



Efficacy of Rhizophora mangle Cream in Venous Ulcer: A Randomized Controlled Clinical Trial
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Compression therapy is the primary treatment for venous ulcers (VU). Topical treatments are used as an adjunct to accelerate healing, but they can be costly, and there is currently no standard medication. Objective. To evaluate reduction in venous ulcer area in patients treated with 5% aqueous extract of Rhizophora mangle L. leaves in cream form. Methods. Patients were randomized into 2 groups: the experimental group (EG) (55 ulcers) received 5% Rhizophora mangle cream, and the control group (CG) (45 ulcers) received medium chain triglyceride oil. Ulcers were evaluated using the MEASURE (measurement, exudate, appearance, suffering, weakening, reassess, edge) methodology, and area was measured using software on day 1, 4 weeks, 8 weeks, and 12 weeks. Results. At 12 weeks, the EG showed a mean 51.69% reduction in ulcer area (mean [SD] 3.97 [6.18] cm²), whereas the CG exhibited lesion worsening, with a mean increase in ulcer area corresponding to a −187.82% variation (mean [SD], 12.17 [20.17] cm²). Complete healing was observed in 34.5% of ulcers in the EG compared with 15.6% in the CG (P = .002). Furthermore, the EG demonstrated greater improvement across all clinical ulcer parameters than the CG. Conclusion. The 5% Rhizophora mangle cream was effective in venous ulcer area reduction and clinical healing, which suggests that it may be an effective an alternative treatment for venous ulcers in the lower limbs.
Compression therapy is the main treatment for venous ulcer (VU).1 This complex presentation necessitates the involvement of highly qualified multidisciplinary teams, whose expertise often entails substantial financial costs.2 The ability to predict the failure of compression therapy in the treatment of VUs may aid in the identification of patients who are suitable candidates for adjunctive topical interventions.3 Topical treatment of VUs aids healing; however, there is no standard therapy, and numerous products can be used to manage VU.4 These products can be used for debridement (eg, collagenase, hydrogel)4,5 or to provide absorption, reduce odor, protect wounds from mechanical injuries, or prevent maceration of the surrounding skin and thereby stimulate healing, such as coverings and dressings (eg, cellulose acetate).6-8
For centuries, traditional medicine has used plant extracts to treat wounds. Rhizophora mangle L. (R. mangle), or red mangrove, is an endemic component of mangrove ecosystems and is a representative species of the Rhizophoraceae Pers Family.9 The pharmacological properties of the plant in traditional medicine arise from the presence of secondary compounds such as tannins, flavonoids, saponins, and terpenes; tannins and flavonoids are important for wound healing.10,11
The wound-healing potential of R. mangle extract has been evaluated in preclinical studies10,11 and preliminary clinical trial,12 based on previous publications that showed anti-inflammatory action13,14 and antioxidant activity,15 as well as stimulation of epithelialization,16 and neovascularization,17 without reports of toxicities.18 Thus, the current study aimed to evaluate VU area reduction in patients treated with cream made from 5% aqueous extract of R. mangle leaves.
Methods
The methods used in this study were approved by the Research Ethics Committee of Federal University of Pernambuco, Recife, Brazil (process number 5.535.377) and were registered in the Brazilian Registry of Clinical Trials (ReBEC) (process number RBR-106nvs7h). The methods follow international ethical guidelines (Declaration of Helsinki, Council for International Organizations of Medical Sciences [CIOMS] International Guidelines for Biomedical Research Involving Human Subjects) and Brazilian ethical guidelines (Res. CNS 466/12 and complementary). Written informed consent was obtained from all subjects involved in the study.
Preparation of R. mangle cream
The leaves of R. mangle were collected in the mangrove forest of the city of Itamaracá, district of Vila Velha, Pernambuco, Brazil, at latitude 7°40' south and longitude 34°50' west. The species was deposited in the Herbarium of the Federal University of Pernambuco (number UFPE: 69.655). The collection was authorized by the Pernambuco Environmental Pollution Control and Water Resources Administration Company under authorization from CA DFRB N. 120/2014. The leaves (500 g) were dried at 35 °C for 72 hours and then ground to a size of 0.177 mm in a variable speed rotor mill Pulverisette 14 classic line (Fritsch GmbH). The aqueous extract was obtained by infusion (40 °C for 10 minutes). The material was filtered and stored at 5 °C.19 The cream was formulated according to the proportion of anionic emulsion base (855 g) and aqueous extract of R. mangle (45 mL). The components of the cream were homogenized and were yellowish in color, with pH of 5.5. The total amount of the cream was portioned into 30-g containers.
The cream was developed at the Federal University of Pernambuco under controlled conditions. The compounded preparations were subjected to sterility and endotoxin testing, as well as physicochemical characterization, to ensure their purity and quality.
