



Use of Synthetic Electrospun Fiber Matrix in the Sealing of Tunneling, Undermining, and Cavity Wounds
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Tunneling, undermining, and cavity wounds created by pressure, infection, or surgery present unique treatment challenges. These wound complications are prone to infection and may necessitate reconstructive flap procedures. Often patients are sarcopenic and malnourished, leading to complications or poor outcomes. The synthetic electrospun fiber matrix (SEFM) studied in this series is a fully synthetic, resorbable extracellular matrix that has shown promise in stimulating healing responses in challenging wound environments. Objective. To evaluate whether the SEFM, in conjunction with proper wound care, supports rapid closure of wound tunneling or undermining, thus obviating the need for complex reconstruction. Methods. A retrospective review of 9 patients with 11 multifactorial wounds treated with the SEFM was conducted. Patients who underwent a single application or serial applications of the SEFM to cavity, tunneling, or undermining wounds were included. All wounds underwent initial surgical sterilization with sharp excision prior to application. Healing progress, resolution of tunneling or undermining, and incidence of complications were assessed and documented at follow-up visits. Results. These wound complications were successfully managed without extensive surgical reconstruction or amputation. Wounds ranged from acute to chronic (>2 years’ duration) and were traumatic, iatrogenic, or secondary to pressure injuries or hidradenitis. Complete wound healing or granulation was achieved in all cases and, as possible to perform after healing, neither magnetic resonance imaging nor white blood cell sequestration showed further evidence of osteomyelitis. Durable results with no wound breakdown or signs of infection were noted at 6- to 18-month follow-up. Conclusion. The SEFM successfully supported healing and collapse of wound tunneling and undermining in a complex patient population. The rapid resolution of these wound complications mitigated the need for large flap reconstructions and recommended amputations. More studies are needed to determine patient populations who would be best served by this technique.
Tunneling, undermining, and cavity wounds created by pressure, friction, infection, trauma, or surgery are uniquely challenging to the health care provider. Although each of these conditions has its own unique presentation, tunneling, undermining, and cavity wounds are similar in that they are characterized by an inability to observe them at an initial glance; additionally, these tracks, pockets, or sinuses can extend deep underneath or around the visible wound.1 Undermining occurs outward from the original wound location, creating a pocket of dead space directly underneath the epidermis surrounding the observable wound.2 In contrast, tunneling occurs deeper within the observable wound, creating tracks deep into subcutaneous tissues.2 Cavity wounds are more poorly defined in the literature; these can range from shallow to deep, but they are most commonly documented as wounds that extend beneath the dermal layer.1 Within these cavity wounds, tunneling and undermining can occur concomitantly.1 Common causes of all of these wound presentations include friction at the site of an existing open wound, infection, traumatic injury, or surgical dehiscence.1,2 Early identification and treatment of these wounds is critical to ensuring positive healing outcomes, because a wound will not entirely heal without addressing these underlying areas. Delays in treatment can lead to nonhealing, infection, and disability.1
Treatment of these wound complications can be challenging. Many patients who present with undermining, tunneling, or cavity wounds have underlying infection within the tracks or sinuses in addition to chronic inflammation, leading to delays in healing.1,3 These patients often present with comorbid conditions that negatively affect healing, including diabetes, obesity, and malnutrition, among others.3 The first step in facilitating healing of these wounds involves addressing underlying disease and controlling comorbidities that may stall healing responses. Active infection should be promptly managed with either local or systemic treatment.1 The wound should be thoroughly cleansed and debrided as appropriate to remove nonviable tissue and subsequently off-loaded as appropriate to prevent further damage from pressure or friction.1,4,5 It is also critical to eliminate dead space within these wounds in order to reduce the risk of infection.1,6 This can be accomplished in a variety of ways depending on the type of wound. Packing the dead space within tunneling, cavity, or undermining wounds is often performed to both fill dead space and provide a moist wound environment to stimulate healing and reduce bacterial infiltration.1,6
