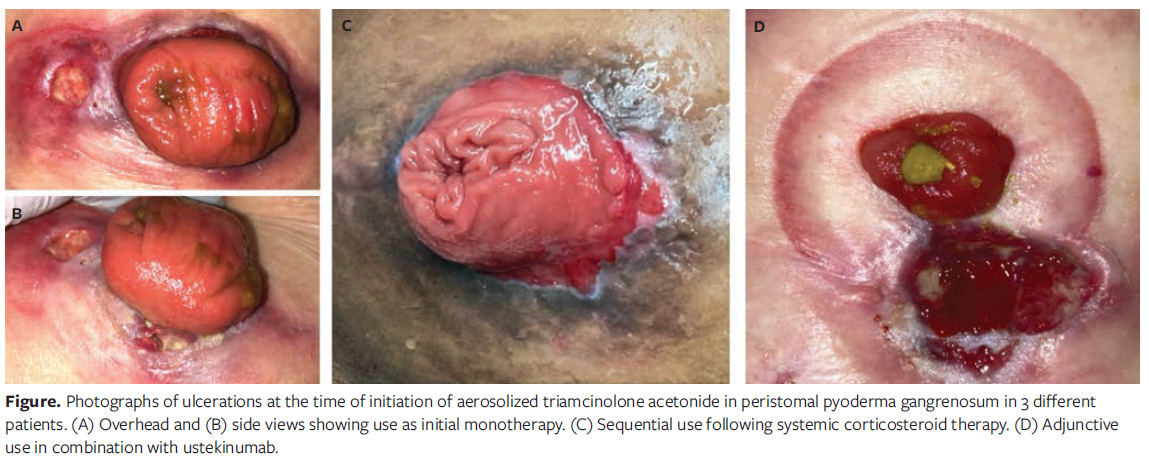
The present case series highlights the varied clinical applications of aerosolized triamcinolone acetonide 55 mcg/spray, including its use as initial monotherapy, as adjunctive therapy, and as sequential therapy following partial improvement, culminating in disease resolution (Figure). These findings add to previous reports of aerosolized steroids being used successfully for peristomal inflammation.8,9 Given that ostomy care teams are often the first to recognize signs of PPG, over-the-counter steroid treatment may represent a practical and accessible intervention that can be initiated early in the development of PPG. Further, the over-the-counter nature of the spray may buffer the price fluctuations and insurance formulary issues associated with prescription corticosteroid sprays and aerosols.
Limitations
This case series is limited by a small sample size of 5 patients, which constrains the ability to draw broad conclusions and increases susceptibility to selection bias. Additionally, all patients received multiple concurrent therapies, including systemic corticosteroids, biologics, or intralesional injections, which complicated efforts to isolate the specific therapeutic effect of aerosolized triamcinolone. The heterogeneity in underlying conditions and treatment regimens further limits generalizability. Controlled studies with larger cohorts are needed to evaluate the independent efficacy of aerosolized steroids in PPG management.
Conclusion
PPG is a rare but severe complication of ostomies that requires prompt recognition and a multimodal treatment approach. This case series highlights the potential role of aerosolized triamcinolone acetonide 55 mcg/spray as an accessible therapeutic option that can be readily integrated into routine ostomy appliance changes. Notably, use of this spray did not compromise ostomy seal integrity, thus addressing a key challenge associated with other topical treatments. In the absence of standardized guidelines, over-the-counter steroid therapy may offer a practical early intervention, potentially improving patient outcomes.
Author and Public Information
Authors: Jordan Z. Hill, MD1; Varshita Chirumamilla, BS1; and Benjamin H. Kaffenberger, MD MS2
Affiliations: 1The Ohio State University College of Medicine, Columbus, OH, USA; 2Department of Dermatology, The Ohio State University Wexner Medical Center, Columbus, OH, USA
Corresponding Author: Benjamin H. Kaffenberger, MD, MS; Department of Dermatology, The Ohio State University Wexner Medical Center, 1328 Dublin Road, Suite 100, Columbus, OH 43212; Benjamin.Kaffenberger@osumc.edu
Funding: None.
Conflicts of Interest: B.H.K. reports consulting fees from Almirall, Boehringer-Ingelheim, Lilly, InflaRx, Novartis, Novocure; research fees for Boehringer-Ingelheim, Leo, Merck, HCW Biologics, InflaRx, Janssen; and speaking fees from Sanofi. The other authors disclose no financial or other conflicts of interest.
Ethical Statement: Only deidentified images were used and thus patient consent was unnecessary.This study was approved by The Ohio State University institutional review board (No. 2021H0072).
Manuscript Accepted: March 18, 2026
References
- Alavi A, French LE, Davis MD, Brassard A, Kirsner RS. Pyoderma gangrenosum: an update on pathophysiology, diagnosis and treatment. Am J Clin Dermatol. 2017;18(3):355-372. doi:10.1007/s40257-017-0251-7
- Nusbaum KB, Boettler M, Korman AM, et al. Subjective assessments in pyoderma gangrenosum diagnostic frameworks undermine framework agreement. Int J Dermatol. 2024;63(2):e67-e69. doi:10.1111/ijd.16952
- Lyon CC, Smith AJ, Griffiths CE, Beck MH. The spectrum of skin disorders in abdominal stoma patients. Br J Dermatol. 2000;143(6):1248-1260. doi:10.1046/j.1365-2133.2000.03896.x
- Boettler M, Kaffenberger B. Budesonide capsules for peristomal pyoderma gangrenosum. J Am Acad Dermatol. 2022;86(2):e37-e38. doi:10.1016/j.jaad.2021.05.053
- Afifi L, Sanchez IM, Wallace MM, Braswell SF, Ortega-Loayza AG, Shinkai K. Diagnosis and management of peristomal pyoderma gangrenosum: a systematic review. J Am Acad Dermatol. 2018;78(6):1195-1204.e1. doi:10.1016/j.jaad.2017.12.049
- Nicholson J, Sriskandarajah S, Moore J, Clouston H, Telford K. Aerosol steroids for the treatment of peristomal mucocutaneous breakdown due to severe eczema. Int J Surg Case Rep. 2014;5(12):1173-1175. doi:10.1016/j.ijscr.2014.11.015
- Ravi M, Trinidad J, Spaccarelli N, Kaffenberger B. The impact of comorbidity identification on outcomes in patients with pyoderma gangrenosum: a retrospective cohort study of previously hospitalized patients. J Am Acad Dermatol. 2022;87(1):194-197. doi:10.1016/j.jaad.2021.07.032
- Mitsaki KS, Gaglani B, Sethi M. Rapid and sustained resolution of peristomal pyoderma gangrenosum with aerosol steroid treatment. J Wound Ostomy Continence Nurs. 2025;52(1):81-83. doi:10.1097/WON.0000000000001150
- Boland J, Brooks D. Topical application of a beclometasone steroid inhaler for treatment of stoma inflammation. Palliat Med. 2012;26(8):1055-1056. doi:10.1177/0269216312446363