Proposed Addendum to the 2006 US Food and Drug Administration Guidance on Chronic Cutaneous Ulcers and Burn Wounds: Recommendations from the Wound Care Collaborative Community
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
The Wound Care Collaborative Community (WCCC) presents this proposed addendum to the 2006 US Food and Drug Administration (FDA) guidance for industry on chronic cutaneous ulcers and burn wounds, with this addendum reflecting nearly 2 decades of scientific and clinical progress. Key gaps in the original guidance have emerged with advances such as the Wound Reporting in Animal and Human Preclinical Studies (WRAHPS) reporting standards and the FDA Biomarker Qualification Program. This proposed addendum updates preclinical recommendations by emphasizing standardized bioassays for biologics, improved animal model selection using WRAHPS criteria, and acknowledgment that animal studies primarily assess safety rather than predict clinical efficacy. Clinical study design recommendations incorporate digital wound assessment technologies; standardized photographic documentation; expanded biomarker use; and innovative umbrella, basket, and platform trial designs to better address biological heterogeneity in chronic wounds. While reaffirming complete wound closure as the most clinically meaningful end point, the addendum also supports the development of validated alternative end points, including patient-reported outcomes. Additional updates include biofilm detection strategies, point of care diagnostic tools, and recognition of differences between clinical trial populations and real world patients. These evidence based recommendations aim to accelerate development of safe and effective wound care products while ensuring alignment with modern regulatory standards.
Chronic wounds, including venous insufficiency ulcers, diabetic foot ulcers (DFUs), pressure ulcers, and burn wounds, continue to pose significant challenges for both patients and health care systems.1 Despite a major clinical need, very few treatments have received US Food and Drug Administration (FDA) approval for efficacy in treating these wounds.2,3 In 2006, the FDA, through the Center for Drug Evaluation and Research (CDER), the Center for Biologics Evaluation and Research, and the Center for Devices and Radiological Health, published a guidance document concerning the development of products for the treatment of chronic cutaneous ulcers and burn wounds.4
The original 2006 FDA guidance document articulates key recommendations for sponsors regarding the preclinical and clinical development of drugs, biological products, and medical devices used in wound management. It is noteworthy that the FDA guidance is not intended to establish legally enforceable obligations; rather, it reflects the FDA’s current thinking on this subject, and it states that sponsors “can use an alternative approach if the approach satisfies the requirements of the applicable statutes and regulations” (eg, per Title 21 of the Code of Federal Regulations).4 As with any guidance document, its contents should be interpreted as recommendations.
Chronic cutaneous ulcers are complex and arise from varied etiologies, including venous insufficiency, diabetes, and other systemic factors, and these ulcers frequently progress to hard to heal wounds due to impaired or incomplete healing.2,3 Although each wound type exhibits distinct pathophysiological features that may necessitate separate clinical evaluation,5 clinical experience demonstrates substantial overlap in the demographics and comorbidities of affected patients, as well as shared biological mechanisms of healing. These similarities support the recommendation of the authors of the proposed addendum that the FDA consider broader acceptance of clinical data across wound types, particularly when multiple indications have already been studied. Consistent with this perspective, the 2006 FDA guidance for industry emphasizes that product labeling must clearly define the wound types a product is intended to treat and must be supported by substantial clinical evidence demonstrating safety and effectiveness for those indications.4
A clear and specific indication for use significantly facilitates the development and subsequent approval of wound care products.4 Sponsors are encouraged to provide compelling evidence reflecting the safety and efficacy of their products for particular wound types. However, in situations in which robust scientific rationale and clinical data suggest potential efficacy across various wound types, shared clinical trial data may be useful in supporting efficacy claims, provided that strong justification is presented to mitigate the risks associated with generalizing results.4
This proposed addendum by the Wound Care Collaborative Community (WCCC) adheres to these guiding principles and endeavors to serve as a recommended update to the 2006 FDA guidance document, incorporating contemporary clinical evidence and insights derived from the literature and contributions from the wound care community. The objective of this project is to enhance and streamline the development of wound care products throughout the continuum of care. The authors assert that improved understanding and adherence to current guidelines will significantly enhance the safety and efficacy of products intended for patients with hard-to-heal wounds.
Work Group Composition and Development Process
This proposed addendum was developed through a consensus process led by the WCCC FDA Guidance Document Work Group. The working group comprises clinicians, scientists, industry professionals, and regulatory experienced contributors who collectively represent several decades of experience across the wound care research and product development continuum.
In addition, the author panel includes individuals with primary backgrounds in clinical wound care, preclinical and translational science, regulatory affairs, medical device and biologics development, clinical trial design, and health technology innovation. Clinical contributors include board-certified physicians, podiatrists, nurses, and physical therapists with extensive experience in the management of chronic wounds across outpatient, inpatient, and specialty care settings. These authors contribute real-world clinical insight into patient populations, treatment pathways, and practical challenges in wound healing research and care delivery.
Preclinical and translational expertise within the group is contributed by scientists with doctoral-level training in wound biology, tissue repair, bioassay development, animal modeling, and biomarker discovery. These contributors have led and participated in laboratory-based studies evaluating mechanisms of action, safety, and biological activity of wound care therapies, as well as the development of standardized reporting frameworks for preclinical wound research.
Industry representation includes senior leaders and subject matter experts from medical device, biologics, diagnostics, and wound imaging organizations; these experts have direct experience in product development, regulatory submission strategy, clinical trial execution, and postmarket evidence generation. Several authors have served in executive, medical affairs, scientific, or product strategy roles, providing applied perspectives on regulatory feasibility, manufacturing considerations, and commercialization pathways.
Academic contributors represent major universities and research institutions, and they bring perspectives on methodology, evidence synthesis, clinical end points, and educational dissemination. In addition, the working group includes contributors with experience in health economics, business consulting, clinical operations, and legal/regulatory interpretation, further supporting the multidisciplinary nature of the recommendations.
The diversity of professional backgrounds spanning clinical, scientific, industry, nonprofit, and academic collaborative settings was intentional to ensure that the proposed updates to the 2006 FDA guidance reflect both scientific rigor and operational practicality. Draft recommendations were developed iteratively through literature review, expert discussion, and consensus refinement, with emphasis on areas in which advances in science, technology, and clinical practice have created gaps in the original guidance.
The recommendations presented represent expert consensus informed by collective experience and published evidence rather than formal regulatory policy and are intended to support ongoing dialogue among sponsors, investigators, and regulators engaged in wound care product development.
Suggested Updates to Preclinical Considerations
Bioassays
Preclinical testing is a critical component of product development, wherein comprehensive evaluations of safety and efficacy are essential. The FDA guidance document from 2006 did not address the topic of bioassays.4 Contemporary preclinical considerations highlight the imperative of implementing stringent bioassays to ensure both the potency and therapeutic consistency of wound treatment products. Potency assays are primarily applicable to biologics; in contrast, performance characteristics are used to determine appropriate regulatory designation of devices.6 Integration of bioassays into the preclinical testing framework is essential for validating product performance and securing regulatory approval.
To achieve consistent therapeutic outcomes for biologics license application and premarket approval products, it is critical to validate their activity and potency through comprehensive testing.7 Potency is defined as the specific capacity of a product to induce its intended biological effects, particularly in the context of wound healing.8 The following recommendations are proposed for the evaluation of activity and potency during the preclinical development of wound care products.