When standard treatment methods for cavity, undermining, or tunneling wounds are unsuccessful, it may be necessary to consider more invasive reconstructive methods.7,8 Reconstruction often necessitates extensive operations for tunnel marsupialization and/or rotational or free flaps.7,8 Often patients are sarcopenic and malnourished, leading to complications or poor outcomes, including amputation.9 A synthetic electrospun fiber matrix (SEFM) (Restrata; Acera Surgical, Inc) could be considered in the management of undermining, tunneling, and cavity wounds. The SEFM is engineered to mimic native extracellular matrix and thus encourage tissue ingrowth in the form of fibroblast migration, proliferation, and subsequent neovascularization.10,11
The SEFM is composed of bioresorbable fibers that are engineered to resorb at a rate matching tissue ingrowth, thus eliminating the need for secondary removal that can retraumatize new tissue.10-12 Because the device is fully synthetic, it is resistant to enzymatic degradation.10,11 This is a highly beneficial feature when treating these wounds, which are often contaminated and require the use of harsh cleaning chemicals, both of which can prematurely degrade biological materials.10,11 Areas of undermining and tunneling often have challenging topography that makes effective packing difficult.1 The SEFM is highly conformable and can be utilized either in full sheets or in a particulate form factor, allowing for maximized contact with the surrounding tissue to stimulate wound healing.10,11
In the present retrospective case series, the SEFM was applied to cavity wounds and areas of undermining and tunneling to stimulate healing and collapse of dead space to avoid the need for reconstructive procedures. It was hypothesized that surgical sterilization of the wound followed by the SEFM application may rapidly seal off these challenging wounds, obviating the need for complex reconstruction.
Methods
A retrospective case series was conducted to identify and analyze healing outcomes in patients with undermining, tunneling, or cavity wounds treated with the SEFM in the operating room by a single general surgeon (T.P.). Following institutional review board (IRB) approval (IRB #2007802), the authors of the present series reviewed the medical charts of patients treated between June 2021 and October 2023 to identify eligible patients. Inclusion criteria were as follows: patients aged 18 years or older at the time of the SEFM application; 1 or more applications of the SEFM to an undermining, tunneling, or cavity wound in the operating room following sharp debridement; and at least 1 follow-up visit to assess healing progress.
Demographic information, including sex and comorbid conditions, were collected, as were wound-specific data such as wound etiology and location. In addition to data on the SEFM placement, the type of wound dressing used was also documented. During follow-up visits, the degree of tunneling and undermining was assessed and documented. Time to resolution was calculated based on time from surgery to documentation of resolution in the patient chart. Complications during the healing period were collected from patient charts. Complications were categorized as either minor or major, with major complications being those that necessitated surgical or invasive interventions.
Results
Following chart review, 9 patients with 11 wounds were determined to be eligible for inclusion and analysis. Included wounds ranged from acute to chronic (>2 years’ duration), and the wounds were traumatic, iatrogenic, or secondary to pressure ulcers or hidradenitis suppurativa. Three patients (33%) had documented evidence of osteomyelitis on bone scintigraphy or computed tomography. These 3 patients underwent 6 weeks of treatment with intravenous antibiotics in addition to complete wound sterilization with bony debridement. Negative post-debridement biopsies were confirmed prior to the first application of the SEFM.