Study protocol
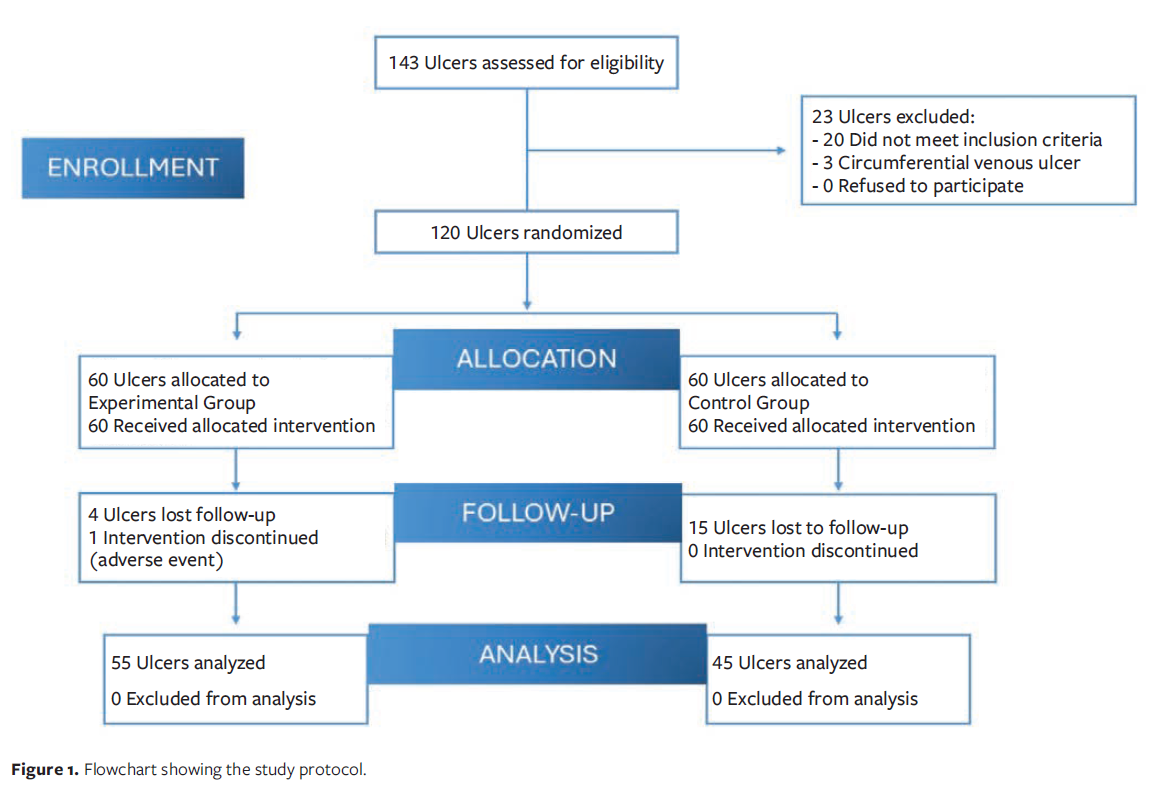
The study protocol is shown in Figure 1. This study is a randomized, controlled, masked, parallel, phase 2 trial with consecutive sampling in patients with VU of the lower limbs. It was carried out from August 1, 2022, to February 4, 2024, and patients signed the Free and Informed Consent Form and the Authorization for Use of Images. The study was conducted in the outpatient clinic of the Angiology and Vascular Surgery Service of the Clinics Hospital of the Federal University of Pernambuco.
The inclusion criteria were patients aged 18 years or older with acute or chronic VU (Clinical-Etiology-Anatomy-Pathophysiology [CEAP] 6). Patients with ulcers of other or mixed etiologies, with circumferential ulcers, or who experienced an adverse event to the medications provided were excluded.
The ulcers were randomized to either the experimental group (EG), which received 5% R. mangle cream, or the control group (CG), which received conventional treatment with medium chain triglyceride oil. Simple randomization was done in Excel 2019 (Microsoft) by recruiting researchers (Lopes, NA; Pinheiro, GRC; Crusco, VS; Segatti, CB; Freitas Filho, LEP; Carneiro, PHVS) who were not involved in evaluating the study results. These researchers were instructed not to disclose the planned intervention to the evaluating researcher or to any of the patients or other researchers involved in the study until after its completion.
Patients were not completely masked because the treatment vehicles were different, with the CG receiving an oil and the EG a cream. Because there was no placebo group, patients were informed that they would receive a treatment; however, in an effort to reduce bias to the extent possible, patients did not know which group the drug studied was in. The researcher (Sa, JGA) evaluating the outcome was masked throughout the study. Allocation secrecy was achieved through the use of sequentially numbered, sealed opaque 60-lb envelopes.
On day 1 (D1), a form was filled out with patient history, anthropometric data, and information about ulcer appearance. The ulcer was then clinically assessed using the MEASURE (measurement, exudate, appearance, suffering, weakening, reassess, edge) methodology.20 Wound photographs were taken using a standardized process, using a dual-lens (ultra-wide and wide-angle) camera placed 15 cm from the ulcer to obtain a 12-megapixel image. The iPhone 11 (Apple Inc) was set to ƒ/1.8 opening, and a 150-mm, 6-inch digital caliper (Digimess) was used for scale for later calibration of the ImageJ software.
In each group, the first treatment application was done by the medical team, who provided study participants with instructions and guidance on how to administer the cream or gel at home. First, the ulcer was cleansed with 0.9% saline solution. Second, the cream or oil was applied, and then a secondary sterile gauze dressing and bandage were placed. Finally, a compressive elastic band was placed. Participants in both groups were instructed to apply the respective substance (oil or cream) once a day, every day. All patients used medium-compression elastic stockings (20 mm Hg-30 mm Hg) for 8 hours a day during the study. Participants were provided with standardized instructions regarding study procedures and conduct, as well as a contact telephone number to report any local or systemic adverse events or to address study-related questions. Participants returned to the outpatient clinic for follow-up evaluation at 4 weeks, 8 weeks, and 12 weeks, which involved ulcer assessment using the MEASURE methodology, photographing the ulcer, and assessment of adverse events. If the ulcer progressed to healing, the patient’s participation in the study was terminated.
Outcomes
The primary outcome of the study was VU area reduction by optimizing the healing process in patients who used 5% R. mangle cream for 12 weeks. In both groups, VU area was measured on D1 as well as at 4-, 8-, and 12-week follow-up visits. The secondary outcomes were VU characteristics in both groups according to the MEASURE methodology: measurement of ulcer area in centimeters squared, quantitative and qualitative evaluation of exudate, description of the appearance of the ulcer base as well as the type of tissue and coloration, pain intensity according to the numerical pain scale, type of pain, reassessment at 4-week intervals, and edge assessment of the VU and the perilesional skin.
Patients experiencing moderate to severe pain on D1 and during follow-up evaluations were referred to a vascular surgeon to assess the indication for analgesia with paracetamol and codeine, and for monitoring patients for local and systemic adverse events.
Sample size calculation
To calculate the sample size, the following were considered: the data on the mean and standard deviation (SD) of the variations (differences) between the assessment on D1 of the assessments at 4 weeks, 8 weeks, and 12 weeks relative to the areas of pilot sample ulcers in the EG and the CG. In the pilot sample, 15 samples from each group were considered and the largest sample size. Data from the largest sample corresponded to the variation from D1 to 12 weeks, with a reduction in the mean in the EG and an increase in the CG. The values of the mean (SD) of the variation (difference between D1 and 4 weeks) in the EG corresponded to a reduction of 6.84 (6.61), while in the CG it corresponded to an increase of −1.20 (12.26). The 20% margin of error was 5%, power of 90% for the 2-sided Mann-Whitney test with asymptotic relative efficiency (ARE) distribution, and the minimum sample size was 40 ulcers in each group. The research was carried out with 55 ulcers in the EG and 45 in the CG. Calculations were done using G*Power (version 3.1.9.2).
