The Importance of Accurate Color in Wound Photography and Data
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Wound photography is widely used for clinical assessment, documentation, telemedicine, and emerging analytic applications. Despite this reliance on wound photography, it has developed largely outside the objective acquisition and accuracy standards applied to other medical imaging modalities. Thus, tissue color, a primary determinant of wound evaluation, may be inconsistently represented in routine clinical photographs. Methods. A structured literature review was conducted, synthesizing peer-reviewed studies, standards documents, and large observational analyses addressing wound photography accuracy, color calibration, acquisition standardization, analytic performance, clinical interpretation variability, and documentation use. Searches were performed across major biomedical databases, with findings synthesized narratively. Conference-reported datasets were included as corroborative evidence when peer-reviewed data were limited. Results. Across studies, uncalibrated wound photographs demonstrated substantial deviation from known color reference values, with wide dispersion of clinically relevant tissue colors. In contrast, standardized acquisition techniques and use of color reference targets were consistently associated with reductions in measured color error and with improved reproducibility. Analytic studies demonstrated that predictive performance varied with baseline image fidelity, while clinical studies reported divergent assessments and measurement variability when photographs were obtained without standardized methods. Conclusion. The literature demonstrates that color inaccuracy in wound photography is prevalent, measurable, and consequential when photographs are used for interpretation, documentation, or analysis. Standardized acquisition and objective assessment of color accuracy improve photographic fidelity and support more reliable clinical and analytic use. Adoption of objective image-quality standards aligned with other medical imaging fields represents a practical pathway to improving reliability in wound photography.
Color is a primary descriptor of wound assessment, guiding identification of tissue type; evaluation of healing, inflammation, or necrosis; and affecting clinical decision-making.1–4 In addition to color, key wound descriptors such as area, 3-dimensional configuration, epithelial surface progression, and measurement reproducibility have been shown to vary with photographic technique and image quality.5–7 Clinicians routinely rely on visual color cues to distinguish granulation tissue, slough, inflammation, erythema, ischemia, and infection, consistent with long-standing color-based wound classification frameworks.1 In many clinical settings, wound photographs serve as an adjunct to in-person assessment rather than as a substitute for direct examination; however, the role of such photographs is more influential in telemedicine, remote monitoring, longitudinal documentation, interdisciplinary consultation, the research context, and artificial intelligence (AI) performance.5–8
Despite this central role, contemporary wound photography lacks any objective, measurable assessment of image accuracy. Quantitative investigations demonstrate that uncalibrated wound photographs frequently exhibit substantial and inconsistent color distortion, particularly in red and yellow ranges, which are critical for assessing granulation tissue, slough, inflammation, erythema, and ischemia.9,10
Historically, medical photography was performed by trained professionals using controlled lighting and standardized acquisition techniques, but as this practice diminished, image capture shifted to clinicians and patients using consumer smartphones and digital cameras,11,12 thus increasing the variability in wound photo documentation. Human vision automatically adapts to changes in room lighting, allowing clinicians to perceive tissue color consistently, but cameras and smartphones do not adjust in the same way. As a result, the same wound can appear different depending on lighting conditions, device type, or camera settings.
Instead of describing color with words such as “redder” or “darker,” computers describe color using numbers. Systems, such as red, green, and blue (RGB) or hue, saturation, and value, assign numeric values to color components and brightness so the same color can be identified, compared, and corrected consistently across images.13,14 Thus, when lighting or camera processing changes, those numbers change, even if the wound itself does not. Measuring color numerically makes it possible to measure and correct color differences, a process known as color calibration.10,15
Color calibration aims to ensure that a wound photograph accurately reflects the tissue appearance observed at the point of care and can be interpreted consistently by other clinicians over time.11,16,17 In clinical photography, calibration is achieved by incorporating a small color reference target with known, fixed numeric values into the photographic field adjacent to the wound.15,18 The reference target provides a stable colorimetric anchor against which the captured image can be evaluated. When calibration methods are applied, measured color values from the reference target are compared with their defined standards, allowing global correction of the image so that displayed colors more closely correspond to their intended values.7,13,15 Because the same correction is applied across the image, tissue colors within the wound are adjusted simultaneously under the same transformation, improving color fidelity and reducing acquisition-related artifact.18,19 This approach supports more consistent color interpretation, minimizes artifactual appearance of change over time, and strengthens the reliability of wound photographs as components of the clinical record.20–23
Even without dedicated color calibration software, placing a color reference chart within a wound photograph provides 2 practical benefits for color accuracy. First, the reference target supplies a fixed colorimetric anchor that supports more reliable color correction at capture through custom white balance or during pos-tprocessing, rather than relying solely on uncontrolled automatic camera settings.10,15,24,25 Second, the visible reference chart allows clinicians to visually judge whether the reference colors appear plausible and internally consistent, providing a practical visual gauge of color accuracy in the wound image.26–29
Color accuracy in digital images can be quantified using CIE ΔE, a standardized metric describing the perceptual difference between colors in CIELAB color space. Lower ΔE values indicate closer correlation between photographed color and visual observation, whereas higher values indicate increasing color distortion that may alter clinical interpretation.13 Human perceptual studies and CIE guidance establish that ΔE values below 1 are generally imperceptible, values between 1 and 2 are barely perceptible under controlled viewing, values between 2 and 3 are perceptible to trained observers, values between 3 and 5 are clearly visible, and values above 5 represent obvious color mismatch.13,30
In digital pathology, dermatology, and medical photography, color fidelity and reproducibility are recognized as essential to reliable interpretation, and ΔE-scale differences are used to quantify image variability and workflow performance.13,17,21,22,27 These fields commonly target color differences on the order of only a few ΔE units to preserve diagnostic reliability. Wound-specific standards for acceptable ΔE have not been formally codified.