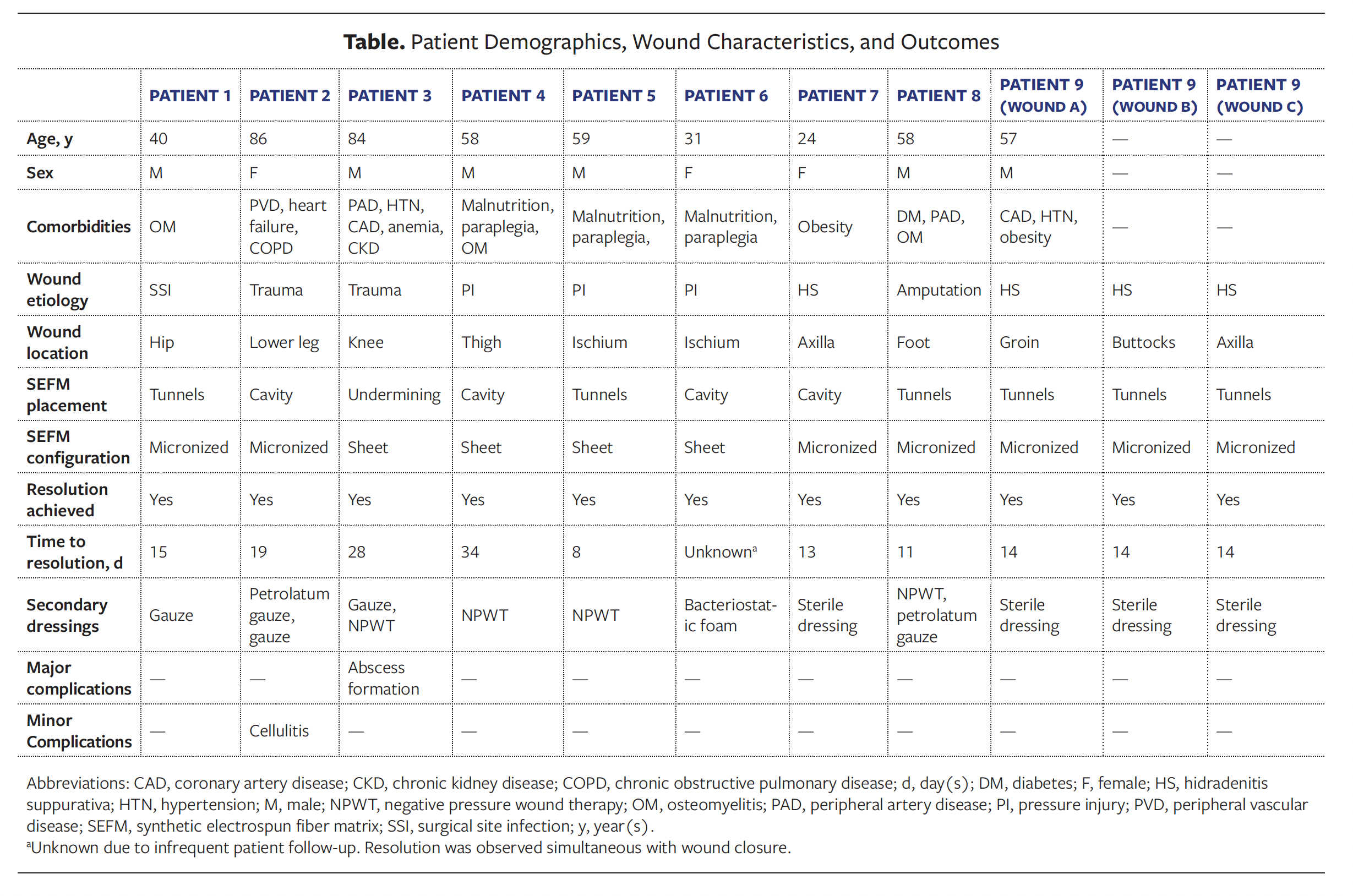
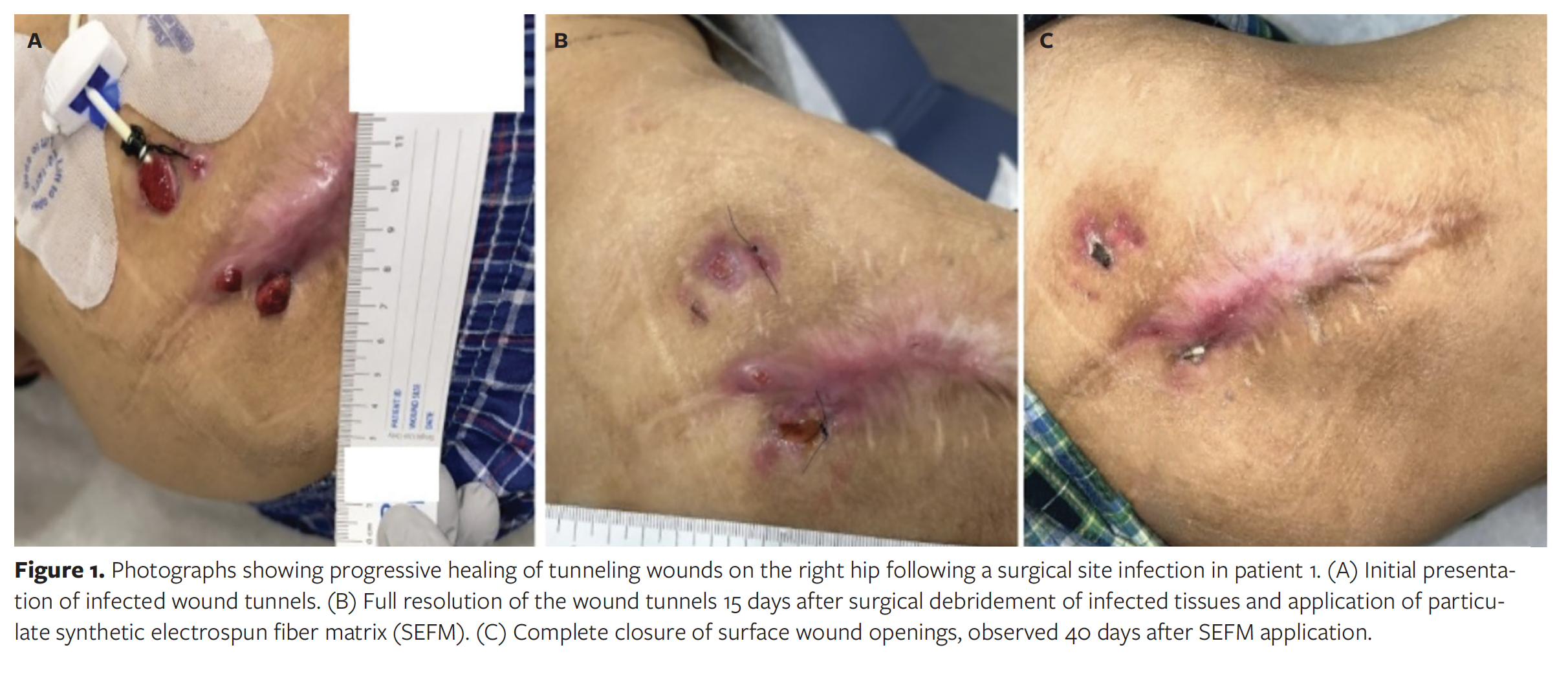
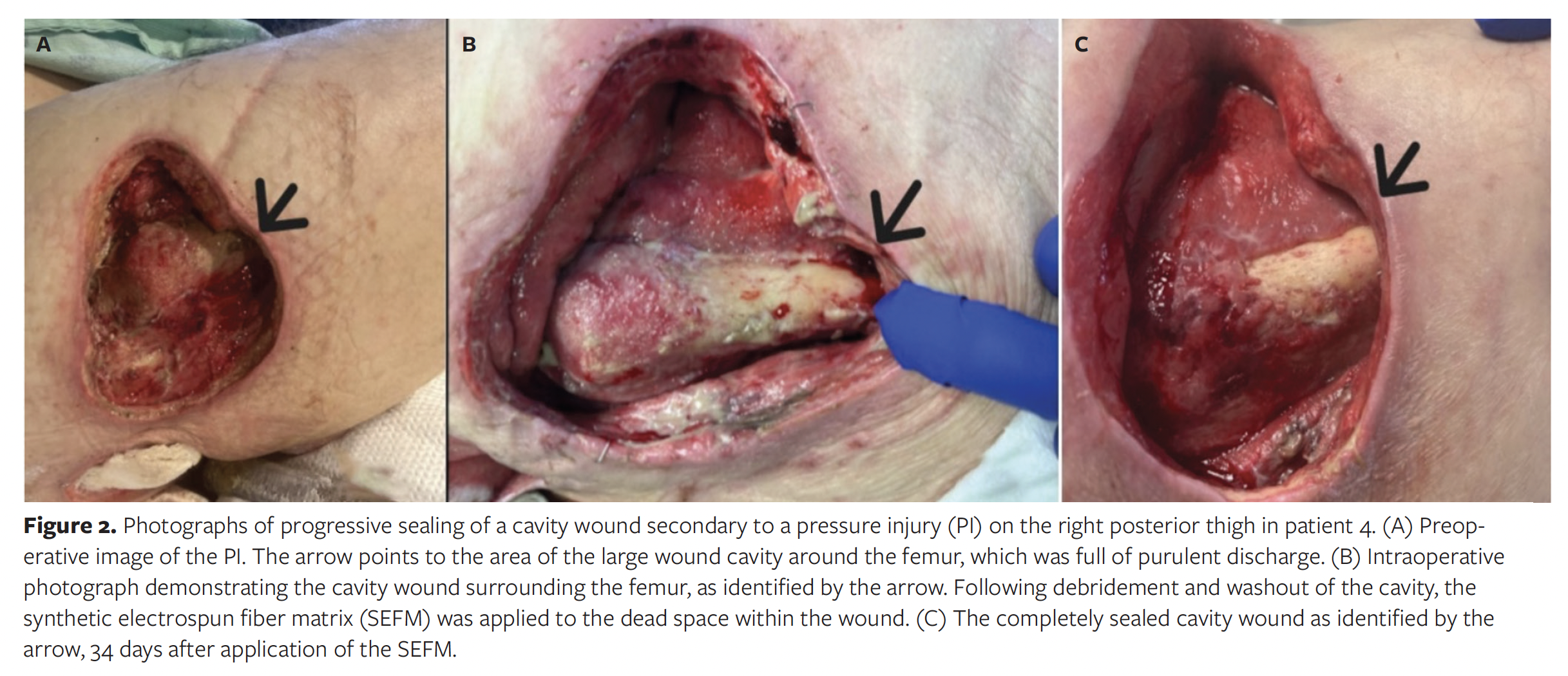
The average (SD) patient age was 55 (20) years. The patients had a multitude of comorbidities, including osteomyelitis, paraplegia, malnutrition, peripheral arterial disease, obesity, and diabetes. Wound locations varied across the population, occurring on the ischium, thigh, axilla, hip, knee, foot, groin, and buttocks. A detailed description of patient demographics, wound characteristics, and healing outcomes is provided in the Table. Representative wound images are presented in Figures 1 and 2.
Following surgical source control, 2 form factors of the SEFM were used to manage these wounds. Both the particulate and the sheet version of the SEFM can be used in undermining, tunneling, or cavity wounds; however, the particulate version may be more easily used in such wounds because it can be packed into deep tunnels. A variety of dressings were used in