Statistical analysis
Data were expressed as absolute frequencies and percentages for categorical variables and measurements, whereas mean (SD), median, and 25th and 75th percentiles were used for numerical variables. To compare groups in relation to categorical variables, either the Pearson chi-square test or the Fisher exact test was used. When comparing groups in relation to numerical variables, the t test with equal variances or the Mann-Whitney test was used; when comparing assessments in the same group, the Friedman test was used. In the case of a significant difference, the Friedman test was used and multiple comparison tests were obtained (between pairs of assessments). The t test with equal variances was chosen when the normality of the data in each group and equality of variances between the 2 groups were verified, and the Mann-Whitney and Friedman tests were used in the absence of data normality. Normality was checked using the Shapiro-Wilk test, and equality of variances was assessed using the F test. The margin of error used in the statistical tests was 5%. The data were entered into the Excel spreadsheet, and statistical calculations were done using SPSS version 25 (IBM Corporation).
Results
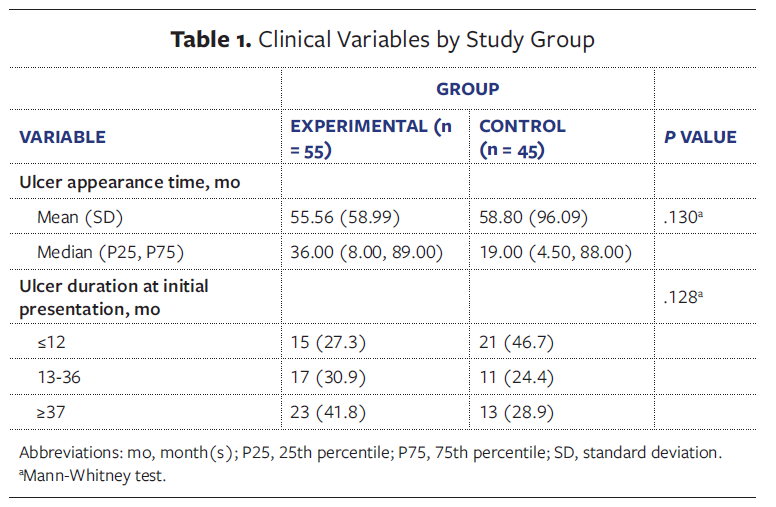
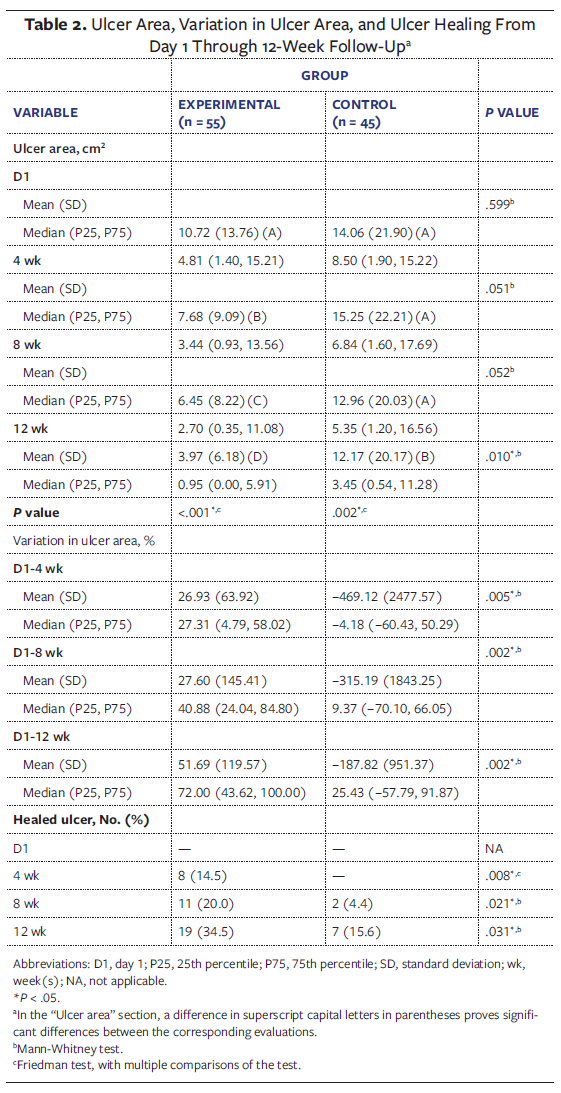
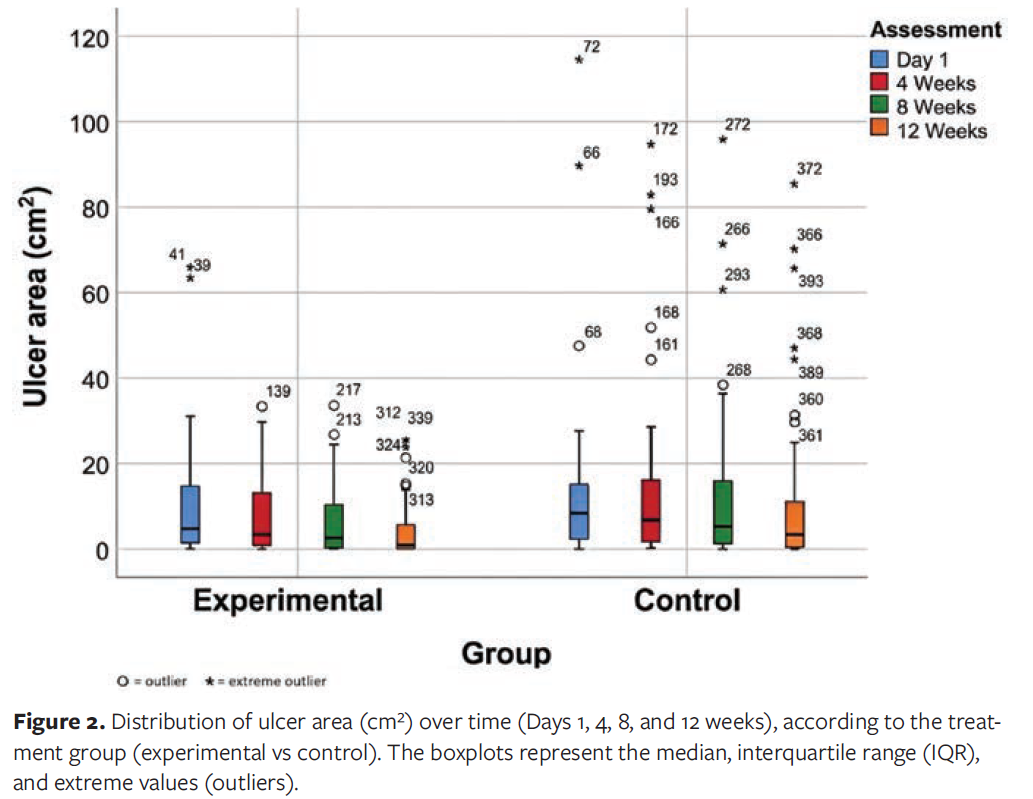
A total of 100 VUs were analyzed, with 55 ulcers in the EG and 45 ulcers in the CG (Table 1). At 12 weeks, the EG showed a mean 51.69% reduction in ulcer area, with a mean (SD) area of 3.97 (6.18) cm². In contrast, the CG exhibited lesion worsening, with an increase in ulcer area corresponding to a −187.82% variation, with a mean area of 12.17 (20.17) cm². Complete healing was observed in 34.5% of ulcers in the EG compared with 15.6% in the CG (P = .031). Furthermore, the EG demonstrated greater improvement than the CG across all clinical ulcer parameters (Table 2; Figure 2). Figure 3 shows a VU that progressed to complete healing in less than 12 weeks in a patient in the EG.
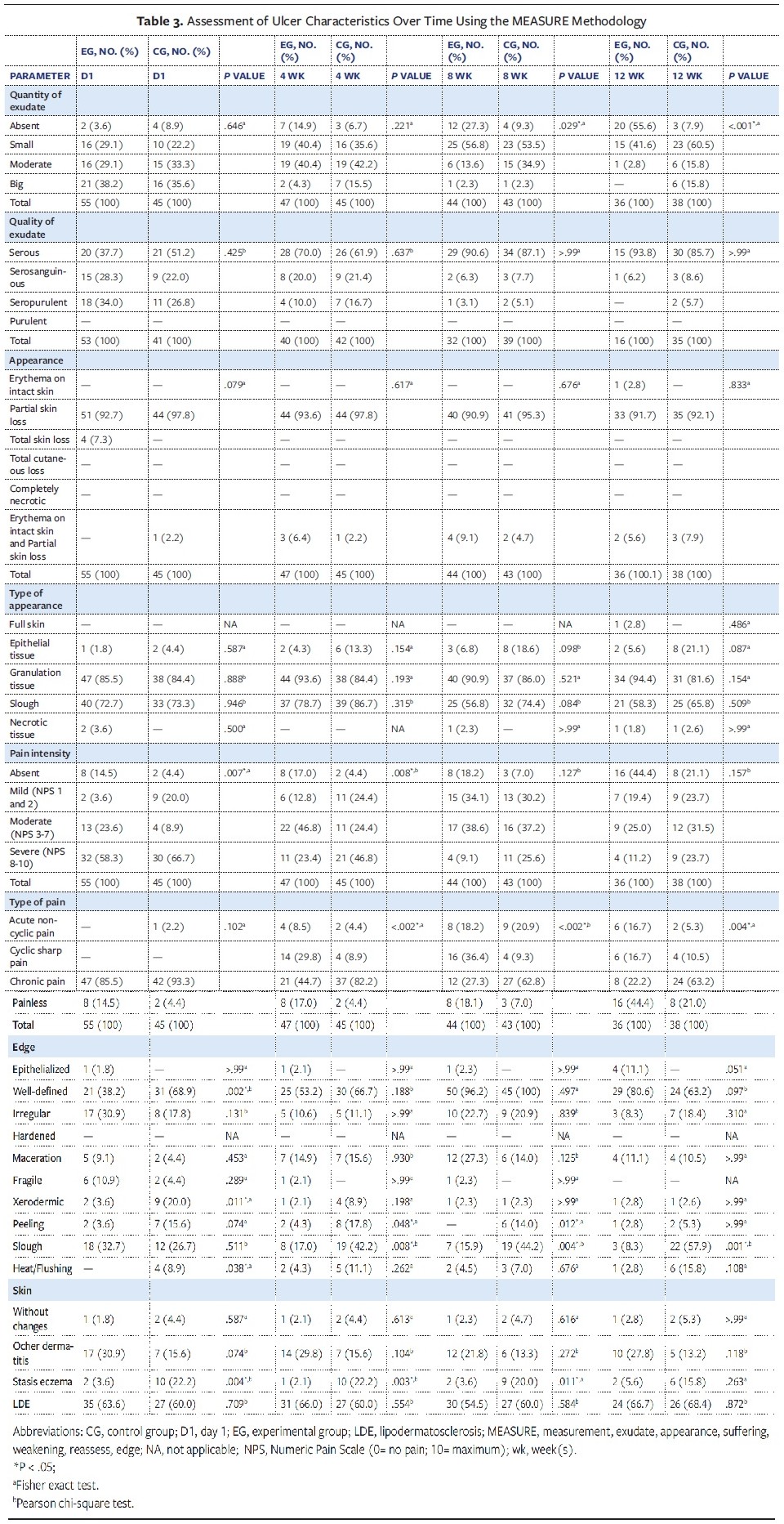
Using the MEASURE methodology, the researchers found that exudate was nearly absent in 55.6% of the ulcers in the EG vs 7.9% of the ulcers in the CG at 12-week follow-up (P < .001). The quality of the exudate progressively improved; at 12-week follow-up, only 1 ulcer in the EG had serosanguinous exudate, whereas 5 ulcers in the CG had seropurulent or serosanguinous exudate (Table 3).