The selection of potency assays should align with the expected mechanism of action of the wound treatment product. Commonly used potency assays comprise cell-based assays that assess cellular responses, such as migration, proliferation, and differentiation (eg, fibroblast or keratinocyte proliferation).8 Additionally, biochemical assays can quantify specific biological molecules (eg, growth factors, cytokines), whereas functional assays may evaluate tissue regeneration and matrix deposition (eg, collagen synthesis, tensile strength).8
It is imperative to establish potency acceptance criteria, with justification for thresholds derived from preclinical efficacy studies. These thresholds should ensure that each batch of the product consistently demonstrates adequate biological activity to support wound treatment. Furthermore, in vitro activity and potency assays should be shown to correlate with in vivo efficacy data from preclinical wound models, thereby validating the relevance of these assays in predicting clinical outcomes.
WCCC-suggested updated
recommendations for bioassays
Development of bioassays. Sponsors are encouraged to create robust, reproducible bioassays to verify the potency and efficacy of wound treatment products. These assays should correlate with clinically relevant outcomes, including epithelialization, angiogenesis, and fibroblast proliferation.
Assay validation and control. Assays should be rigorously validated according to FDA guidelines to ensure accuracy, precision, linearity, and specificity. Additionally, appropriate positive and negative controls must be included to reinforce the reliability of the data.
Standardized reporting. In alignment with WRAHPS guidelines, 9 the adoption of a standardized format for reporting findings is recommended to facilitate better understanding and comparability of results across studies.
Animal wound models
Animal wound models are essential for establishing safety, understanding pharmacological responses, and exploring mechanisms of action, as well as for evaluating potential toxicities of wound treatment products. However, there is a significant need for standardized reporting in preclinical testing for wound healing, as emphasized by the WRAHPS guidelines.9 Thus, the WCCC suggests the following updates to this section of the FDA guidance document.
The selection of an appropriate animal wound model should be based on sound scientific principles, the proposed mechanism of action, and its relevance to the specific scientific questions being investigated. It is important to note that existing models do not accurately reflect human condition and are typically not true “chronic” wound models.9,10 Instead, they are more accurately described as acute skin wound models that, due to certain conditions imposed on them, result in delayed or impaired healing to a various degree. Choosing the appropriate model for preclinical testing requires careful consideration, because each model has unique strengths and limitations, as highlighted by Ojeh et al.9 To ensure relevance of the model, the chosen animal species must demonstrate a measurable biological response to the test product.
Assessment methods should be rigorous and reproducible, prioritizing tissue morphometric evaluations over gross wound imaging, which can often be misleading.11 While animal models can be valuable for establishing proof of concept for certain products and for identifying potential mechanisms of action, they may not always be reliable predictors of efficacy in clinical trials.4 Therefore, efforts should be made to establish correlations between animal testing and human samples.
Given the absence of an ideal animal model for chronic wounds or extensive burns, it may be necessary to use multiple animal models to evaluate the efficacy of wound treatment products.12 For instance, as noted in Sullivan et al,13 “fibroplasia and stroma formation can be assessed through subcutaneous injection of products in various animal models, while contraction and re-epithelialization may be evaluated via topical application on full-thickness excisional wounds or in pig graft donor site models. Pigs are particularly useful as models because their skin architecture closely resembles that of human skin.” Additionally, angiogenesis induction can be assessed using the chick chorioallantoic membrane or rabbit cornea, and breaking strength assessments can be conducted in a rat linear incision model.14
Impaired healing models often extend the duration of assessment to accommodate various conditions, including infection or biofilm formation, necrotizing trauma, irradiation, corticosteroid or chemotherapeutic drug administration, and drug- or genetically induced diabetes in species such as mice, rats, hamsters, guinea pigs, and young pigs. It is essential to consider the duration of these induced biological changes prior to conducting any tests that seek to replicate aspects of human conditions. For example, wound evaluations performed immediately following the induction of either chemically or food-induced diabetes may yield misleading results.15
Furthermore, each model possesses specific characteristics that can facilitate the evaluation of a product’s efficacy. For instance, the rabbit ear dermal ulcer model is particularly advantageous for assessing re-epithelialization, as it does not exhibit the vigorous wound contraction observed in other rodent models and allows for the induction of ischemia within the wound.4,16 Additionally, combining biological changes, such as infection with diabetes and/or oxidative stress, may offer a more accurate representation of the human condition.17 The WRAHPS guidelines provide a comprehensive summary of key preclinical wound models, detailing assessment methods, along with the respective advantages and disadvantages of each model, thereby guiding experimental design and methodology prior to product testing.9
Although the phases of wound healing across various species may exhibit similarities to those in humans, there are significant variations in the timeline, healing mechanisms, anatomical structures of the skin, and underlying tissues.18 Thus, it is crucial to consider physiological and anatomical relevance to humans when selecting a preclinical model.
The data generated from these models can vary substantially based on the selected species, time points, and additional biological factors, including sex, age, hair cycle, microbiome diversity, metabolic considerations, wound type, and the underlying cause of the induced wound. Furthermore, assessment methods should take into account location-specific responses, because biological assessments and responses may differ notably between the wound edge and the wound base due to significant alterations in cellular composition. Another key factor to consider is the timing of assessments after the wound occurs. Evaluating the wound at only a single time point may not capture the full progression of the healing process. Instead, multiple time points should be included to better reflect the underlying biological mechanisms involved. For example, if the goal is to study the inflammatory phase of healing, then assessments should be done at earlier time points. In contrast, if the focus is on later outcomes, such as scarring, then assessments at later stages are more appropriate.
Preclinical models are designed to “replicate the underlying pathophysiology of human chronic wound disorders in animal systems, thereby enabling the study of wound healing under specific conditions and the evaluation of treatments for complex wounds.”9 However, inherent limitations exist within these experimental models due to the differences between impaired wound responses in animals and chronic wounds in humans. As reported in Ojeh et al,9 “species-specific variations in wound healing mechanisms, tissue architecture, and immune responses” complicate the accurate replication of human chronic wounds in animal models. Consequently, no single animal model can comprehensively represent all aspects of human chronic wounds; rather, each model reflects distinct characteristics of chronic ulcers. Therefore, it is imperative to carefully select an appropriate wound model while ensuring comprehensive documentation of methodology and results to guarantee that the outcomes are translatable.9
The FDA endorses the principles of the “3Rs”: replace, reduce, and refine animal testing when feasible. The FDA encourages sponsors to engage with the agency if they wish to use a non-animal testing method that is suitable, adequate, validated, and practical.9 Through this process, the FDA evaluates whether a proposed alternative testing methodology could be assessed for equivalency to an animal testing method.