conjunction with the SEFM, including gauze, negative pressure wound therapy (NPWT) dressing, petrolatum gauze, and other absorbent materials. In addition to receiving appropriate wound dressings, patients underwent regular wound monitoring by qualified health care staff and received supportive care as appropriate, such as off-loading and glucose control. All wounds included in the study achieved complete resolution of tunneling and undermining, as well as collapse of any cavities. Mean (SD) time to complete resolution was 17 (8.8) days, with the exception of 1 outlier in which the exact date of cavity collapse was unknown due to inconsistent follow-up, and collapse was documented simultaneously at the time of wound closure.
In all cases, tunneling, undermining, and cavities resolved. When possible to perform, posthealing magnetic resonance imaging or white blood cell sequestration showed no further evidence of osteomyelitis. Durable results were achieved at 6- to 18-month follow-up, with no further wounds or signs of infection. Three complications occurred. One major complication—abscess formation requiring incision and drainage (I&D)—occurred in 1 patient. The abscess was superficial and occurred later in the wound healing process; sealing of extensive undermining prevented deep abscess formation and systemic symptoms. A course of prophylactic antibiotics was initiated after I&D, and this patient achieved full wound closure without further complications. One patient experienced the minor complication of superficial cellulitis, which was identified by another provider. The cellulitis was successfully managed with a short course of oral antibiotics. A second patient developed partial skin graft loss after resolution of wound tunnels. This complication was attributed to decreased blood perfusion related to the patient’s history of diabetes and peripheral artery disease and deemed to be unrelated to treatment of the tunneled wound regions.
