


The Aero Era: Early Experience With Shockwave C2 Aero
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Christopher L. Brown, MD
Swedish Heart and Vascular Institute, Swedish Medical Center, Seattle, Washington
Can you tell us about your practice and the kinds of patients that you see?
 I run the complex coronary program at Swedish Medical Center in Seattle. We are a large coronary care center and do more than 1,000 percutaneous coronary interventions (PCIs) a year, over 500 transcatheter aortic replacements, and more than 300 other valvular interventions. My work is mostly complex coronary disease and complex peripheral vascular disease. Because of the amount of calcified disease we treat, we use a lot of lithotripsy, atherectomy, and other plaque-modification tools.
I run the complex coronary program at Swedish Medical Center in Seattle. We are a large coronary care center and do more than 1,000 percutaneous coronary interventions (PCIs) a year, over 500 transcatheter aortic replacements, and more than 300 other valvular interventions. My work is mostly complex coronary disease and complex peripheral vascular disease. Because of the amount of calcified disease we treat, we use a lot of lithotripsy, atherectomy, and other plaque-modification tools.
Tell us about your experience with the Shockwave C2 Aero.
We had early access to the Shockwave C2 Aero from Johnson & Johnson MedTech. We’ve had it for more than 6 months and to me, the Shockwave C2 Aero feels less like a small iteration and more like a meaningful change. I was skeptical at first, honestly. I like the company and I’ve always thought Shockwave is a good device, but every company’s “next generation” tends to come with bold claims attached to it. I was excited that they were trying to make it more deliverable, but I wanted to use it myself before offering feedback. I’ll admit I’ve had to bite my tongue, because they under-promised and over-delivered, which is pretty rare, especially in the device space.
The balloon feels genuinely redesigned. It has different polymer and different balloon behavior, and it addresses what has always been the main limitation, which is getting an intravascular lithotripsy (IVL) balloon to deliver in the very calcified vessels you are treating. With the prior Shockwave C2+, the balloon felt more deliverable than a cutting balloon but wasn’t on-par with a Takeru-type balloon (Terumo), so deliverability was something operators and cath labs had to plan around. We leaned on guide extensions, Wiggle wires (Abbott Vascular), and a lot of workarounds.
With the Shockwave C2 Aero, the balloon coating is completely different. It is hydrophilic and extremely slippery, in a good way. The balloon material is also more flexible, and the tip is more tapered, which helps you seat into the lesion and advance more confidently. All of those changes probably contribute, but I think the real lift is the polymer and the surface of the balloon.
The difference shows up when you are trying to treat more than one vessel. Before, if we treated a left anterior descending (LAD) and wanted to use the same balloon in a calcified circumflex, we often had to do a fair amount of prep just to get the balloon into the second vessel. With the Shockwave C2 Aero balloon, we’ve needed much less of that. There are cases where we have gone in without predilation in lesions where we previously would have needed to escalate from a 1.5 mm balloon to a Takeru 2.0 mm, maybe even a 2.5 mm non-compliant balloon, just to get the IVL balloon to deliver. Shockwave C2 Aero just delivers.
The other big change is rewrap. In my experience, after treatment, the balloon comes back down and rewraps much tighter than the Shockwave C2+ balloon, which makes it easier to reposition and remove.
Overall, the outside of the Shockwave C2 Aero balloon, its deliverability and rewrap are the most striking differences for me.
How has the performance of Shockwave C2 Aero impacted your treatment algorithm for coronary calcification?
From my perspective, it changes a lot. It does not eliminate atherectomy. There will always be cases where you still need a Rotablator (Boston Scientific) but it shifts the line of when you have to reach for it. There are vessels where we used to spend a lot of time just doing lesion prep to get a Shockwave across, or we would move to atherectomy first to create space and then come back with lithotripsy. With Shockwave C2 Aero more of those cases can be treated with lithotripsy alone.
It also makes it easier to extend IVL into additional vessels during the same case. I don’t always need 120 pulses in a LAD. I might need 80 in the LAD and 40 in the circumflex, but in the past, getting the balloon into the circumflex for those 40 pulses sometimes took a lot of extra work. With this balloon, that has been much less of an issue.
When you plan to treat more than one calcified vessel, how do you manage pulses?
We use pulses based on what the lesion length and lesion response required. If I need to deliver 20 pulses, move half a balloon length, deliver another 20, and keep marching through a long calcified segment, then I do that, even if I use all 120 pulses.
What we don’t do is keep firing once we have clearly achieved what we need. If we have already delivered 20, 20, and 20 pulses, the vessel looks compliant, and the segment is adequately treated, there is no reason to use another 60 pulses just because we have them. That said, the reality is the balloon is opened and paid for, so in the past there were times when people would use extra pulses simply because they were available.
The difference now is that any remaining pulses can be put to better use in a second vessel. There were plenty of cases before where we would say, “We have 40 pulses left, but we’re never going to get this balloon down to the mid circumflex.” We would treat the LAD, then end up opening a second balloon because we thought that was best for the patient. Now, if I have pulses left, I can redirect them to the circumflex without overthinking it, because delivery is much more reliable. It makes multivessel calcified PCI, what you could call “percutaneous CABG”, more doable.
What lesion types or locations do you find benefit the most from Shockwave C2 Aero’s improved deliverability and crossability?