Neither therapy worsened the appearance of the ulcer base, which consistently showed partial skin loss with areas of intact skin and erythema across sequential assessments at weeks 4, 8, and 12. However, there was a greater percentage reduction in the presence of slough in the EG than in the CG, with slough present in 72.7% of ulcers in the EG compared with 73.3% in the CG on D1 vs in 58.3% of ulcers in the EG and 65.8% of active ulcers in the CG at 12-week follow-up (Table 3). Furthermore, presence of granulation tissue increased in the EG, from 85.5% on D1 to 94.4% at 12-week follow-up. In comparison, presence of granulation tissue decreased from 84.4% to 81.6% at the same time points in the CG.

Moderate to severe pain intensity was present in 81.8% of ulcers in the EG and in 75.6% of ulcers in the CG on D1. At 4 weeks, 17% of ulcers in the EG were painless, compared with 4.4% in the CG (P < .008). At the end of 12 weeks, 44.4% of ulcers in the EG were painless, compared with 21.1% in the CG. The type of pain also changed over time. On D1, chronic pain was present in a high percentage of ulcers in both groups (EG, 85.5%; CG, 93.3%). After 4 weeks, chronic pain was considerably reduced in the EG (44.7%) compared with the CG (82.2%) (P < .002). At 8 weeks, chronic pain was present in only 27.3% of active ulcers in the EG and in 62.8% in the CG (P < .002). Of the active ulcers at 12 weeks, chronic pain was present in 22.2% in the EG and 63.2% in the CG (P = .004) (Table 3).
There were no ulcers with detachment of the perilesional skin in either group. On D1, the edges of the venous ulcers were better defined in the CG (68.9%) compared with the EG (38.2%), with P = .002. However, at the end of 12 weeks, the CG had 57.9% of the edges with slough, while the EG had only 8.3%, with P = .001. In addition, cutaneous changes of chronic venous disease (CVD) were identified, with patients presenting lipodermatosclerosis in 63.3% of the EG and 60% of the CG on D1. (Table 3).
Discussion
In the present study, women represented 67.1% of the sample, in agreement with a population study that reported 66% female participants.21 The prevalence of systemic arterial hypertension was 59% in the EG and 67.7% in the CG, with P = .451, values higher than those observed in the general population.22 Obesity was also present in both groups, with an average body mass index of 32 kg/m², identified in 64.1% of patients in the EG and in 61.3% in the CG. Venous pressure in the feet is significantly higher in obese individuals in all positions, and lower limb ulcer disease is more severe than in non-obese individuals.1,23
VU is a complex system of the inexorable pathophysiological evolution of primary CVD that is not correctly treated,3 which explains a long period of venous insufficiency and local inflammatory processes before culminating in the wound.24 In a population-based multicenter study conducted by researchers from France and Germany, only 36% of patients had CVD lasting 5 years or longer. Patients were from Brazil, the Czech Republic, France, Hungary, Italy, Romania, Russia, and Spain, but recruitment for this study was not known to the researchers and the research participants answered an online questionnaire, thus preventing the researchers from confirming the presence or absence of CVD. The justification was that, typically, patients with early-stage CVD seek medical care sporadically.21 In the present study, the average duration of CVD was greater than 18 years in both groups, probably because the sample was drawn from an outpatient clinic specializing in angiology and vascular surgery at a tertiary public hospital that performs surgical interventions and is a referral center for severe cases.
Although the patients in the present study had long-term disease, the majority did not use oral symptomatic drugs for CVD, such as venoprotectors (diosmin plus hesperidin) or hemorheological drugs (pentoxifylline), which is similar to other studies reporting low use of these medications.25 In the case of venoprotectors, lack of use is likely because they are not provided by Brazil’s public health system, although adjuvant treatment with micronized purified flavonoid fraction can reduce inflammation associated with venous hypertension, promote VU healing, and improve quality of life if associated with compression therapy.1 Pentoxifylline likely was not used by most patients in the present study because there are conflicting studies about its real benefit,26 despite it being recommended by scientific societies.1,3
The primary outcome of the current study was evaluation of the use of 5% R. mangle cream on VUs. There was a significant reduction in mean ulcer area in the EG from D1 to 12 weeks (P = .010), and complete healing was achieved in 34.5% of ulcers in that group, whereas in the CG, the mean ulcer area reduction and complete healing were smaller (P = .031).
R. mangle extract has a mitogenic effect and a phytochemical profile that includes tannins and flavonoids.11 These secondary compounds, especially tannin and tannic acid, have epithelializing, angiogenic, antioxidant actions and stimulate extracellular matrix production, with no evidence of local or systemic toxicities in several preclinical studies.9,10,11,13-15
In 2024, an in vivo study was published in which surgical wounds were created on the backs of rats. Histomorphometric analysis of the scars after 15 days of daily application of 5% R. mangle cream showed complete wound re-epithelialization (determined by measuring the distance between the epithelia), with statistically significant differences observed between the groups. Those treated with 5% dexpanthenol cream (positive control group) and 0.9% saline solution (negative control group) did not show comparable results, suggesting that R. mangle extract may effectively contribute to wound re-epithelialization.27
A preliminary, randomized, controlled, blinded clinical trial evaluated the action of a 5% R. mangle cream compared to a 5% dexpanthenol cream on 3-mm circular surgical wounds in the upper eyelids of volunteer patients. Clinical analysis demonstrated macroscopic, morphometric, and histomorphometric healing after 7 days of use of both medications. Histomorphometric analysis showed a significantly smaller distance between the epithelia in the R. mangle group compared to the dexpanthenol group (P < .05); no adverse events were reported.12
That study also evaluated cutaneous hydration in skin treated with 5% R. mangle cream and 5% dexpanthenol cream. Skin hydration achieved by the 5% R. mangle cream likely occurs because of the presence of secondary compounds, which cause antioxidant and free radical scavenging effects.12 Moreover, earlier studies have reported that R. mangle components form a superficial protective film through interaction with skin proteins, resulting in wound isolation and the creation of a humid microenvironment favorable to tissue repair.16 Optimal hydration of both the ulcer and perilesional tissue is essential for effective healing; moisture-retentive environments have consistently been associated with enhanced tissue regeneration and reduced incidence of infection, scarring, and pain.28-30
The MEASURE methodology was used to compare several parameters within and between groups in the current study.20 At the end of 12 weeks, there was significantly less exudate in the EG compared with the CG. This outcome also reduced costs by decreasing the need for changes of the secondary dressing (ie, the outer absorbent dressing applied over the primary wound dressing to manage exudate). Regarding exudate quality, both groups showed improvement after 12 weeks, with most wounds exhibiting serous exudate. Excessive wound exudate may prolong the inflammatory phase of healing due to the presence of proinflammatory cytokines and proteases, thereby favoring the chronification of venous ulcers.