Of note, the FDA’s pharmacology and toxicology review teams are primarily concerned about the potential of wound healing products to harm human subjects in clinical trials. As a result, nonclinical wound healing studies are primarily reviewed by these teams to evaluate whether the drug product potentially impairs wound healing.19 Although sponsors and researchers might use nonclinical wound healing studies as proof-of-concept studies and/or for hypothesis generation, these studies are not designed to evaluate clinical efficacy, which is best determined in clinical trials. Therefore, from the FDA’s perspective the primary purpose of an animal wound healing study is to assure that the drug product does not impair wound healing and to support the safet use of the drug product in clinical trials.19 Wound healing is a complicated process, and the best assessment of a drug product’s wound healing efficacy is through the conduct of clinical trials in human subjects.19
Suggested Updates to Clinical Study Design Considerations
Effective clinical trial design is paramount for demonstrating a product’s efficacy and safety. A well-structured clinical trial serves as the foundation for gathering robust evidence, which is essential for regulatory approvals and informing clinical practice. Researchers must meticulously plan the trial methodology, including participant selection, randomization, and data collection techniques. This rigor ensures that results are reliable and can be confidently interpreted. Ultimately, a thorough approach enhances the credibility of findings and facilitates informed decision-making in the health care sector.
The design of clinical trials for wound indications requires careful consideration to address the unique challenges associated with wound healing and treatment efficacy. The current proposal presents targeted recommendations to enhance trial design, focusing on methodologies tailored for wound-related outcomes, underlining the importance of robust and scientifically sound approaches to improve the validity and reliability of results, and the WCCC suggests the consideration of the following items.
Clinical study design: new elements (not in 2006 FDA guidance)
The recommendations outlined in this section aim to strengthen the rigor and relevance of wound indication trials. The WCCC asserts that embracing these considerations can result in significant advances in wound healing research and enhanced therapeutic outcomes for individuals experiencing chronic wounds.
Study length. The duration of a study should reflect the expected timeline for primary and secondary wound healing end points, allowing sufficient observation for treatment effects while maintaining participant engagement and adherence to study protocols. When feasible, studies should also incorporate extended follow up periods to evaluate wound recurrence and the durability of healing outcomes over time, which are critical for assessing the long-term effectiveness of wound care interventions.
Run-in phase. The inclusion of a run-in phase may be beneficial to stabilize patient conditions before randomization. However, the necessity of this phase must be assessed based on specific trial objectives and population characteristics.
Number of subjects. Determining the appropriate sample size is vital for statistical power. Studies should balance the number of subjects against resource availability and logistical considerations while ensuring adequate representation of the target population.
Decenteralized clinical trials. The potential implementation of decentralized clinical trial methodologies may enhance participant recruitment and retention, especially in diverse geographic locations. Consideration should be given to technological requirements and participant accessibility.
Data analysis. An effective data analysis plan is crucial to correctly interpret trial outcomes. Analysis should account for all randomized participants and use appropriate statistical methods to handle missing data and ensure integrity.
Randomization and stratification. For trials involving a small number of subjects, stratification should be simplified to prevent imbalances between treatment groups. Reducing the number of stratification variables can enhance the effectiveness of randomization and ensure comparable groups.20
Comparator arms. Clarification regarding the necessity of vehicle control arms is crucial; it is particularly important to determine circumstances in which such an arm may be impractical. While the FDA commonly requires a vehicle control in drug and biologics trials, some vehicle controls may have beneficial activity for topical skin preparations. The European Medicines Agency (EMA) ICH E10 guideline adopts a more practical approach to control design, allowing for methods better suited to the study context when standard approaches may not be feasible.21
Centralized adjudication and objective wound assessment
Use of a panel of assessors with specialized training in wound healing is recommended to maintain objectivity during wound evaluations. An odd number of assessors will facilitate a majority decision regarding wound status at confirmation visits. This process should be informed by initial assessments and supplemented by photographic evidence.22 Photographic evidence review should follow the guidelines outlined in the “Photographic Documentation” section of this proposed addendum.
Wound assessment and quantification. To enhance reliability and accuracy of wound assessment, the WCCC recommends the use of established methods supported by the medical literature for photo documentation as well as advanced measurement techniques imperative for producing objective, measureable results.
Photographic documentation should be integral to assessment and should adhere to standardized acquisition protocols to ensure accurate and consistent measurement. Reliability should be established through the use of validated measurement tools, which include scale and color calibration techniques, to reinforce data integrity. To this end, photographic documentation should be used as a primary means of objectively capturing and conveying changes in wounds over time. It is essential that photographs accurately represent live observations to serve as reliable supporting evidence in wound assessment. Photo documentation should follow the guidelines set forth in the “Photographic documentation” section.
Photographic documentation. Medical photographic documentation is a means to objectively support wound assessment, tissue identification, diagnosis, and healing response.23-28 The trustworthiness of a photo to accurately represent wound characteristics, such as size and color, is based on the reliability of the photo capture system and the techniques used to capture the photo. External markers adjacent to the wound are commonly used for establishing scale from which the size of the wound can be calculated.24 Various digital methods exist to reinforce photo capture techniques, such as outlines or shadows from the previous photo or methods that address skew to further increase the reliability of the photo documentation.24
Color accuracy can be objectively measured and validated through calibration techniques using a color chart with a range of clinically relevant colors.23-33 In the medical literature cited in the current article, the same process may be referred to both as color correction and color calibration by different authors. Assuring color accuracy allows for a consistent analysis of the wound and periwound, ensuring that observed color changes can be accurately identified and reported via the wound photograph. The combination of optimizing the wound capture techniques and color calibration have been shown to improve color accuracy by 73% over the National Institute of Standards and Technology baseline.34
Inaccurate and unreliable medical photographs can occur because of technical variability of the camera hardware and software, improper and/or inconsistent photographer technique, and the prevalence and ease of photographic manipulation. The medical literature clearly indicates proven methods to resolve these challenges, as shown in the supplementary material.
Incorporation of photo documentation in data analysis. Standardizing photo documentation and procedures for the use of digital wound imaging medical devices that automatically calculate wound area measurements, percentage area reduction (PAR), and percentage volume reduction (PVR) with accurate and reliable methods will improve the validity of wound assessment and quantification.35-38
To ensure optimal consistency and accuracy, the WCCC advises that examiners provide a detailed description of the photographic evaluation techniques used in wound healing assessments. In addition to traditional photographic documentation, it is recommended to integrate advanced digital devices for the extraction of wound measurements.
Validated devices available to measure PAR and PVR offer greater accuracy compared with conventional wound tracing methods.29 The use of these modern digital tools can significantly enhance the precision of wound assessments and uphold the integrity of the data obtained from photographic evidence.29
Ulcer classification
The WCCC recommendation emphasizes the importance of expanding the information provided on various ulcer grading scales. It is crucial to incorporate widely recognized criteria for classifying ulcer stages to ensure a comprehensive understanding of wound management.
One such classification is the National Pressure Injury Advisory Panel (NPIAP) grading system, which is specifically designed for pressure ulcers/injuries. This classification categorizes injuries into stages based on the severity of skin and tissue damage, ranging from stage 1, which indicates nonblanchable erythema of intact skin, to stage 4, which is characterized by full-thickness tissue loss and exposure of bone, tendon, or muscle.39
Several classification systems are used to assess DFUs, each with distinct strengths and limitations. The Wagner classification, one of the earliest and most widely used systems, focuses primarily on ulcer depth and the presence of gangrene, but it does not account for infection or ischemia.40 The University of Texas system expands on the Wagner classification by incorporating both infection and ischemia into a matrix format, offering improved prognostic value.41 The SINBAD (site, ischemia, neuropathy, bacterial infection, and depth) system provides a simple, binary scoring approach based on 6 clinical features, facilitating global comparisons and ease of use.42 The PEDIS (perfusion, extent, depth, infection and sensation) classification, developed by the International Working Group on the Diabetic Foot (IWGDF), is more descriptive and is commonly used in research settings to standardize reporting.43
Including classification system grading will promote accurate assessment and intervention strategies in ulcer management and will assist with generalization of study results. Selection of a grading system should be guided by clinical context, research needs, and the desired balance between simplicity and comprehensiveness.