The absence of objective accuracy measurement represents a potential and often unmeasured source of variability in wound care. In contrast to other medical imaging modalities, such as radiology, pathology, and ophthalmic imaging, wound photography provides no standardized verification of image fidelity, no minimum acceptable accuracy threshold, and no expert-defined quality signal.16,21,22
The present review examines the use of wound photography in clinical care, focusing on evidence related to color accuracy, sources of photographic variability, and the role of standardized acquisition and color calibration in reducing artifact where photographic interpretation is relied upon.
Methods
A structured narrative literature review was conducted to evaluate wound photography, color accuracy in medical imaging, tissue-color interpretation, and image integrity in clinical documentation. Searches were performed in PubMed/MEDLINE, Scopus, Web of Science, and Google Scholar for literature published between 1990 and 2024, supplemented by forward and backward citation chaining from foundational articles. Search terms combined MeSH and free-text keywords related to “wound photography, “color calibration” (including CIELAB and ΔE), tissue color assessment, smartphone and telemedicine imaging, and medicolegal image documentation.
Inclusion criteria included original research, systematic reviews, peer-reviewed research, consensus guidelines, and validated technical methods directly relevant to wound or skin imaging and providing sufficient methodological detail to assess imaging reliability or clinical applicability. Studies were excluded if they addressed nonclinical or cosmetic photography, lacked extractable imaging or color-
accuracy methodology, or represented duplicate or derivative publications without novel findings.
Article screening and data extraction were performed independently by 2 reviewers (F.G.J. and J.W.) with iterative refinement of inclusion criteria to ensure technical and clinical relevance, and to screen out materials not written in the English language. One reviewer (F.G.J.) is an independent medical color expert who founded TRUE-See Systems, writing the foundational patents for color calibration and collaborating with clinicians and researchers for 15 years to improve photo integrity and accuracy in medical photos. The other reviewer (J.W.) is an instructor at the University of Louisiana at Lafayette with a PhD in affective virtual reality and postdoc research in medical robotics and imagery analysis. Findings were synthesized narratively, with quantitative outcomes reported as described in the original publications rather than pooled or meta-analyzed.
Results
The literature search identified 427 records, with 311 unique articles remaining after duplicate removal and screening by title and abstract. Two hundred twenty-one records were excluded for clinical irrelevance or absence of imaging or color-related data.
Ninety full-text articles were reviewed in detail. Of these 90, only 22 studies contained sufficient methodological rigor and quantitative data to directly address the current review’s questions regarding color accuracy, reliability, and clinical interpretation in wound care photography. Newly identified references from the extended search of forward and backward citation chaining from foundational articles were tracked separately to maintain traceability between previously established evidence and newly added literature.
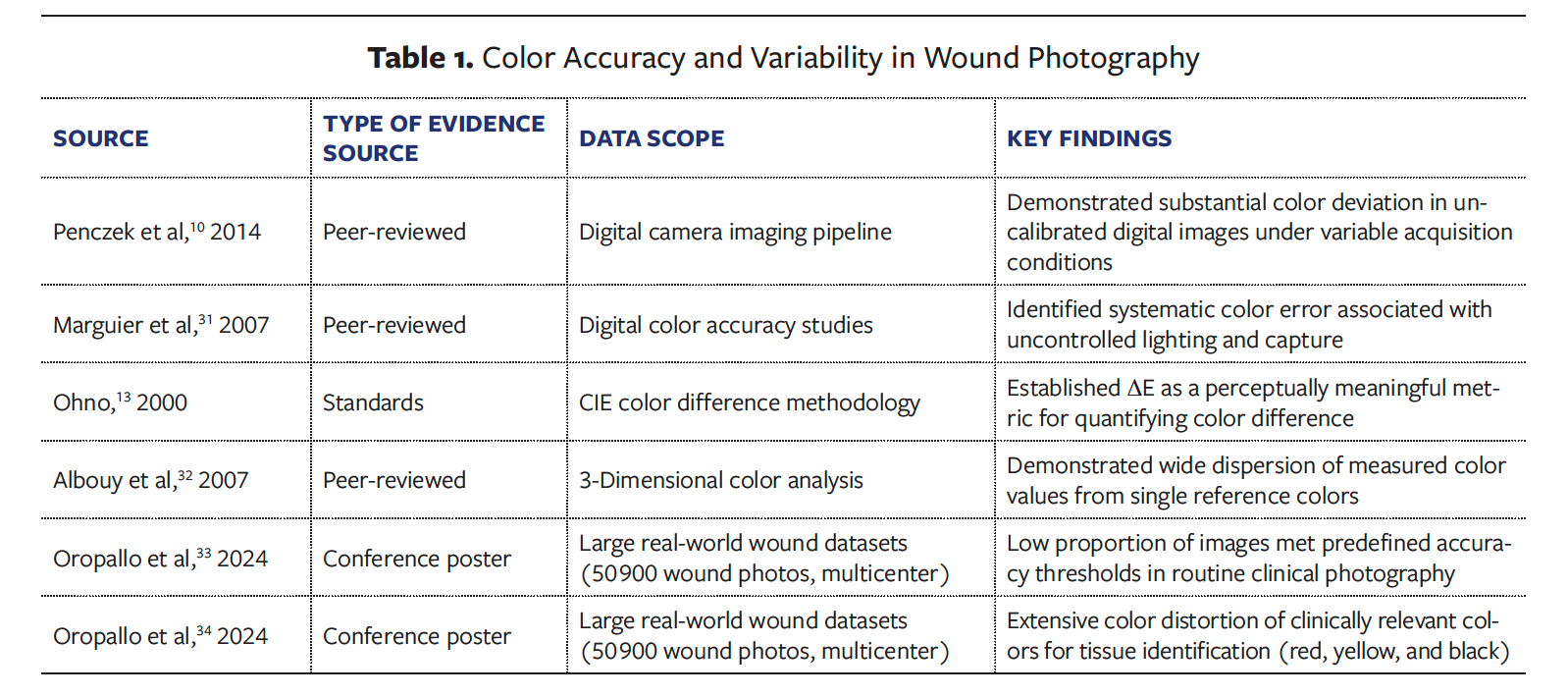
Across peer-reviewed, standards-based, and real-world observational studies, uncalibrated wound photographs demonstrated substantial color deviation, characterized by systematic color error under uncontrolled acquisition conditions typical of clinical practice.10,13,31–34 Quantitative analyses consistently showed wide dispersion of measured color values originating from single, known reference targets, indicating instability rather than random noise.