Discussion
In the present retrospective case series, the SEFM was used to resolve undermining, tunneling, and cavity wounds in patients with multiple comorbidities and complex wound etiologies. In many of these cases, progression of undermining or sinus tracks could have resulted in hip disarticulation or amputation without quick resolution. In the present case series, none of the SEFM-treated patients required amputation despite significant risk of this due to the depth of wound tunnels or cavities and chronically exposed bone. The costs associated with these complications and poor overall health outcomes to both health care systems and patients alike can be quite high.13,14 By mitigating the need for amputation in this population, the costs associated with these complications as well as decline in quality of life may be avoided.
While the present report is the first to evaluate the SEFM in a series of patients with tunneling, undermining, and cavity wounds, the SEFM demonstrated positive outcomes in a prior publication reporting a single pressure ulcer.15 That ulcer presented as a massive cavity wound with undermining and 2 exposed vertebral segments; over a 16-year period, it had not healed after 3 weeks of NPWT, 11 years of wet-to-dry dressings, and 3 flap procedures. On presentation, the wound was swabbed and was found to be positive for Staphylococcus aureus (S aureus), Pseudomonas, Escherichia coli (E coli), and Proteus mirabilis. Treatment with intravenous antibiotics was initiated in parallel with applications of the SEFM, with a total of 9 applications in an 11-week period, resulting in granulation tissue formation over exposed vertebrae, resolution of undermining, and exudate reduction.15 In the context of tunneling, undermining, or cavity wounds, exudate reduction is critical due to the limited amount of surface area that allows for drainage.
Wounds that have progressed to cavity wounds or that have developed areas of tunneling or undermining are usually chronic in nature, and these features have arisen as complications of nonhealing.1,5 Chronic wounds such as these are often contaminated due to prolonged environmental exposure.16 Frequently, skin substitutes are used to pack these wounds and encourage healing, but many have biologic components.1,17,18 Given the contaminated microenvironment, biologic materials may not be ideal due to the risk of premature degradation on exposure to bacteria present within the wound.10,11 The SEFM is indicated for use within contaminated wounds because its synthetic composition provides resistance to bacterial breakdown and premature enzymatic degradation.10,11 In a prior in vitro study of the SEFM per United States Pharmacopeia (USP) <51> Antimicrobial Effectiveness Testing standards, the matrix demonstrated passing results against some of the most documented microbes found in the wound bed, including E coli, Pseudomonas aeruginosa, S aureus, Proteus mirabilis, Enterococcus faecalis, Aspergillus brasiliensis, and Candida albicans.19
Deep cavity wounds and tunneling wounds can frequently progress deep beyond the dermal layer and may lead to exposed bone or joint cavity.1,4,20 Chronically exposed bone is susceptible to infections such as osteomyelitis. Osteomyelitis can be difficult to treat and may result in amputation or slow wound healing, which can reintroduce risk of recurrence if successful coverage of exposed bone is not achieved quickly.21,22 In the present case series, 3 patients presented with evidence of osteomyelitis prior to initiation of treatment with the SEFM. Following appropriate antibiotic therapy and bony debridement, application of the SEFM was performed and wound healing was observed. This indicated the resolution of any remaining active underlying infection, with 1 incident being documented on posttreatment bone scanning. Wounds with chronically exposed bone have shown response to the SEFM in prior studies.23 In a single case report evaluating use of the SEFM on a chronic calcaneal wound with exposed bone, repeat applications of the SEFM resulted in granulation tissue formation over the bone, despite prior evidence of osteomyelitis and several prior failed treatments.23 This was also confirmed by histopathologic assessment of the re-granulated tissue at the bone/tissue interface, which demonstrated no evidence of residual osteomyelitis, foreign materials, or bacteria, and only mild acute inflammation.23