Biofilms
The 2006 FDA guidance document did not address biofilms.4 Most hard-to-heal wounds are characterized by the presence of biofilm, as opposed to planktonic microbes.44 Consequently, the clinical signs and symptoms indicative of infection, as well as traditional wound cultures, may offer limited utility.
The WCCC recommends the use of tissue biopsy, which is generally considered preferable to quantitative and qualitative swab specimen cultures. Additionally, autofluorescence imaging devices to assess bioburden exceeding 104 CFU/g have been proven to have clinical utility and support diagnostic accuracy.45
In certain instances, more specialized diagnostic methods, such as polymerase chain reaction or next-generation sequencing, may be used to identify specific pathogens and assess antibiotic susceptibility or resistance to treatment. Next-generation sequencing has proved to be particularly valuable in complex clinical scenarios in which conventional techniques do not accurately identify the infection. This advanced sequencing approach characterizes microbial DNA present in the wound, facilitating the detection of bacterial, viral, and fungal pathogens and yielding comprehensive genomic insights, especially given the polymicrobial complexity of chronic wounds.46
Biomarkers
Biomarkers, as defined in the BEST (Biomarkers, EndpointS, and Other Tools) glossary, are specific characteristics that can be objectively measured and quantified.47 They can indicate normal biological processes, disease states, or responses to treatment. The FDA/CDER launched the Biomarker Qualification Program to develop biomarkers and provide a framework for review and regulatory decisions.47
Tissue biomarkers. Tissue biomarkers offer substantial value in evaluating healing outcomes and informing standard of care, particularly because these readily accessible biomaterials can be analyzed using routine dermatopathology immunostains to predict clinical outcomes.48
Systemic biomarkers. Although localized to a specific body location (eg, foot, leg), a nonhealing wound inherently has systemic manifestations that can be measured in blood, serum, urine, and exudates. Thus, there are potential measurable biomarkers that can predict clinical outcomes of healing based on their systemic presence.49
Point-of-care devices for assessing local and systemic biomarkers for wound healing are currently undergoing various stages of development and validation. The introduction of advanced tools and technologies such as near-infrared spectroscopy, thermography, and fluorescence imaging can help objectively quantify findings.50-52 These methods can assess molecules present in debrided tissue biomaterial, wound dressings, and wound fluid, potentially offering more detailed insights into the healing trajectory.
Proteases. Human and bacterial proteases are important biomarkers in wound healing; they play roles in the inflammatory response, tissue remodeling, and infection. Elevated protease activity has been recognized to be associated with impaired healing.53 An imbalance between matrix metalloproteinases (MMPs) and their natural inhibitors, tissue inhibitors of metalloproteinases (TIMPs), plays a critical role in impaired wound healing. Various approaches have been employed to measure their levels and ratios, which are often used to assess wound status and forecast healing outcomes.54 In addition, bacteria found in wounds produce proteases that impair healing and promote infections.54 Various methods exist for protease detection and quantification, but only a limited number of these point-of-care devices are FDA 510(K) cleared.
pH. The pH characteristics of wounds play a critical role in understanding their microenvironment, which can aid in assessment. The skin typically maintains an acidic pH, usually between 4 and 6.55 Physiological wounds often exhibit a temporary shift toward acidosis, resulting in a progression of wound pH from neutral to acidic as healing takes place. An alkaline pH may suggest a slower healing process.55 It is also important to note that pathogenic bacteria thrive in environments where the pH exceeds 6. Thus, monitoring wound pH can potentially help in predicting or detecting infections and assessing whether a wound is responding effectively to treatment.
Oxygenation. Chronic wounds, such as DFUs, venous ulcers, and pressure ulcers, frequently have impaired oxygen delivery due to inadequate circulation or other underlying health issues.56 Clinicians can assess oxygen levels to predict a wound’s healing potential, determining whether it might heal on its own or requires advanced treatment, such as hyperbaric oxygen therapy or vascular surgery. Hypoxia in these wounds signals poor healing capability and may warrant more intensive wound care strategies, including enhancing blood flow or implementing oxygen therapy to facilitate healing.56
FDA Biomarker Qualification Program integration. The FDA Biomarker Qualification Program, established under the 21st Century Cures Act, provides a structured pathway for developing and qualifying biomarkers to support regulatory decision-making across drug development programs and offers significant opportunities to advance wound care through the use of validated, standardized biomarker tools.57 The Biomarker Qualification Program involves 3 stages: (1) Letter of Intent submission outlining the proposed biomarker and intended context of use, (2) Qualification Plan development detailing the analytical and clinical validation strategy, and (3) Full Qualification Package submission with comprehensive evidence supporting the biomarker’s reliability and clinical utility.57 Biomarkers relevant to wound healing that may benefit from the qualification process include tissue-based protease activity ratios (MMP/TIMP) for predicting healing trajectory, systemic inflammatory markers for assessing wound chronicity, point-of-care pH and oxygenation measurements for treatment selection, molecular signatures from wound fluid or tissue biopsies for infection detection, and imaging-based biomarkers for objective wound assessment.
Sponsors developing wound care products should consider engaging with the Biomarker Qualification Program when the proposed biomarker addresses an unmet need in wound assessment or treatment selection, sufficient preliminary data exist to support the biological rationale and analytical methodology, the biomarker has potential utility across multiple wound types or treatment modalities, and collaborative development with other sponsors or academic institutions is feasible.19 Qualified biomarkers provide several benefits, including reduced regulatory uncertainty, potential for accelerated development pathways, enhanced trial efficiency through enrichment strategies, and improved postmarket surveillance capabilities.19 For wound care, in which traditional end points such as complete closure may require extended observation periods, qualified biomarkers could enable earlier go/no-go decisions and more efficient dose-finding studies.
The WCCC recommends that wound care stakeholders jointly develop and qualify biomarkers of common interest, leveraging shared resources and expertise while reducing individual sponsor burden. This collaborative approach aligns with the FDA’s encouragement of multisponsor biomarker development initiatives and could accelerate the availability of validated tools for the entire wound care community.
Sponsors interested in biomarker qualification should engage early with the FDA through presubmission meetings to discuss their development strategy and ensure alignment with regulatory expectations before initiating formal qualification activities.19
Study populations
Selecting the appropriate patient population in clinical trials is critical to producing results that are both scientifically valid and relevant to real-world practice. Trials must balance the need for a homogeneous group (thus reducing variability and increasing statistical power) with the need for generalizability so that results apply to the broader patient population. The WCCC’s Natural History Project was established to document the real-world course of patients with chronic wounds, including wound severity, outcomes, time to heal, and comorbidities. Its goals are to provide a “reality check” against trial populations, illustrate the limited generalizability of most DFU randomized controlled trials, and assess whether wound outcomes relate more to type or severity.