Standards-based investigations validated CIE ΔE as a perceptually relevant and technically appropriate metric for quantifying these deviations. When applied to clinical datasets, a low proportion of images met predefined accuracy thresholds, with greater than or equal to 50% deviation from target color values commonly observed.33–35 Color error was not uniformly distributed; instead, extensive RGB dispersion was most pronounced in red, yellow, and black tissue colors, which are central to wound classification and clinical decision-making (Table 1).10,13,31–34
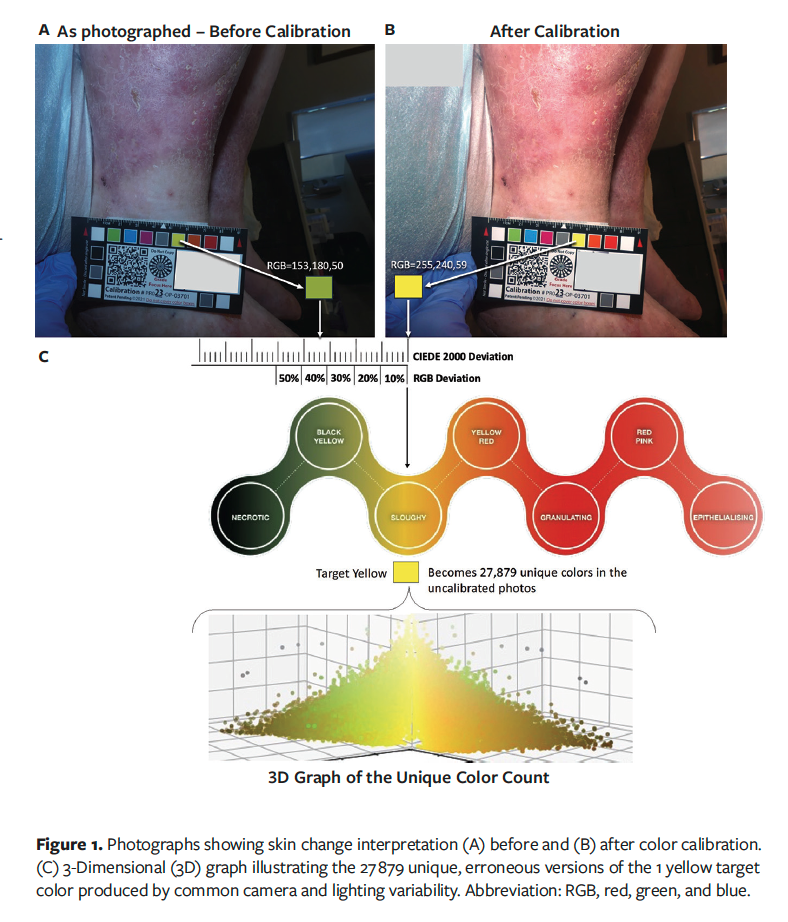
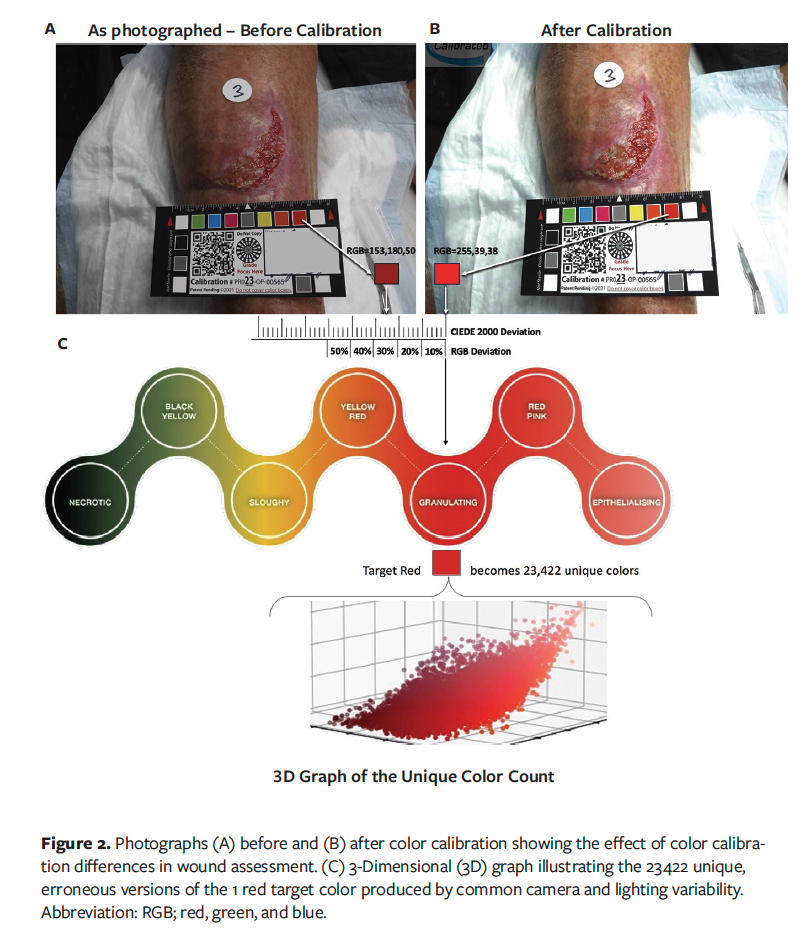
Three-dimensional color plotting demonstrated that across 50 900 wound photographs, a single clinically relevant reference color (eg, yellow or red) was reproduced as tens of thousands of distinct and erroneous colors, indicating substantial dispersion relative to the known reference (Figures 1 and 2).34 Multiple peer-reviewed and conference-derived datasets demonstrated that standardized image acquisition techniques combined with color calibration using reference targets produce substantial and clinically meaningful reductions in color error (Table 2).15,16,18,35–37