In terms of ulcer appearance, there was a reduction in the presence of slough at the base of the ulcer in both groups. It was not uncommon to find more than one type of tissue, such as granulation tissue and slough; therefore, in the analysis of the type of appearance, several types of tissues were noted. It is important to emphasize that the preparation of the ulcer base promotes the conversion of the molecular and cellular environment of a chronic wound to that of an acute healing wound with the possibility of resolution.31 Although there are no studies on the autolytic properties of R. mangle cream, the improvement of the ulcer base should not be ignored, and further studies should address this gap.
The intensity of pain in venous ulcers was arbitrarily defined in this study as absent, mild, moderate, or severe. Pain can originate from nociceptive or neuropathic mechanisms, and its occurrence can be classified as noncyclic (sporadic), cyclic (frequent, for example, during dressing changes, at the end of the day), or chronic.32 Four main causes of pain were identified: the wound itself; underlying pathophysiological processes and disease-related complications (eg, neuropathy, inflammation, ischemia, infection); procedures associated with treatment, including debridement, dressing changes, and wound cleansing; and, in some cases, a very low individual pain threshold.33
Pain is an important symptom in patients with VU, affecting quality of life.34 In the present study, pain intensity was assessed using a numerical scale. On D1, pain was moderate to severe in 81.8% of ulcers in the EG and 75.6% in the CG, which is consistent with a systematic review published in 2020 that reported an 80% prevalence of moderate to severe pain in patients with VU.33 At 12-week follow-up in the current study, the percentage of pain-free ulcers had improved to 44.4% in the EG and 21.1% in the CG. The number of pain-free ulcers increased between week 8 and week 12 in the EG and between week 4 and week 12 in the CG. A study involving the treatment of VU with bacterial cellulose membrane showed a significant reduction in pain and discontinuation of analgesic use with this treatment compared to controls; however, the type of pain was not evaluated.6
In addition to assessing and monitoring pain intensity, it is also important to assess and monitor the type of pain—chronic, acute cyclical, or acute noncyclic—because therapeutic plans can be optimized, and tracking such pain can aid in monitoring the evolution of VU treatment.32 For example, in the current study, the percentage of ulcers with chronic pain in the EG decreased from 85.5% on D1 to 22.2% at 12-week follow-up (P = .004). The results of the current study indicate that reduction of frequency and duration of pain should be included in patient assessment and monitoring.
The MEASURE methodology was created to evaluate wounds in general, such as pressure ulcers and arterial ulcers; commonly, venous ulcers do not present areas of perilesional skin detachment, which are correlated with the severity of tissue necrosis, as in pressure ulcers. In the current study, no ulcer in its initial evaluation in any of the groups presented perilesional skin detachment.35 The developmental or healing stage of the ulcer may be indicated by the morphological characteristics of the wound margins and the condition of the periwound skin.20 The final step of the MEASURE methodology is the assessment of the edges,20 and the CG group presented at the end of the study a high percentage of well-defined edges and little presence of slough, unlike the EG group, which, conversely, presented numerous sloughs at the edges. Both groups also presented, as early as D1, severe perilesional skin alterations, such as lipodermatosclerosis.
In the current study, only 1 patient reported an adverse event related to the use of R. mangle cream. The event was classified as mild, consisting of slight itching immediately after application of the cream; the cream was removed with abundant saline solution washing. The multidisciplinary team advised the patient not to continue treatment. In her medical history, the patient also reported intolerance to the use of medium-chain triglyceride oil and several healing creams. There was no need for specific therapy for the pruritus, other than discontinuation of the cream. In the study by Silva et al,12 although the R. mangle cream was applied to the upper eyelids, the thinnest skin on the body, no patient reported a cutaneous or ophthalmological adverse event.
Limitations
This study has some limitations. One is that follow-up was restricted to 12 weeks among patients with active ulcers. Since CVD is a chronic condition associated with morbidity rather than mortality, the hospital's multidisciplinary team routinely reassesses patients with chronic wounds every 90 days. Therefore, 90 days was defined as the study endpoint. After 90 days, patients in the CG who still had active venous ulcers in their lower limbs received the experimental treatment and continued follow-up under routine medical care. Another limitation was ulcer recurrence, which was not monitored over a 12-month period. In long-term studies, a crossover design can help control for intrinsic patient-related factors that may influence the healing process. Even so, baseline ulcer characteristics were homogeneous between groups at D1, thus minimizing potential confounding effects on the study results. Furthermore, future studies should consider including the use of venoprotective or hemorheological medications as part of the eligibility criteria to further reduce bias. In the current study, most patients were not using these medications, and those who were maintained stable treatment regimens throughout the study period.
The non-use of inelastic compression bandages represents a significant contextual limitation of this study. The research was conducted in a public hospital serving a predominantly low-income population, and access to inelastic compression systems was not routine. Consequently, compression therapy was limited to the use of elastic compression stockings, reflecting standard practice in this health care setting. Despite this limitation, treatment allocation and follow-up were standardized across groups to minimize potential biases. Future studies should consider strategies to mitigate this limitation, including providing inelastic compression bandages through research funding, partnerships with public health agencies or manufacturers, and the development of protocols that ensure equitable access to compression modalities. These approaches can improve treatment comparability while maintaining the applicability of results in real-world settings.
Conclusion
This clinical trial showed promising results with the use of R. mangle cream on VUs of the lower limbs, demonstrating the effectiveness of the cream with a VU mean area reduction of 51.69% as well as a 34.5% rate of healing after 12 weeks of treatment. In addition, treatment with this cream promoted exudate reduction, increased granulation tissue at the base of the ulcer, reduced intensity and type of pain, and improved tissue edges, suggesting its utility as an alternative therapy for VU.