Initial findings from the WCCC’s Natural History Project reveal a persistent gap between trial populations and the patients most clinicians see:
• DFU trials remain narrow. Most still enroll only Wagner grade 1 or “grade 2 without exposed bone” ulcers, excluding patients with common comorbidities such as autoimmune disease or end-stage renal disease.
• Criteria vs reality. Even when protocols appear broader, actual enrollment often skews toward patients who are likely to heal quickly, such as those with smaller wounds or without severe systemic illness.
• Venous leg ulcer (VLU) trials show similar issues. While protocols may list fewer exclusions, real-world enrollment often omits patients with significant comorbidities, and follow-up is typically limited to approximately 12 weeks.
With few exceptions, DFU and VLU trial populations do not reflect the complexity or severity seen in routine practice. This misalignment limits the applicability of trial findings and underscores the need for designs that capture the true diversity of patients who will receive these treatments.
Efficacy end points
In wound healing research, the precise definition of primary and secondary end points is of utmost importance. These end points must be relevant and inclusive of both clinical and patient-reported outcomes to facilitate a thorough assessment of treatment efficacy. The selection of effective end points requires a clear establishment of parameters that genuinely represent treatment outcomes in wound healing. Efficacy end points, including time to wound closure and healing quality, should be prioritized. Notably, the Wound-care Experts/ FDA-Clinical Endpoints Project has identified and validated 15 clinically meaningful and patient-centered end points through a collaborative effort with the FDA58-61 (Table). This initiative involved comprehensive surveys of clinicians and patients, coupled with rigorous evidence research.58-61
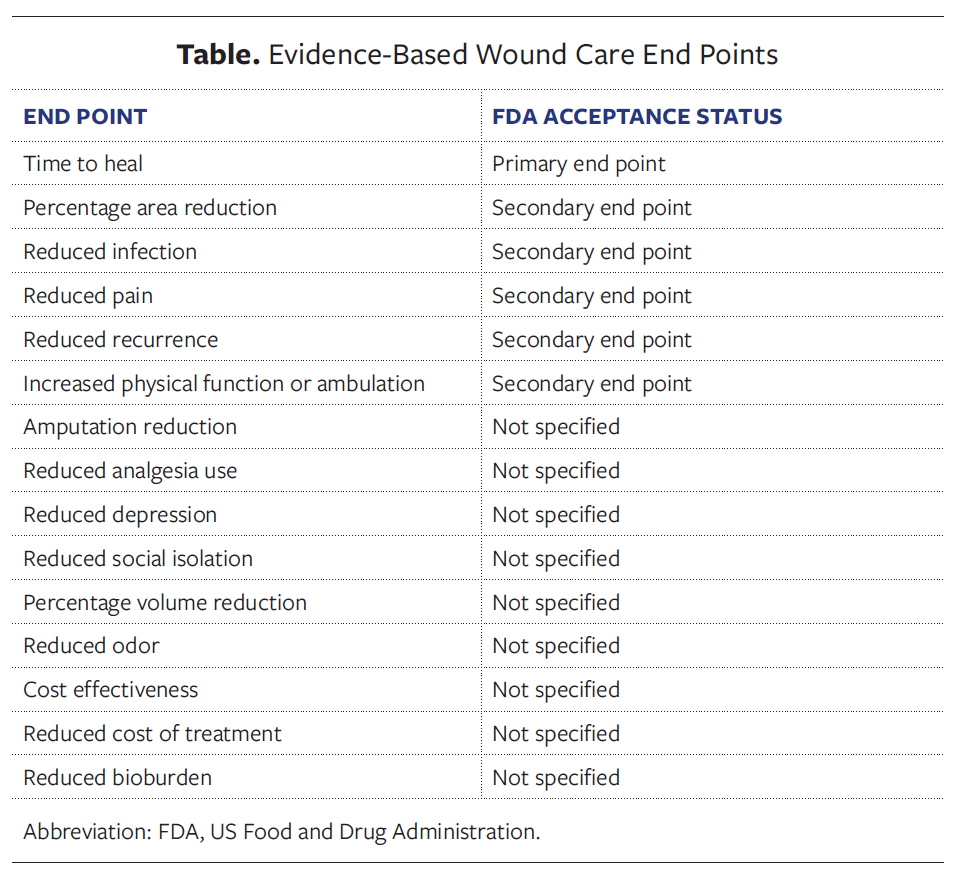
The FDA continues to recommend complete wound closure (100% epithelialization without drainage or dressing requirements) as the most objective and clinically meaningful end point for wound healing trials intended to support a product for treatment, while acknowledging there is interest in alternative end points.58 If alternative end points are proposed for wound healing treatment indications, such end points must reflect benefits that are clinically meaningful to patients, improving how they feel, function, or survive. For example, PAR alone is not considered clinically meaningful.19 This was reinforced in the 2022 FDA wound healing scientific workshop, where patients suggested that a 50% area reduction alone—especially on critical areas like the sole of the foot—was insufficient for meaningful improvement in daily life (eg, mobility, bathing).22 Therefore, to support a drug’s or biologic’s efficacy for treatment of a chronic wound, PAR alone likely could not serve as a primary end point; however, it might be acceptable in combination with another clinically meaningful co-primary or multicomponent end point (eg, improved pain, reduced infection, better ambulation).19 To assess whether PAR plus improvement in a patient-reported outcome is clinically meaningful, sponsors could consider first conducting cognitive interviews and surveys with patients and then, in clinical trials, conducting exit interviews with subjects to ensure that the subjects who achieved the end point were satisfied with the intervention. Regardless of which end point is selected, sponsors should engage with the FDA prior to initiation of pivotal trials to obtain alignment on proposed end points to support efficacy.19
Innovative trial design
Chronic wounds present unique challenges for clinical trial design due to the heterogeneity of underlying healing barriers, even within the same wound subtype. Although all wounds progress through the classic stages of healing (inflammation, proliferation, and remodeling), with common pathways such as granulation tissue formation and epithelialization, the primary impediments to healing can vary substantially between patients.62
For example, in a cohort of 100 subjects with DFUs, the distribution of primary healing barriers might include 30% with infection-related impediments, 40% with poor blood flow, 20% with excessive inflammation, and 10% with unknown factors. These distinct biological mechanisms require different therapeutic approaches, suggesting that traditional “one-size-fits-all” trial designs may not optimally demonstrate treatment effects for wound healing products. Therefore, inclusion of descriptions of innovative trial designs would be a helpful addition to the FDA guidance document.19
Umbrella trial design. An umbrella trial studies multiple therapies within a single disease type, typically stratified by biomarkers or subject characteristics.63 For wound healing applications, subjects would be stratified based on specific biological barriers to healing and matched to appropriate targeted therapies. “Sponsors should consider umbrella trial designs when multiple therapeutic mechanisms are being investigated for the same wound type, when validated biomarkers or clinical characteristics can identify distinct healing barriers, and when the goal is to demonstrate targeted efficacy in biologically defined subpopulations.” (K.D. Verma, MD, FDA Center for Drug Evaluation and Research. Written communication, October 10, 2025.)
An umbrella trial on DFUs could randomize subjects based on biological features, with subjects demonstrating high local inflammation receiving anti-inflammatory interventions, subjects with poor vascularization receiving angiogenic therapy, and subjects with high bacterial biofilm burden receiving antimicrobial treatment. Each subgroup would receive tailored treatment in addition to standard of care within a single trial framework.” (K.D. Verma, MD, FDA Center for Drug Evaluation and Research. Written communication, October 10, 2025.)