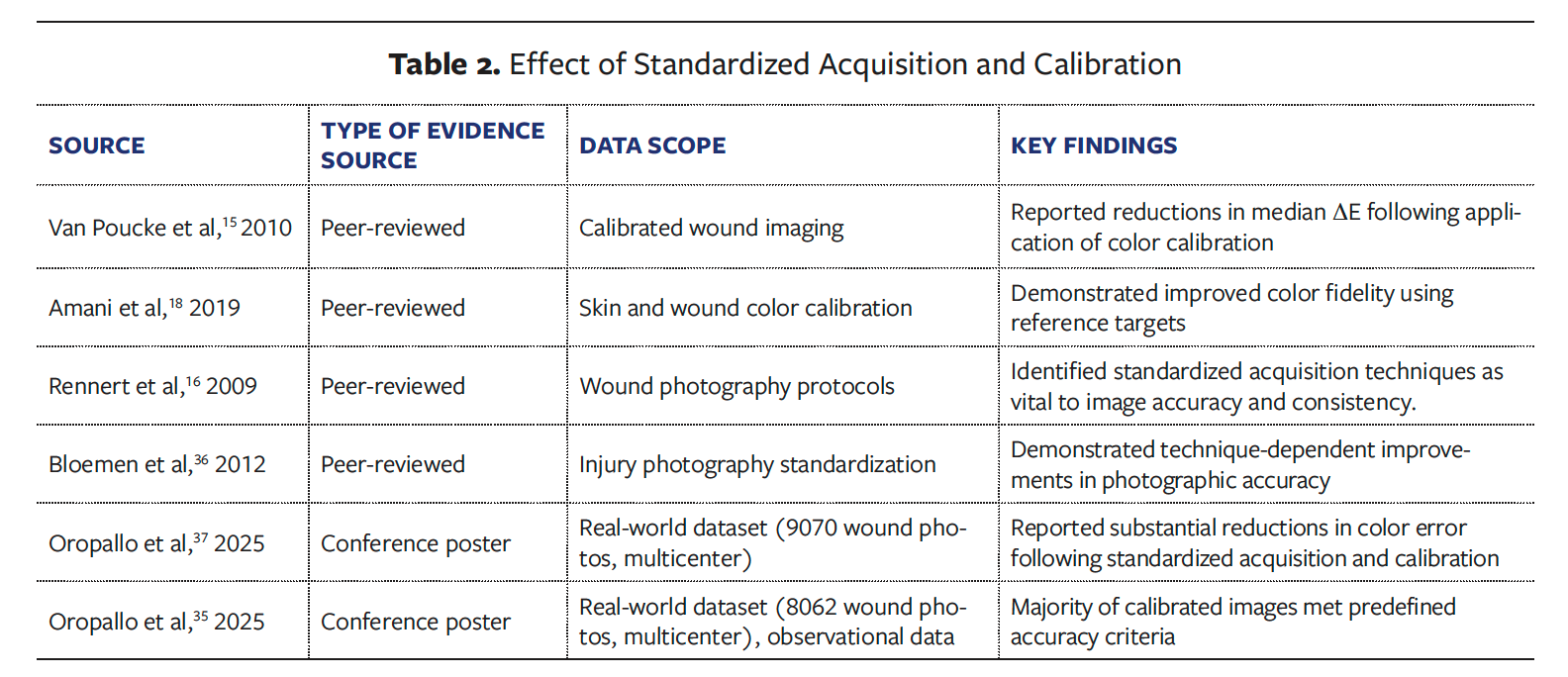
Across large real-world datasets, calibration was associated with marked reductions in mean ΔE. In these datasets, most calibrated images met predefined accuracy thresholds, whereas uncalibrated images did so infrequently. Reported mean ΔE values decreased from 21.6 in uncalibrated images to 5.8 following calibration in conference-reported analyses.37 These improvements reflected enhanced color fidelity across wound and skin types and were strongly technique dependent, with acquisition consistency identified as a key determinant of reproducible accuracy. While calibration alone improved performance, the most reliable and sustained accuracy was observed when calibration was paired with standardized capture practices, enabling the majority of wound photographs to meet predefined accuracy thresholds and supporting reproducible color interpretation at scale (Table 2).