NPWT is commonly used in cavity and tunneling wounds and can be used with a variety of packing materials.1,6 Foam is the most commonly used material to evenly disperse vacuum pressure and improve fluid drainage.1,6 NPWT is highly effective in stimulating healing responses, but complications associated with foam have been reported.6 The foam is not resorbable, and complications associated with foam retention within the wound occurred most often within deep cavity wounds.6 Additionally, newly formed tissue may grow into the foam itself, resulting in pain on removal and loss of new, healthy tissue.6 These complications often arise due to poor compliance with the required dressing changes, which should occur every 2 days to 3 days.6
The SEFM used in the present case series mitigated the risk of pain, tissue trauma, and foam retention due to its ability to fully resorb through hydrolysis. This rate matches that of tissue ingrowth (approximately 1 week-3 weeks depending on wound moisture) and ensures the gradual off-loading of new tissue from the matrix to the wound bed.10,11 This prolonged resorption time frame limits the need for frequent, deep wound dressing changes. NPWT has been used in conjunction with the SEFM, with positive results to date, and can also be used with instillation to treat the wound with antimicrobial and cleaning solutions.24 While this approach may degrade biologic materials, it can work in conjunction with the SEFM due to its synthetic resistance to premature degradation upon exposure.10,
Limitations
As a retrospective case series, the present study has limitations. There is a limited number of patients and wound sites, in addition to a combination of tunneling, cavity, and undermining wounds across a variety of wound etiologies. These factors make the generalizability of results challenging. This study lacks direct comparison to standard of care or other advanced wound therapies. Additionally, a variety of secondary dressings and configurations of the SEFM were used in this patient cohort. This creates challenges in elucidating the exact effects of the SEFM in this population and in determining which configuration may be ideal for use. Future prospective studies should focus on a single wound etiology as a precursor to larger, comparative trials.
Conclusion
In the present retrospective case series, the SEFM was successfully used to collapse and re-granulate undermining, tunneling, and cavity wounds. The resorbable and synthetic features of the matrix likely contributed to this success, because synthetic materials remain resistant to enzymatic degradation in these often highly exudative wounds, while the resorbable nature of the device limits the need for secondary removal, which can potentially traumatize newly formed tissue. The success observed in the present study indicates the need for further studies evaluating use of the SEFM in specific wound etiologies.
Author and Public Information
Authors: Thea Price, MD1; and Katie Meador, NP2
Affiliations: 1Rush Medical College, Department of Surgery, Rush University, Chicago, IL, USA; 2Rush University Medical Center, Department of General Surgery, Chicago, IL, USA
Disclosure: The authors received payment from Acera Surgical, Inc, in the form of a consulting agreement for time spent on data collection and review.
Ethical Approval: This study was approved by the Institutional Review Board (IRB #2007802).
Correspondence: Thea Price, MD; 4500 San Pablo Rd S, Jacksonville, FL 32224; Price.Thea@mayo.edu
Manuscript Accepted: January 30, 2026
References
wounds in clinical practice. Wound Care Today. Accessed in August 2024. https://www.woundcare-today.com/journals/issue/wound-care-today/article/addressing-challenges-cavity-wounds-clinical-practice
2. Kirwan H, Pignataro R. The skin and wound healing. In: Magee DJ, Zachazewski JE, Quillen WS, Manske RC, eds. Pathology and Intervention in Musculoskeletal Rehabilitation. 2nd ed. Elsevier; 2016:28.
3. Rosenzweig A, Lee M. Wound care. In: Fenstemacher P, Winn P, eds. Long-Term Care Medicine: A Pocket Guide. Humana Press; 2011:205-222. Skolnik NS, ed. Current Clinical Practice.
4. Vowden K. Defining, assessing and managing cavity wounds. Wounds UK. 2016;12(1):18-23.
5. Nagle SM, Stevens KA, Wilbraham. Wound Assessment. In: StatPearls. StatPearls Publishing; 2023. Last updated June 26, 2023.