“Umbrella trials might serve as proof-of-concept studies to inform later-phase development. Sponsors should consider that results may support biomarker-enriched phase 3 trials with potentially larger treatment effects, although generalizability to broader patient populations should be addressed, and labeling and indication scope may be affected by the enriched population studied.” (K.D. Verma, MD, FDA Center for Drug Evaluation and Research. Written communication, October 10, 2025.)
Basket trial design. Basket trials test a single therapy across multiple diseases or conditions that share a common biological feature or mechanism.64 These trials are appropriate when the investigational product targets a common biological pathway across different wound types, when efficiency in gathering broader efficacy data is desired, and when mechanistic rationale supports efficacy across multiple wound etiologies. “For example, a topical regenerative therapy targeting angiogenesis could potentially be studied simultaneously across multiple wound types with impaired vascularization, including DFUs, VLUs, and pressure ulcers.” (K.D. Verma, MD, FDA Center for Drug Evaluation and Research. Written communication, October 10, 2025.)
Platform trial design. Platform trials test multiple therapies under a single master protocol, with the ability to add, drop, or modify treatment arms as data emerge.65 These trials offer flexibility for testing multiple interventions simultaneously, making adaptive modifications based on interim analyses, and ensuring efficient use of trial infrastructure and patient populations. A platform trial could include multiple arms based on wound subtype and biological characteristics, such as DFUs with high inflammation receiving anti-inflammatory gel, DFUs with poor blood flow receiving pro-angiogenic therapy, and VLUs with specific biomarker profiles receiving targeted treatment.19
Limitations
These recommendations reflect current evidence, but they may require revision as wound healing science, diagnostic technologies, and regulatory expectations continue to evolve. Variability across preclinical models, clinical study designs, biomarker methodologies, and digital imaging tools limits the generalizability of some recommendations; many emerging approaches lack extensive validation in chronic wound populations.
Clinical trial populations often remain narrower and healthier than the broader chronic wound population, thus constraining the applicability of these recommendations to routine practice. Standardization of preclinical models, bioassays, and photographic techniques is recommended, but such standardization may be challenging to implement consistently due to resource and technical constraints. Moreover, animal models remain inherently limited in their ability to replicate human chronic wound biology, restricting translation of nonclinical findings.
Finally, this report serves as a proposed addendum and does not replace formal FDA guidance. Sponsors must interpret these recommendations within the context of product specific regulatory pathways and ongoing agency feedback.
Conclusion
The WCCC presents this proposed addendum to the 2006 FDA guidance for industry on chronic cutaneous ulcers and burn wounds with the intent to modernize and strengthen regulatory pathways for chronic wound treatment products. By integrating contemporary scientific advancements, real-world clinical insights, and stakeholder consensus, these recommendations aim to enhance the safety, efficacy, and accessibility of wound care innovations.
Key updates include the incorporation of validated bioassays, refined animal model selection, and the adoption of standardized reporting frameworks (eg, WRAHPS). The current report also emphasizes the importance of robust clinical trial design, including the use of digital imaging technologies, biomarker integration, and innovative trial methodologies such as umbrella, basket, and platform designs. These strategies are intended to better reflect the biological complexity of chronic wounds and improve the generalizability of clinical findings.
Furthermore, the WCCC underscores the need for alignment between trial populations and real-world patients, and thus, advocates for end points that are both clinically meaningful and patient-centered. By addressing gaps in the original guidance, such as biofilm detection, ulcer classification, and the role of systemic and tissue biomarkers, this proposed addendum provides a comprehensive framework to support the development of next-generation wound therapies.
The WCCC encourages continued collaboration among regulators, clinicians, researchers, and industry partners to ensure that regulatory guidance evolves in step with scientific progress. Through these collective efforts, it is possible to accelerate the delivery of safe, effective, and innovative treatments to the millions of patients affected by chronic wounds.
Author and Public Information
Authors: Windy Cole, DPM1; Mitch Sanders, PhD2; Vickie Driver, DPM3; Marissa Carter, PhD4; Peggy Dotson, RN3; Caroline Fife, MD5; Sarah Griffiths Langbord, PhD6; Franics James, BFA7; Holly Korzendorfer, PT, PhD8; Maribel Henao, DPM, MSPT9; Alisha Oropallo, MD10; Joseph Rolley, MSIA11; Robert Snyder, DPM, MSc, MBA12; Marjana Tomic-Canic, PhD13; Zweli Tunyiswa, BA14; and Howard Walthall, JD, BSE15
Affiliations: 1College of Podiatric Medicine, Kent State University, Kent, OH; 2ProDevLabs, Southborough, MA; 3Wound Care Collaborative Community, Malvern, PA; 4Strategic Solutions, Inc, Oak Brook, IL; 5Intellicure, LLC, The Woodlands, TX; 6NOxy Health Products, San Mateo, CA; 7TRUE-See, New Orleans, LA; 8Marist University, Poughkeepsie, NY; 9Organogenesis, Canton, MA; 10Northwell Health, New Hyde Park, NY; 11JTR Business Consulting, LLC, Doylestown, PA; 12MediWound, Wilmington, DE; 13Miller School of Medicine, University of Miami, Miami, FL; 14Open Wound Research, Puyallup, WA; 15Venture Medical, LLC, Missoula, MT
Disclosures: The authors disclose no financial or other conflicts of interest.
Author Contributions: All authors participated in critical review of the manuscript for intellectual content and approved the final version.
Acknowledgments: The authors would like extend their deep appreciation to Dev Verma, MD, Division of Dermatology and Dentistry, Center for Drug Evaluation and Research, US Food and Drug Administration, for his expert guidance and contributions to the development and refinement of this manuscript. We also would like to express our sincere gratitude to Cat Thompson, Executive Director of the Wound Care Collaborative Community, for her invaluable logistical support throughout the preparation of this work.
Correspondence: Windy Cole, DPM; College of Podiatric Medicine, Kent State University, 6000 Rockside Woods Blvd, Independence, OH 44242-0001; drwec@yahoo.com
Manuscript Accepted: May 13, 2026
References
- McDermott K, Fang M, Boulton AJM, Selvin E, Hicks CW. Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care. 2023;46(1):209-221. doi:10.2337/dci22-0043
- Pastar I, Balukoff NC, Marjanovic J, Chen VY, Stone RC, Tomic-Canic M. Molecular pathophysiology of chronic wounds: Current state and future directions. Cold Spring Harb Perspect Biol. 2023;15(4):a041243. doi:10.1101/cshperspect.a041243
- Eming SA, Martin P, Tomic-Canic M. Wound repair and regeneration: Mechanisms, signaling, and translation. Sci Transl Med. 2014;6(265):265sr6. doi:10.1126/scitranslmed.3009758
- US Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research, Center for Biologics Evaluation and Research, Center for Devices and Radiological Health: Guidance for industry: chronic cutaneous ulcer and burn wounds—developing products for treatment; June 2006. Accessed September 16, 2025. https://www.fda.gov/media/71278/download
- Darwin E, Tomic-Canic M. Healing chronic wounds: Current challenges and potential solutions. Curr Dermatol Rep. 2018;7(4):296-302. doi:10.1007/s13671-018-0239-4
- Simon CG Jr, Bozenhardt EH, Celluzzi CM, et al. Analysis of the measurements used as potency tests for the 31 US FDA-approved cell therapy products. J Transl Med. 2025;23(1):259. doi:10.1186/s12967-025-06253-4
- US Food and Drug Administration. M3(R2) Nonclinical safety studies for the conduct of human clinical trials and marketing authorization for pharmaceuticals. January 2010. Accessed September 16, 2025. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/m3r2-nonclinical-safety-studies-conduct-human-clinical-trials-and-marketing-authorization.