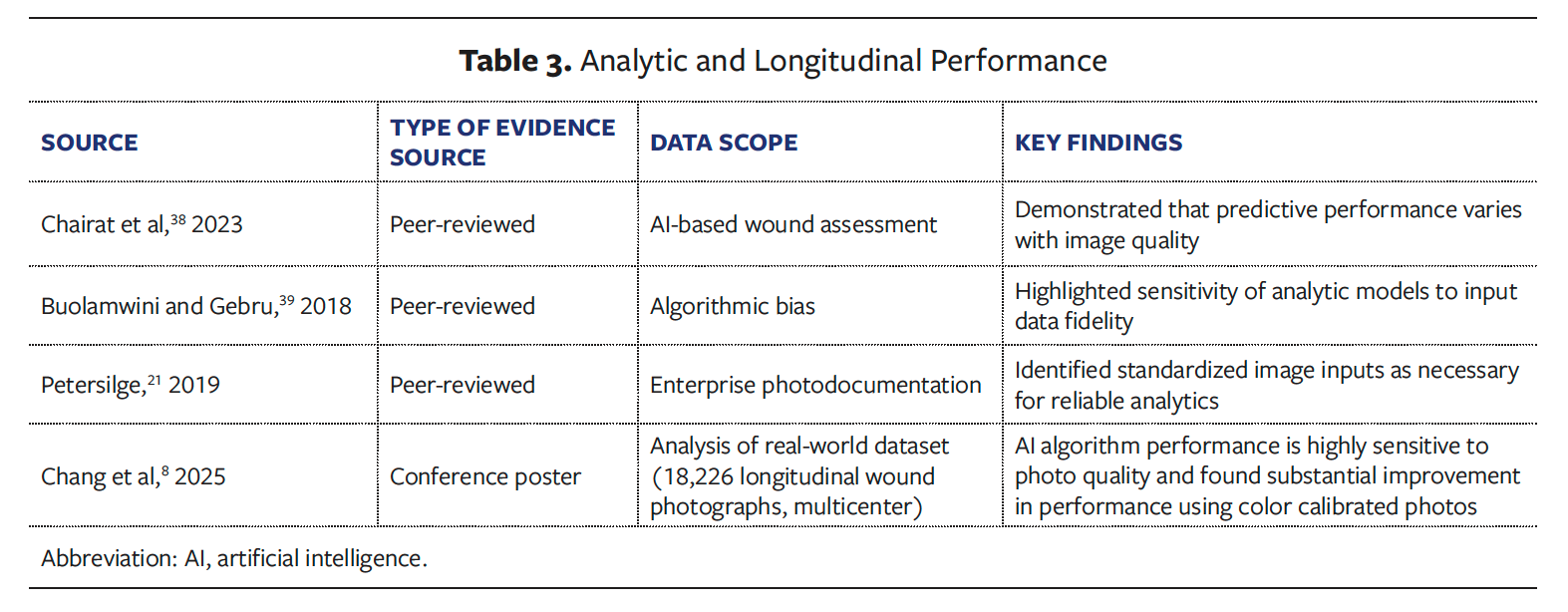
Evidence evaluating analytic and longitudinal applications of wound photography consistently identified image fidelity as a key determinant of performance, including in AI performance. A conference poster reported moderate overall predictive performance for short-term wound progression, with overall discrimination of an approximate area under the curve of 0.71, and analyses demonstrated clear sensitivity to baseline image quality.8 Large observational datasets further showed stratified performance gains as image color accuracy improved, with increases of up to about 12% and with the largest gains observed in lower-quality image strata. Standards-based guidance and algorithmic bias literature similarly emphasized the importance of standardized, high-fidelity image inputs to ensure reliable and reproducible analytic performance over time (Table 3).8,21, 38–39
Clinical studies evaluating wound image interpretation and documentation demonstrated divergent clinical assessments when photographs of the same wound were obtained during a single visit under nonstandardized imaging conditions, highlighting substantial interpretation variability from nonstandardized images (Table 4).11,40–45 Across studies, there was marked variability in photo-derived wound metrics, including large changes in photo-derived wound area and volume over time, even when no corresponding clinical change was documented.
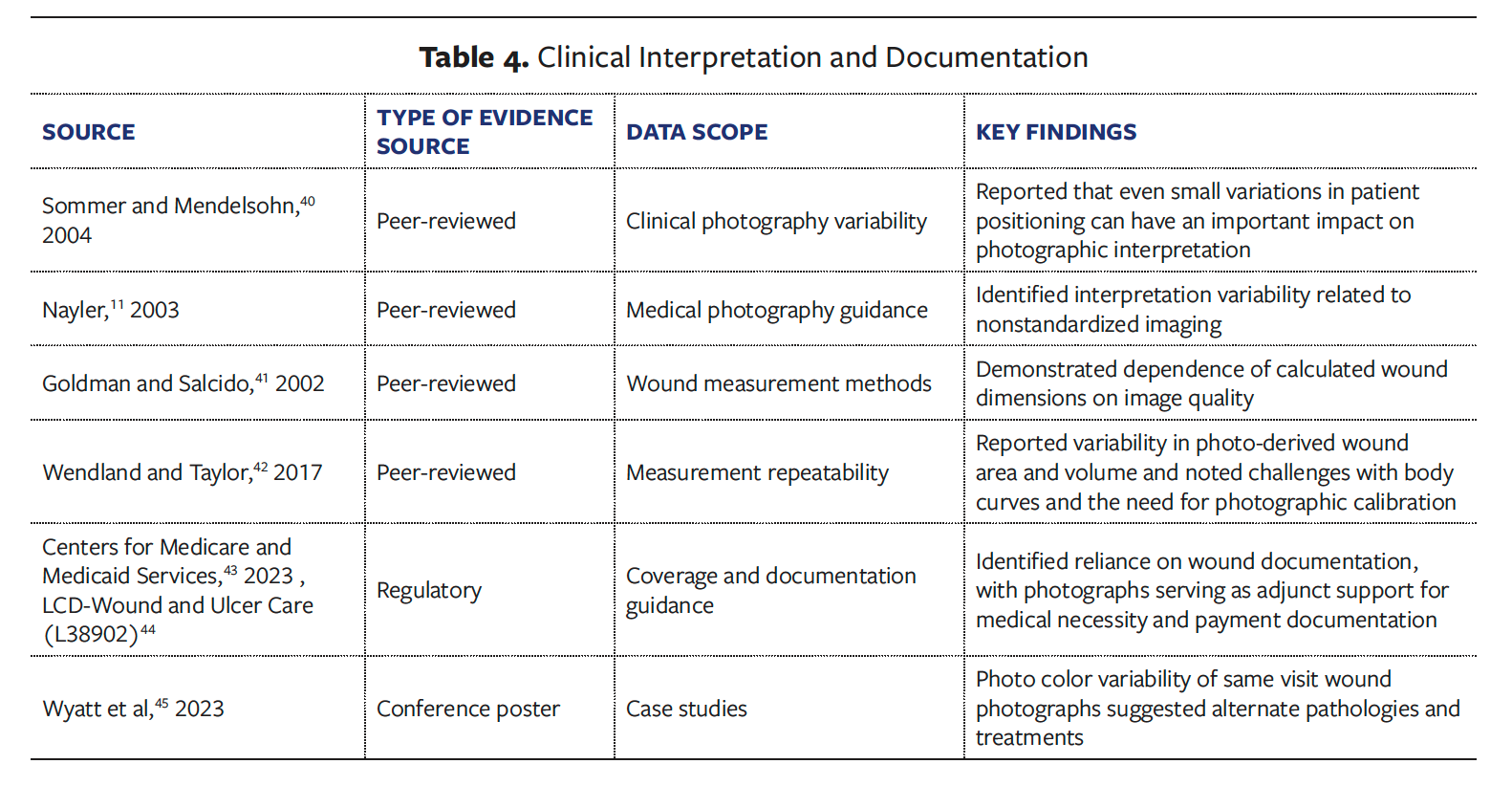
Wound measurement-focused investigations further showed that calculated wound dimensions were highly dependent on image quality, with dependence of calculated dimensions on photographic technique, lighting, and image resolution producing inconsistent measurements across time points. In parallel, regulatory and payer guidance emphasized the reliance on photographs for determinations of medical necessity and reimbursement, which carry clinical and administrative implications.
Discussion
Across peer-reviewed studies, standards, and large observational analyses, color inaccuracy in wound photography emerges as a systematic and measurable phenomenon. Digital imaging literature has long documented color distortion arising from automated camera processing and uncontrolled acquisition conditions.10,31,41 The present literature review demonstrates that these effects persist in wound care and are evident at scale.15,33–35
Evidence consistently indicates that acquisition technique is a critical determinant of accuracy. Calibration alone is insufficient unless it is paired with standardized capture conditions controlling distance, angle, focus, and lighting.16,17 Objective metrics, such as ΔE, are validated across dermatologic and medical imaging applications and provide a reproducible framework for assessing photographic fidelity.46 Analytic studies show that image fidelity directly affects predictive performance, consistent with broader medical AI literature demonstrating sensitivity to input data quality and standardization.8,38 Clinical variability studies further show that photographic inconsistency alone can influence interpretation.
Wound-focused studies and conference posters further demonstrate that nonstandardized photography frequently exhibits substantial color error, while the introduction of standardized acquisition protocols and colorimetric calibration can meaningfully reduce variability and improve consistency.15,16,37 Taken together, this body of evidence suggests that lower ΔE values, similar to those targeted in other medical imaging fields, are associated with improved consistency and interpretability in wound photography, although wound-specific thresholds have not yet been formally established.