Author and Public Information
Authors: Jéssica Guido de Araújo Sá, MD, MSc1; Jeymesson Raphael Cardoso Vieira, PhD2; Jerrar Janedson Xavier Silva, MD, PhD1; Natalia Araújo Lopes, MS1; Guilherme Rêis de Carvalho Pinheiro, MS1; Vinícius Salcedo Crusco, MS1; Camila Brito Segatti, MS1; Luiz Eugênio Peres de Freitas Filho, MS1; Pedro Henrique Vanderley da Silva Carneiro, MS1; Eduarda Santos de Santana, MSc3; and Esdras Marques Lins, MD, PhD1
Affiliations: 1Medical Science Center, Federal University of Pernambuco, Recife, Brazil; 2Department of Histology and Embryology, Biosciences Center, Federal University of Pernambuco, Recife, Brazil; 3Biosciences Center, Federal University of Pernambuco, Recife, Brazil
Author Contributions: Study conception and planning, data collection and analysis, result interpretation, manuscript drafting, critical review and editing, and ethical responsibility: J.G.A.S. and E.M.L. Contribution to study conception and planning, as well as critical review and editing of the manuscript: J.R.C.V. Assisted in interpreting the study results: J.J.X.S. Participated in data collection and analysis: N.A.L., G.R.C.P., V.S.C., C.B.S., L.E.P.F.F., and P.H.V.S.C. Participated in review and editing of the manuscript: E.S.S.
Acknowledgments: The authors would like to thank all the researchers and experts who participated in this study.
Disclosure: The authors have no financial or other conflicts of interest to disclose.
Ethical Approval: The methods used in this study were approved by the Research Ethics Committee of Federal University of Pernambuco (process number 5.535.377) and are registered in the Brazilian Registry of Clinical Trials (process number RBR-106nvs7h), and they follow international ethical guidelines (Declaration of Helsinki, Council for International Organizations of Medical Sciences [CIOMS] International Guidelines for Biomedical Research Involving Human Subjects) and Brazilian ethical guidelines (Res. CNS 466/12 and complementary). Written informed consent was obtained from all subjects involved in the study.
Correspondence: Jeymesson Raphael Cardoso Vieira; Department of Histology and Embryology, Biosciences Center, Federal University of Pernambuco, Av. Prof. Moraes Rego, 1235, Cidade Universitária, 50760-420, Recife, PE, Brazil. E-mail: jeymesson.vieira@ufpe.br
Manuscript Accepted: February 20, 2026.
References
- Kikuchi R, Nhuch C, Drummond DAB, et al. Brazilian guidelines on chronic venous disease of the Brazilian Society of Angiology and Vascular Surgery. J Vasc Bras. 2023;22:e20230064. doi:10.1590/1677-5449.202300642
- Kitchens BP, Snyder RJ, Cuffy CA. A literature review of pharmacological agents to improve venous leg ulcer healing. Wounds. 2020 Jul;32(7):195-207. PMID: 33166265.
- Abbade LPF, Frade MAC, Pegas JRP, et al. Consensus on the diagnosis and management of chronic leg ulcers—Brazilian Society of Dermatology. An Bras Dermatol. 2020;95(suppl 1):1-18. doi:10.1016/j.abd.2020.06.002
- Shaydakov ME, Ting W, Sadek M, et al; American Venous Forum Research Committee. Review of the current evidence for topical treatment for venous leg ulcers. J Vasc Surg Venous Lymphat Disord. 2022;10(1):241-247.e15. doi:10.1016/j.jvsv.2021.06.010
- Cavalcanti LM, Pinto FCM, de Oliveira GM, Lima SVC, Aguiar JLA, Lins EM. Efficacy of bacterial cellulose membrane for the treatment of lower limbs chronic varicose ulcers: a randomized and controlled trial. Rev Col Bras Cir. 2017;44(1):72-80. doi:10.1590/0100-69912017001011
- Silva LG, Albuquerque AV, Pinto FCM, Ferraz-Carvalho RS, Aguiar JLA, Lins EM. Bacterial cellulose: an effective material in the treatment of chronic venous ulcers of the lower limbs. J Mater Sci Mater Med. 2021;32(7):79. doi: 10.1007/s10856-021-06539-1
- Eriksson E, Liu PY, Schultz GS, et al. Chronic wounds: treatment consensus. Wound Repair Regen. 2022;30(2):156-171. doi:10.1111/wrr.12994
- Regalado AI, Sánchez LM, Mancebo B. Rhizophora mangle L. (mangle rojo): una especie con potencialidades de uso terapéutico. J Pharm Pharmacogn Res. 2016;4(1):1-17.doi: 10.56499/jppres15.095_4.1.1
- Sánchez Janet, Faure R, Martínez G, Vega E, Fernández O. Propiedades antioxidantes de Rhizophora mangle (L.) y su relación con el proceso de curación de heridas en ratas. Rev Salud Anim. [Internet]. 2009 Dic [citado 2026 Mar 25] ; 31( 3 ): 170-175. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0253-570X2009000300006&lng=es.
- Araújo JG. Wound healing through topical treatment with Rhizophora mangle L leaf extract cream [dissertation]. Recife: Universidade Federal de Pernambuco; 2015. Disponível em: https://repositorio.ufpe.br/handle/123456789/18404
- De-Faria FM, Almeida ACA, Luiz-Ferreira A, et al. Mechanisms of action underlying the gastric antiulcer activity of the Rhizophora mangle L. J Ethnopharmacol. 2012;139(1):234-243. doi:10.1016/j.jep.2011.11.007
- Silva JJX, Leal LB, Sá JGA, et al. A preliminary study of cutaneous wound healing on the upper eyelid in a small Brazilian population using Rhizophora mangle-based cream. An Acad Bras Ciênc. 2024;96(1):e20231143. doi:10.1590/0001-3765202420231143
- Marrero E, Sánchez J, de Armas E, et al. COX-2 and sPLA2 inhibitory activity of aqueous extract and polyphenols of Rhizophora mangle (red mangrove). Fitoterapia. 2006;77(4):313-315. doi:10.1016/j.fitote.2006.03.009
- Wendel GH, Teves MR, Paredes JD, Sánchez Perera LM, Pelzer LE. Evaluation of the antidiarrheal activity of Rhizophora mangle L. (Rhizophoraceae). Lat Am J Pharm. 2013;32(1):128-131.