- US Department of Health and Human Services, Food and Drug Administration, Center for Biologics Evaluation and Research. Guidance for Industry: Potency Tests for Cellular and Gene Therapy Products; January 2011. Accessed September 16, 2025. https://www.fda.gov/files/vaccines,%20blood%20%26%20biologics/published/Final-Guidance-for-Industry--Potency-Tests-for-Cellular-and-Gene-Therapy-Products.pdf.
- Ojeh N, Vecin NM, Pastar I, et al: The Wound Reporting in Animal and Human Preclinical Studies (WRAHPS) Guidelines. Wound Repair Regen. 2025;33(1):e13232. doi:10.1111/wrr.13232
- Flynn K, Mahmoud NN, Sharifi S, Gould LJ, Mahmoudi M. Chronic wound healing models. ACS Pharmacol Transl Sci. 2023;6(5):783-801. doi:10.1021/acsptsci.3c00030
- FDA, ICH, and the 3Rs Paul C. Brown, PhD Center for Drug Evaluation and Research Food and Drug Administration. September 2020. Accessed September 16, 2025. https://www.fda.gov/media/143220/download
- US Food and Drug Administration. General Considerations for Animal Studies Intended to Evaluate Medical Devices. Guidance for Industry and Food and Drug Administration Staff. March 28, 2023US Food and Drug Administration. Accessed September 16, 2025. https://www.fda.gov/media/93963/download.
- Sullivan TP, Eaglstein WH, Davis SC, Mertz P. The pig as a model for human wound healing. Wound Repair Regen. 2001;9(2):66-76. doi:10.1046/j.1524-475X.2001.00066.x
- Nowak-Sliwinska P, Segura T, Iruela-Arispe ML. The chicken chorioallantoic membrane model in biology, medicine and bioengineering. Angiogenesis. 2014;17(4):779-804. doi:10.1007/s10456-014-9440-7
- Ansell DM, Marsh C, Walker L, Hardman MJ, Holden K. Evaluating STZ-induced impaired wound healing in rats. J Invest Dermatol. 2018;138(4):994-997. doi:10.1016/j.jid.2017.10.020
- Masson-Meyers DS, Andrade TAM, Caetano GF, et al. Experimental models and methods for cutaneous wound healing assessment. Int J Exp Pathol. 2020;101(1-2):21-37. doi:10.1111/iep.12346
- Dhall S, Do DC, Garcia M, et al. Generating and reversing chronic wounds in diabetic mice by manipulating wound redox parameters. J Diabetes Res. 2014;2014:562625. doi:10.1155/2014/562625
- Rittié L. Cellular mechanisms of skin repair in humans and other mammals. J Cell Commun Signal. 2016;10(2):103-120. doi:10.1007/s12079-016-0330-1
- Verma KD, Lewis F, Mejia M, Chalasani M, Marcus KA. Food and Drug Administration perspective: Advancing product development for non-healing chronic wounds. Wound Repair Regen. 2022 May;30(3):299-302. doi: 10.1111/wrr.13008
- Altman DG, Bland JM. How to randomise. BMJ. 1999;319(7211):703-704. doi:10.1136/bmj.319.7211.703
- European Medicines Agency. ICH Topic E 10: Choice of Control Group in Clinical Trials; January 2001. Accessed September 16, 2025. https://www.ema.europa.eu/en/documents/scientific-guideline/ich-e-10-choice-control-group-clinical-trials-step-5_en.pdf
- US Food and Drug Administration. Public Workshop: FDA Wound healing scientific workshop, April 28-29, 2022. Accessed February 18, 2024. https://www.fda.gov/drugs/news-events-human-drugs/public-workshop-fda-wound-healing-scientific-workshop-04282022
- Nayler JR. Clinical photography: A guide for the clinician. J Postgrad Med. 2003;49(3):256-262.
- Prasad S, Roy B. Digital photography in medicine. J Postgrad Med. 2003;49(4):332-336.
- Petersilge CA. Fundamentals of enterprise photodocumentation: Connecting the clinical and technical—a review of key concepts. J Digit Imaging. 2019;32(6):1052-1061. doi:10.1007/s10278-019-00212-4
- Zoltie T, Blome-Eberwein S, Forbes S, Theaker M, Hussain W. Medical photography using mobile devices. BMJ. 2022;378:e067663. doi:10.1136/bmj-2021-067663
- Wongvibulsin S, Feterik K. Recommendations for better adoption of medical photography as a clinical tool. Interact J Med Res. 2022;11(2):e36102. doi:10.2196/36102
- Gallagher BA. Wound Bed Assessment Using Calibrated Images and Representation in OpenEHR. Dissertation. University of Dublin; 2012.
- Korzendorfer H, Dotson P, James F, Cole W, Oropallo A. An overview and survey of US Food and Drug Administration–registered wound imaging devices capable of determining percentage area reduction and/or percentage volume reduction. Wounds. 2025;37(5):210-219. doi:10.25270/wnds/24201
- Maglogiannis I, Kosmopoulos DI. A system for the acquisition of reproducible digital skin lesions images. Technol Health Care. 2003;11(6):425-441.
- Chairat S, Chaichulee S, Dissaneewate T, Wangkulangkul P, Kongpanichakul L. AI-assisted assessment of wound tissue with automatic color and measurement calibration on images taken with a smartphone. Healthcare (Basel). 2023;11(2):273. doi:10.3390/healthcare11020273
- Penczek J, Boynton PA, Splett JD. Color error in the digital camera image capture process. J Digit Imaging. 2014;27(2):182-191. doi:10.1007/s10278-013-9644-1
- Bloemen EM, Rosen T, Schiroo JAC, et al. Photographing injuries in the acute care setting: Development and evaluation of a standardized protocol for research, forensics, and clinical practice. Acad Emerg Med. 2016;23(5):653-659. doi:10.1111/acem.12955
- Oropallo A, Dotson P, Franzen-Korzendorfer H, et al. Standardizing medical photo acquisition to improve image quality. Abstract presented at: SAWC Spring 2025; April 30-May 4, 2025, Grapevine, TX. CR-065. Accessed September 15, 2025. https://d148x66490prkv.cloudfront.net/hmp_ln/supplements/2025-05/SAWC_2025Spring_Abstracts-Approved.pdf.