Emerging evidence indicates that standardized image acquisition combined with use of a color reference and color calibration substantially reduces color error and improves agreement between photographic and live wound assessment.15,35,37,46 Together, these findings highlight the potential value of expert-driven approaches to defining and communicating photographic accuracy in wound care.
Limitations
Several limitations should be considered when interpreting this review. It was conducted as a structured narrative review rather than a formal systematic review or meta-analysis, and therefore the findings reflect narrative synthesis rather than pooled quantitative estimates. Although the search strategy included multiple biomedical databases and citation chaining, this does not completely remove any potential selection bias and interpretive limitations inherent in reviewing an emerging, interdisciplinary topic. In addition, the review was limited to English-language sources.
Similarly, as this is an emerging, interdisciplinary topic, the underlying evidence base was heterogeneous, including peer-reviewed studies, standards documents, consensus guidance, and conference-reported observational datasets, with variability in imaging methods, calibration approaches, outcome measures, and overall rigor. This heterogeneity limited direct comparison across studies and precluded formal meta-analysis. Conference-reported findings were included as corroborative evidence where wound-specific peer-reviewed data were limited. Finally, although article screening and data extraction were performed independently by 2 reviewers, some degree of interpretive bias remains possible.
Conclusion
Collectively, the literature demonstrates that wound photography has become an increasingly measurement-dependent clinical modality without commensurate accuracy standards. Color inaccuracy is prevalent, quantifiable, and consequential across clinical interpretation, documentation reliability, and analytic and AI performance.10,15,8,39 Evidence from peer-reviewed studies, standards, and large real-world datasets, including analyses reported at conferences, consistently shows that standardized acquisition and objective assessment of color accuracy substantially improve photographic fidelity. Aligning wound photography with the objective standards applied to other medical imaging modalities represents a practical, evidence-supported pathway to improve reliability as the clinical and analytic use of photographic data continues to grow.
Author and Public Information
Authors: Francis G. James, SOC1; Alisha Oropallo, MD1-4; Jason Woodworth, PhD5; Vickie Driver, DPM1,6; Courtney Pina, MD3; Peggy Dotson, RN, BS1; Oscar Alvarez, PhD7-8
Affiliations: 1Wound Care Collaborative Community, Orlando, FL; 2Danbury Hospital, Department of Vascular and Endovascular Surgery, Danbury, CT; 3Donald and Barbara Zucker School of Medicine, Hempstead, NY; 4Northwell Health, Lake Success, NY; 5University of Louisiana-Lafayette, Lafayette, LA; 6University of Washington, Seattle, WA; 7University of Miami, Miami, FL; 8Rutgers University, New Brunswick, NJ
Disclosures: F.G.J. is the Founder of TRUE-See Systems, Inc. The other authors have no financial or other conflicts of interest to disclose.