- Sánchez J, Melchor G, Martínez G, Escobar A, Faure R. Antioxidant activity of Rhizophora mangle bark. Fitoterapia. 2006;77(2):141-143. doi:10.1016/j.fitote.2005.11.011
- Fernandez O, Capdevila JZ, Dalla G, Melchor G. Efficacy of Rhizophora mangle aqueous bark extract in the healing of open surgical wounds. Fitoterapia. 2002;73(7-8):564-568. doi:10.1016/s0367-326x(02)00229-0
- da Silva LA, Lira EC, Leal LB, et al. Prevention of necrosis in ischemic skin flaps using hydrogel of Rhizophora mangle. Injury. 2022;53(7):2462-2469. doi:10.1016/j.injury.2022.03.034
- Sánchez Perera LM, Fraga Chávez I, Macebo Dorveny B, Lorenzo Miranda R. Toxicidad aguda y subaguda oral del extracto acuoso liofilizado de Rhizophora mangle L. en ratas. Rev Cubana Plant Med [Internet]. 2008;13(3). Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1028-47962008000300008&lng=es.
- de Oliveira AB, Ferrisse TM, de Annunzio SR, et al. In vitro evaluation of photodynamic activity of plant extracts from Senna species against microorganisms of medical and dental interest. Pharmaceutics. 2023;15(1):181. doi:10.3390/pharmaceutics15010181
- Keast DH, Bowering CK, Evans AW, Mackean GL, Burrows C, D’Souza L. MEASURE: a proposed assessment framework for developing best practice recommendations for wound assessment. Wound Repair Regen. 2004;12(3 Suppl):S1-S17. doi:10.1111/j.1067-1927.2004.0123S1.x
- Rabe E, Régnier C, Goron F, Salmat G, Pannier F. The prevalence, disease characteristics and treatment of chronic venous disease: an international web-based survey. J Comp Eff Res. 2020;9(17):1205-1218. doi:10.2217/cer-2020-0158
- Migowski, Arn & Costa, Gustavo. (2024). Análise temporal da prevalência de hipertensão arterial no Brasil entre 2006 e 2023: evidências a partir dos dados do Vigitel. OnScience. 2. e0027. doi: 10.33634/2764-0736.2024.0027
- Mościcka P, Cwajda-Białasik J, Jawień A, Jaraczewski W, Szewczyk MT. Evaluation of factors affecting the healing process of venous ulcers: A 12-week longitudinal study. Wound Repair Regen. 2023 Nov-Dec;31(6):783-792. doi: 10.1111/wrr.13140
- Nicolaides AN. The most severe stage of chronic venous disease: an update on the management of patients with venous leg ulcers. Adv Ther. 2020;37(Suppl 1):19-24. doi:10.1007/s12325-020-01219-y
- Sant'ana SM, Bachion MM, Santos QR, Nunes CA, Malaquias SG, Oliveira BG. Venous ulcers: clinical characterization and treatment in users treated in outpatient facilities. Rev Bras Enferm. 2012 Jul-Aug;65(4):637-44. Portuguese. doi: 10.1590/s0034-71672012000400013. PMID: 23258684.
- Lemos PC, Lins EM, Pinto FCM, Aguiar JLA, Appolonio F, Breno F. Evaluation of pentoxifylline and ferrous sulfate for treatment of lower limb venous ulcers. J Vasc Bras. 2021;20:e2020167. doi:10.1590/1677-5449.200167
- Sá JGA, de Souza IA, Marcelino Neto PP, de Santana ES, Vieira JRC. Evaluation of wound healing activity of Rhizophora mangle in cream. Acta Sci Biol Sci. 2024;46:e67572. doi:10.4025/actascibiolsci.v46i1.69794
- Sánchez-Nicolat NE, Guardado-Bermúdez F, Arriaga-Caballero E, et al. Revisión en úlceras venosas: epidemiología, fisiopatología, diagnóstico y tratamiento actual. Revista Mexicana de Angiología. 2019;47(1):26-38. doi: 10.24875/RMA.21000005
- Nuutila K, Eriksson E. Moist wound healing with commonly available dressings. Adv Wound Care (New Rochelle). 2021;10(12):685-698. doi:10.1089/wound.2020.1232
- Lee TY, Yoon IJ, Han SK, Namgoong S, Jeong SH, Kim DW, Dhong ES. Skin hydration level cutoff value to predict wound healing potential in diabetic foot ulcers. Diabetes Res Clin Pract. 2022 Nov;193:110122. doi: 10.1016/j.diabres.2022.110122. Epub 2022 Oct 19. PMID: 36272583.
- O'Donnell TF Jr, Passman MA, Marston WA, et al. Management of venous leg ulcers: clinical practice guidelines of the Society for Vascular Surgery ® and the American Venous Forum. J Vasc Surg. 2014 Aug;60(2 Suppl):3S-59S. doi: 10.1016/j.jvs.2014.04.049. Epub 2014 Jun 25. PMID: 24974070.
- World Health Organization. WHO guidelines for the pharmacological and radiotherapeutic management of cancer pain in adults and adolescents. Geneva, Switzerland: World Health Organization; 2018.
- Leren L, Johansen E, Eide H, Falk RS, Juvet LK, Ljoså TM. Pain in persons with chronic venous leg ulcers: a systematic review and meta-analysis. Int Wound J. 2020;17(2):466-484. doi:10.1111/iwj.13296
- Raffetto JD, Ligi D, Maniscalco R, Khalil RA, Mannello F. Why venous leg ulcers have difficulty healing: overview on pathophysiology, clinical consequences, and treatment. J Clin Med. 2020 Dec 24;10(1):29. doi: 10.3390/jcm10010029. PMID: 33374372; PMCID: PMC7795034.
- Arora M, Harvey LA, Chhabra HS, Sharawat R, Glinsky JV, Cameron ID. The reliability of measuring wound undermining in people with spinal cord injury. Spinal Cord. 2017 Mar;55(3):304-306. doi: 10.1038/sc.2016.108. Epub 2016 Jul 12. PMID: 27401125.