- Lucas Y, Niri R, Treuillet S, Douzi H, Castaneda B. Wound size imaging: Ready for smart assessment and monitoring. Adv Wound Care (New Rochelle). 2021;10(11):641-661. doi:10.1089/wound.2018.0937
- Shah A, Wollak C, Shah JB. Wound measurement techniques: Comparing the use of ruler method, 2D imaging and 3D scanner. J Am Coll Clin Wound Spec. 2015;5(3):52-57. doi:10.1016/j.jccw.2015.02.001
- Wendland DM, Taylor DWM. Wound measurement tools and techniques: A review. Journal of Acute Care Physical Therapy. 2017;8(2):42-57. doi:10.1097/JAT.0000000000000050
- Rogers LC, Bevilacqua NJ, Armstrong DG, Andros G. Digital planimetry results in more accurate wound measurements: A comparison to standard ruler measurements. J Diabetes Sci Technol. 2010;4(4):799-802. doi:10.1177/193229681000400405
- National Pressure Injury Advisory Panel. NPIAP Pressure Injury Staging. Accessed September 16, 2025. https://npiap.com/page/PressureInjuryStaging
- Wagner FW. Diabetic foot study. Surg Clin North Am. 1981;61(4):659-668. doi:10.1016/S0039-6109(16)42054-7
- Oyibo SO, Jude EB, Tarawneh I, Nguyen HC, Harkless LB, Boulton AJ. A comparison of two diabetic foot ulcer classification systems: the Wagner and the University of Texas wound classification systems. Diabetes Care. 2001;24(1):84-88. doi:10.2337/diacare.24.1.84
- Ince P, Abbas ZG, Lutale JK, et al. Use of the SINBAD classification system and score in comparing outcome of foot ulcer management on three continents. Diabetes Care. 2008;31(5):964-967. doi:10.2337/dc07-2367
- International Working Group on the Diabetic Foot. IWGDF guideline on the classification of diabetic foot ulcers. 2019. Accessed September 16, 2025. https://iwgdfguidelines.org/wp-content/uploads/2019/05/07-IWGDF-classification-guideline-2019.pdf
- James GA, Swogger E, Wolcott R, et al. Biofilms in chronic wounds. Wound Repair Regen. 2008;16(1):37-44. doi:10.1111/j.1524-475X.2007.00321.x
- Badrie S, Moore Z, Patton D, O’Connor T, Derwin R. The clinical utility of autofluorescence imaging for bacterial detection in wounds: A systematic review. Int Wound J. 2025;22(6):e70678. doi:10.1111/iwj.70678
- Uberoi A, McCready-Vangi A, Grice EA. The wound microbiota: Microbial mechanisms of impaired wound healing and infection. Nat Rev Microbiol. 2024;22(8):507-521. doi:10.1038/s41579-024-01035-z
- FDA-NIH Biomarker Working Group. BEST (Biomarkers, EndpointS, and other Tools) Resource [Internet]. Food and Drug Administration (US), National Institutes of Health (US); January 28, 2016. Updated January 16, 2025. https://www.ncbi.nlm.nih.gov/books/NBK338448/
- Kirsner RS, Pastar I, Krambrink A, et al. Evaluation of c-Myc and phosphorylated glucocorticoid receptor (p-GR) for predicting diabetic foot ulcer healing—a Diabetic Foot Consortium study. Wound Repair Regen. 2025;33(3):e70044. doi:10.1111/wrr.70044
- Jones TLZ, Holmes CM, Katona A, et al. The NIDDK Diabetic Foot Consortium. J Diabetes Sci Technol. 2023;17(1):7-14. doi:10.1177/19322968221121152
- Manley M. Near-infrared spectroscopy and hyperspectral imaging: non-destructive analysis of biological materials. Chem Soc Rev. 2014;43(24):8200-8214. doi:10.1039/c4cs00062e
- Lu Y, Sun N, Wu P, Zhou G, Peng L, Tang J. The application of infrared thermography technology in flap: A perspective from bibliometric and visual analysis. Int Wound J. 2023;20(10):4308-4327. doi:10.1111/iwj.14333
- Le L, Baer M, Briggs P, et al. Diagnostic accuracy of point-of-care fluorescence imaging for the detection of bacterial burden in wounds: Results from the 350-patient fluorescence imaging assessment and guidance trial. Adv Wound Care (New Rochelle). 2021;10(3):123-136. doi:10.1089/wound.2020.1272
- Acosta JB, del Barco DG, Vera DC, et al. The pro-inflammatory environment in recalcitrant diabetic foot wounds. Int Wound J. 2008;5(4):530-539. doi:10.1111/j.1742-481X.2008.00457.x
- Weigelt MA, Lev-Tov HA, Tomic-Canic M, et al. Advanced wound diagnostics: Toward transforming wound care into precision medicine. Adv Wound Care (New Rochelle). 2022;11(6):330-359. doi:10.1089/wound.2020.1319
- Sim P, Strudwick XL, Song Y, Cowin AJ, Garg S. Influence of acidic pH on wound healing in vivo: A novel perspective for wound treatment. Int J Mol Sci. 2022;23(21):13655. doi:10.3390/ijms232113655
- Sen CK. Wound healing essentials: Let there be oxygen. Wound Repair Regen. 2009;17(1):1-18. doi:10.1111/j.1524-475X.2008.00436.x
- US Food and Drug Administration. Biomarker qualification program. Content current as of May 16, 2025. Accessed September 16, 2025. https://www.fda.gov/drugs/drug-development-tool-ddt-qualification-programs/biomarker-qualification-program
- Driver VR, Gould LJ, Dotson P, et al. Identification and content validation of wound therapy clinical endpoints relevant to clinical practice and patient values for FDA approval. Part 1. Survey of the wound care community. Wound Repair Regen. 2017;25(3):454-465. doi:10.1111/wrr.12533
- Driver VR, Gould LJ, Dotson P, Allen LL, Carter MJ, Bolton LL. Evidence supporting wound care end points relevant to clinical practice and patients’ lives. Part 2. Literature survey. Wound Repair Regen. 2019;27(1):80-89. doi:10.1111/wrr.12676
- Gould LJ, Liu J, Wan R, Carter MJ, Dotson MP, Driver VR. Evidence supporting wound care end points relevant to clinical practice and patients’ lives. Part 3: The patient survey. Wound Repair Regen. 2021;29(1):60-69. doi:10.1111/wrr.12872
- Driver VR, Wathall H, Oropallo A, et al. Collaboration encourages innovation: setting new standards in wound care with the Wound Care Collaborative Community Expert Panel consensus recommendations. Wounds. 2024;36(12):410-418. doi:10.25270/wnds/24186
- Schultz GS, Chin GA, Moldawer L, Diegelmann RF. Principles of wound healing. In: Fitridge R, Thompson M, eds. Mechanisms of Vascular Disease: A Reference Book for Vascular Specialists. University of Adelaide Press; 2011:chap 23.
- Ouma LO, Wason JMS, Zheng H, Wilson N, Grayling M. Design and analysis of umbrella trials: Where do we stand? Front Med (Lausanne). 2022;9:1037439. doi:10.3389/fmed.2022.1037439
- Duan XP, Qin BD, Jiao XD, Liu K, Wang Z, Zang YS. New clinical trial design in precision medicine: discovery, development and direction. Signal Transduct Target Ther. 2024;9(1):57. doi:10.1038/s41392-024-01760-0
- Woodcock J, LaVange LM. Master protocols to study multiple therapies, multiple diseases, or both. N Engl J Med. 2017;377(1):62-70. doi:10.1056/NEJMra1510062