Author contributions: F.G.J. and J.W. independently performed article screening and data extraction with iterative refinement of inclusion criteria to ensure technical and clinical relevance. All authors contributed to the conception and design of the work and to the critical review of the manuscript ensuring accuracy of the data presented.
Ethical Approval: No ethical approval was required for the literature review.
Correspondence: Francis G. James, SOC; Medical Color Intelligence, 72 A Main Street, Westford, MA 01886; 504-813-8440; medicalcolorintelligence@gmail.com
Manuscript Accepted: March 6, 2026
References
1. Stotts NA. Seeing red and yellow and black. The three-color concept of wound care. Nursing. 1990;20(2):59-61.
2. Gray D, White RJ, Cooper P, Kingsley A. Applied wound management: part 3. Use in practice. (2010). Accessed September 16, 2025. https://wounds-uk.com/applied-wound-management/applied-wound-management-supplement-part-3/
3. Gray D, White RJ, Cooper P. Understanding Applied Wound Management. Br J Community Nurs. 2002;7(Sup4):15-19. doi:10.12968/bjcn.2002.7.Sup4.12616
4. Armstrong DG, Bauer K, Bohn G, Carter M, Snyder R, Serena TE. Principles of Best Diagnostic Practice in Tissue Repair and Wound Healing: An Expert Consensus. Diagnostics (Basel). 2020;11(1):50. doi:10.3390/diagnostics11010050
5. Ayello EA, Capitulo KL, Fife CE, et al. Legal issues in the care of pressure ulcer patients: key concepts for health care providers: a consensus paper from the international expert wound care advisory panel. J Palliat Med. 2009;12(11):995-1008. doi:10.1089/jpm.2009.9939
6. Ayello EA. Pressure Ulcer Staging. Presented at the IRF Provider Training; May 12, 2014, Baltimore, MD. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/IRF-Quality-Reporting/Downloads/IRF-QRP-Training-%E2%80%93-PrU-Staging-May-12-2014-.pdf
7. Scheinfeld N. Photographic images, digital imaging, dermatology, and the law. Arch Dermatol. 2004;140(4):473-476. doi:10.1001/archderm.140.4.473
8. Chang P, Gohil S, Reed A, Oropallo A, Carpenter S. A deep learning model for predicting wound healing using color-calibrated imaging. Poster presentation presented at: International Post-Acute Woundcare Society Summit; September 11, 2025.
9. Cronin A, Tkaczyk ER, Hussain I, Bowden A, Saknite I. Effect of camera distance and angle on color of diverse skin tone-based standards in smartphone photos. J Biophotonics. 2023;16(6):e202200381. doi:10.1002/jbio.202200381
10. Penczek J, Boynton PA, Splett JD. Color error in the digital camera image capture process. J Digit Imaging. 2014;27(2):182-191. doi:10.1007/s10278-013-9644-1
11. Nayler JR. Clinical photography: a guide for the clinician. J Postgrad Med. 2003;49(3):256-262.
12. Collection: Stanley B. Burns, M.D., historic medical photography collection | Archives at Yale. Accessed January 27, 2026. https://archives.yale.edu/repositories/10/resources/11880
13. Ohno Y. CIE fundamentals for color measurements. In: Proceedings of the IS&T International Conference on Digital Printing Technologies (NIP16). 2000:540-545. doi:10.2352/ISSN.2169-4451.2000.16.1.art00033_2
14. Prasad S, Roy B. Digital photography in medicine. J Postgrad Med. 2003;49(4):332-336.
15. Van Poucke S, Vander Haeghen Y, Vissers K, Meert T, Jorens P. Automatic colorimetric calibration of human wounds. BMC Med Imaging. 2010;10:7.. doi:10.1186/1471-2342-10-7
16. Rennert R, Golinko M, Kaplan D, Flattau A, Brem H. Standardization of wound photography using the wound electronic medical record. Adv Skin Wound Care. 2009;22(1):32-38. doi:10.1097/01.ASW.0000343718.30567.CB
17. Finnane A, Curiel-Lewandrowski C, Wimberley G, et al; International Society of Digital Imaging of the Skin (ISDIS) for the International Skin Imaging Collaboration (ISIC). Proposed technical guidelines for the acquisition of clinical images of skin-related conditions. JAMA Dermatol. 2017;153(5):453-457. doi:10.1001/jamadermatol.2016.6214
18. Amani M, Falk H, Jensen OD, Vartdal G, Aune A, Lindseth F. Color calibration on human skin images. In: Tzovaras D, Giakoumis D, Vincze M, Argyros A, eds. Computer Vision Systems. ICVS 2019. Lecture Notes in Computer Science, vol 11754. doi:10.1007/978-3-030-34995-0_20
19. Maglogiannis I, Kosmopoulos DI. A system for the acquisition of reproducible digital skin lesions images. Technol Health Care Off J Eur Soc Eng Med. 2003;11(6):425-441.
20. Duysburgh P, Jacobs A. The Use of Calibrated Photos for Wound Care in a Home Care Setting. D3.5: Wound Care System Scenarios for Home Care. Unknown; 2011.