6. Huang C, Leavitt T, Bayer LR, Orgill DP. Effect of negative pressure wound therapy on wound healing. Curr Probl Surg. 2014;51(7):301-331. doi:10.1067/j.cpsurg.2014.04.001
7. Norman G, Wong JKF, Amin K, Dumville JC, Pramod S. Reconstructive surgery for treating pressure ulcers. Cochrane Database Syst Rev. 2022;10(10):CD012032. doi:10.1002/14651858.CD12032.pub3
8. Chang JW, Oh SW, Oh J, Choi MSS. Treatment of deep cavities using a perforator-based island flap with partial de-epithelization. BMC Surg. 2018;18(1):96. doi:10.1186/s12893-018-0431-2
9. Skórka M, Więch P, Przybek-Mita J, Malisiewicz A, Pytlak K, Bazaliński D. Nutritional status of people with a coexisting chronic wound and extended assessment using bioelectrical impedance. Nutrients. 2023;15(13):2869. doi:10.3390/nu15132869
10. MacEwan MR, MacEwan S, Kovacs T, Batts J. What makes the optimal wound healing material? A review of current science and introduction of a synthetic nanofabricated wound care scaffold. Cureus. 2017;9(10):e1736. doi:10.7759/cureus.1736
11. MacEwan M, Jeng L, Kovács T, Sallade E. Clinical application of bioresorbable, synthetic, electrospun matrix in wound healing. Bioengineering (Basel). 2022;10(1):9. doi:10.3390/bioengineering10010009
12. Dinah F, Adhikari A. Gauze packing of open surgical wounds: empirical or evidence-based practice? Ann R Coll Surg Engl. 2006;88(1):33-36. doi:10.1308/003588406X83014
13. Qaarie MY. Life expectancy and mortality after lower extremity amputation: overview and analysis of literature. Cureus. 2023;15(5):e38944. doi:10.7759/cureus.38944
14. Wong LH, Woelber E, Wyland A, et al. Is reoperation higher than expected after below-the-knee amputation? A single-center evaluation of factors associated with reoperation at 1 year. Clin Orthop Relat Res. 2021;479(2):324-331.
15. Herron K. Treatment of a complex pressure ulcer using a synthetic hybrid-scale fiber matrix. Cureus. 2021;13(4):e14515. doi:10.7759/cureus.14515
16. Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv Wound Care (New Rochelle). 2015;4(9):560-582. doi:10.1089/wound.2015.0635
17. Brigido SA, Schwartz E, McCarroll R, Hardin-Young J. Use of an acellular flowable dermal replacement scaffold on lower extremity sinus tract wounds: a retrospective series. Foot Ankle Spec. 2009;2(2):67-72. doi:10.1177/1938640009333474
18. Sood A, Granick MS, Tomaselli NL. Wound dressings and comparative effectiveness data. Adv Wound Care (New Rochelle). 2014;3(8):511-529. doi:10.1089/wound.2012.0401
19. Sallade E, Grimes D, Jeng L, MacEwan MR. Antimicrobial effectiveness testing of resorbable electrospun fiber matrix per United States Pharmacopeia (USP) <51>. Cureus. 2023;15(12):e50055. doi:10.7759/cureus.50055
20. Butcher M. Managing wound sinuses. Nurs Times. 2002;98(2):63.
21. Lew DP, Waldvogel FA. Osteomyelitis. N Engl J Med. 1997;336(14):999-1007. doi:10.1056/NEJM199704033361406
22. Schmidt BM, Keeney-Bonthrone TP, Hawes AM, et al. Comorbid status in patients with osteomyelitis is associated with long-term incidence of extremity amputation. BMJ Open Diabetes Res Care. 2023;11(6):e003611. doi:10.1136/bmjdrc-2023-003611
23. Harder JG, Hernandez EJ, MacEwan MM. Histopathologic analysis of a recalcitrant calcaneal wound treated using a synthetic hybrid-scale fiber matrix. Plast Reconstr Surg Glob Open. 2024;12(2):e5597. doi:10.1097/GOX.0000000000005597
24. Fernandez L, Schar A, Matthews M, et al. Synthetic hybrid-scale fiber matrix in the trauma and acute care surgical practice. Wounds. 2021;33(9):237-244.
25. Temple EW. Treatment of hematomas using a synthetic hybrid-scale fiber matrix. Cureus. 2022;14(7):e26491. doi:10.7759/cureus.26491
26. Chowdhry S. Utility of a synthetic hybrid-scale fiber matrix in surgical soft tissue reconstruction. Eplasty. 2024;24:e2.
27. Fernandez LG, Matthews MR, Kim PJ. A synthetic hybrid-scale fiber matrix for complex surgical wounds: consensus guidelines. Wounds. 2023;35(5):E160-E168. doi:10.25270/wnds/22067