21. Petersilge CA. Fundamentals of enterprise photodocumentation: connecting the clinical and technical. A review of key concepts. J Digit Imaging. 2019;32(6):1052-1061. doi:10.1007/s10278-019-00212-4
22. Petersilge CA, McDonald J, Bishop M, Yudkovitch L, Treuting C, Towbin AJ. Visible light imaging: clinical aspects with an emphasis on medical photography—a HIMSS-SIIM Enterprise Imaging Community whitepaper. J Digit Imaging. 2022;35(3):385-395. doi:10.1007/s10278-022-00584-0
23. Wiedemann LA. Using clinical photos in EHRs. J AHIMA. 2010;81(4):44-45.
24. How to Set In-Camera White Balance. X-Rite. Accessed February 1, 2026. https://www.xrite.com/service-support/how_to_set_incamera_white_balance?utm_source=chatgpt.com
25. Color Rendition Chart-TE188. October 13, 2025. Accessed October 13, 2025. https://image-engineering.de/products/charts/all/516-te188
26. Krupinski EA. Current perspectives in medical image perception. Atten Percept Psychophys. 2010;72(5):10.3758/APP.72.5.1205. doi:10.3758/APP.72.5.1205
27. Krupinski EA, Silverstein LD, Hashmi SF, Graham AR, Weinstein RS, Roehrig H. Observer performance using virtual pathology slides: impact of LCD color reproduction accuracy. J Digit Imaging. 2012;25(6):738-743. doi:10.1007/s10278-012-9479-1
28. ColorChecker® Classic. X-rite. October 14, 2025. Accessed October 14, 2025. https://calibrite.com/us/product/colorchecker-classic/
29. Defining a Realistic Pass/Fail Tolerance | X-Rite Blog. X-Rite. October 14, 2025. Accessed October 14, 2025. https://www.xrite.com/blog/tips-to-define-tolerances
30. Mokrzycki W, Tatol M. Color difference Delta E - A survey. ResearchGate. Accessed October 2, 2025. https://www.researchgate.net/publication/236023905_Color_difference_Delta_E_-_A_survey
31. Marguier J, Bhatti N, Baker H, Harville M, Süsstrunk S. Assessing human skin color from uncalibrated images. Int J Imaging Syst Technol. 2007;17(3):143-151. doi:10.1002/ima.20114
32. Albouy B, Lucas Y, Treuillet S. 3D modeling from uncalibrated color images for a complete wound assessment tool. Annu Int Conf IEEE Eng Med Biol Soc. 2007;2007:3323-3326. doi:10.1109/IEMBS.2007.4353041
33. Oropallo A, Alvarez O, Wyatt H, Woodworth JW, Dotson P, Weir D. Measuring color accuracy of wound photographs. ePoster presented at: Symposium of Advanced Wound Care Spring meeting; May 14-18, 2024; Orlando, FL.
34. Oropallo A, Alvarez O, Wyatt H, Woodworth J, Dotson P, Weir D. 3D plotting of wound photos inaccuracy. Spring SAWC 2024. Published online May 18, 2024.
35. Oropallo A, Alvarez O, Dotson P, Carpenter S, Franzen-Korzendorfer H, James F. A Medical photo color accuracy score. Poster presentation presented at: International Post-Acute Woundcare Society Summit; September 11, 2025.
36. Bloemen EM, Rosen T, Schiroo JAC, et al. Photographing injuries in the acute care setting: development and evaluation of a standardized protocol for research, forensics, and clinical practice. Acad Emerg Med Off J Soc Acad Emerg Med. 2016;23(5):653-659. doi:10.1111/acem.12955
37. Oropallo A, Dotson P, Franzen-Korzendorfer H, Cole W, Alexander BD, Driver VR. Standardizing medical photo acquisition to improve image quality. ePoster presented at: Symposium of Advanced Wound Care Spring meeting; April 30-May 3, 2025; Grapevine, TX.
38. Buolamwini J, Gebru T. Gender shades: intersectional accuracy disparities in commercial gender classification. In: Proceedings of Machine Learning Research. 2018;81:1-15.
39. Chairat S, Chaichulee S, Dissaneewate T, Wangkulangkul P, Kongpanichakul L. AI-Assisted Assessment of Wound Tissue with Automatic Color and Measurement Calibration on Images Taken with a Smartphone. Healthcare. 2023;11(2):273. doi:10.3390/healthcare11020273
40. Sommer DD, Mendelsohn M. Pitfalls of nonstandardized photography in facial plastic surgery patients. Plast Reconstr Surg. 2004;114(1):10-14. doi:10.1097/01.prs.0000127791.31526.e2
41. Goldman RJ, Salcido R. More than one way to measure a wound: an overview of tools and techniques. Adv Skin Wound Care. 2002;15(5):236-243. doi:10.1097/00129334-200209000-00011
42. Wendland DM, Taylor DWM. Wound measurement tools and techniques: a review. J Acute Care Phys Ther. 2017;8(2):42-57. doi:10.1097/JAT.0000000000000050
43. Centers for Medicare and Medicaid Services. 2023 Medicare Fee-for-Service Supplemental Improper Payment Data. Published December 7, 2023. Accessed September 18, 2025. https://www.cms.gov/data-research/monitoring-programs/improper-payment-measurement-programs/comprehensive-error-rate-testing-cert/cert-reports/2023-medicare-fee-service-supplemental-improper-payment-data
44. LCD - Wound and Ulcer Care (L38902). Accessed March 20, 2026. https://www.cms.gov/medicare-coverage-database/view/lcd.aspx?lcdid=38902
45. Wyatt H, Perez-Clavijo F, Van Meter K, James F. What is the Standard for Wound Care Photography? Spring SAWC 2023. Published online April 30, 2023.
46. Raina A, Hennessy R, Rains M, et al. Objective measurement of erythema in psoriasis using digital color photography with color calibration. Skin Res Technol. 2016;22(3):375-380. doi:10.1111/srt.12276