Long, heavily calcified lesions benefit the most, especially when you want to deliver the balloon all the way to the distal end of the calcium instead of having to “shockwave” your way through the segment just to advance. Previously, we’d use a guide extension, get the Shockwave balloon as far as we could, treat the tightest or most resistant part, then work to move it farther, sometimes tracking the guide extension to help advance, sometimes repeating the process. We had a lot of tricks to make that work.
With Shockwave C2 Aero we are not doing that nearly as often. We don’t even use guide extensions for delivery in probably three-quarters of cases anymore. It cuts out a lot of the extra work we used to do just to get adequate lesion prep and a good result.
The other major change is multivessel use, especially when you are treating a second lesion or a second vessel. I can’t overstate how big that is. In a surgical turndown with diffuse calcification, being able to treat more of the coronary tree with a single catheter is a real win. It helps the hospital and the system, too, because margins are tight and every device costs something. If you can treat more vessels with one catheter, that is a meaningful improvement.
Case Report: Treating Multivessel Disease With Shockwave C2 Aero
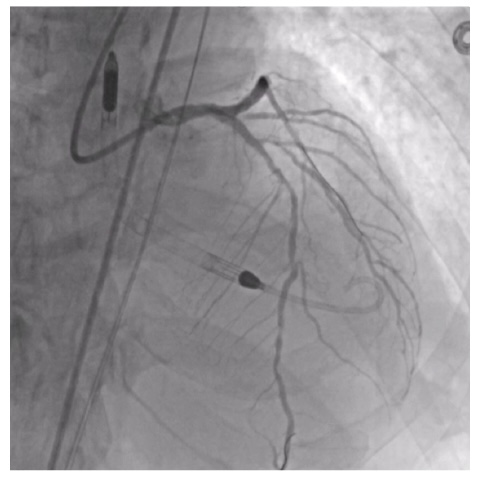
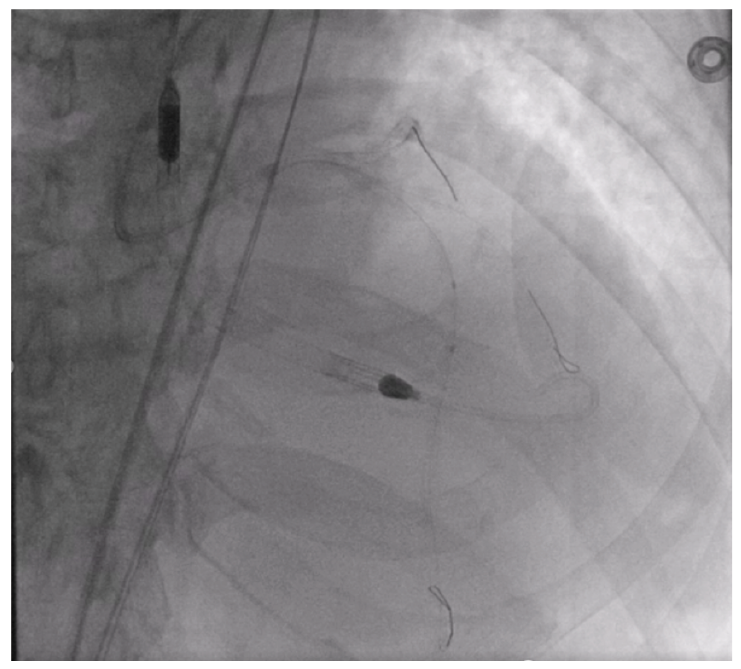
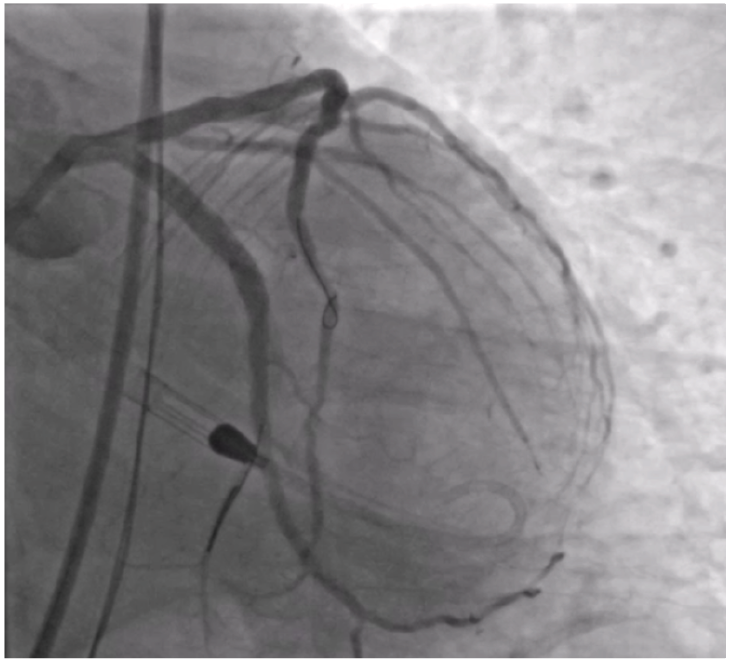
This was an 84-year-old patient with an ejection fraction of 25%. The patient presented with a calcified subtotal proximal circumflex and severe, diffuse calcium in the left anterior descending (LAD) coronary artery (Figures 1-2).
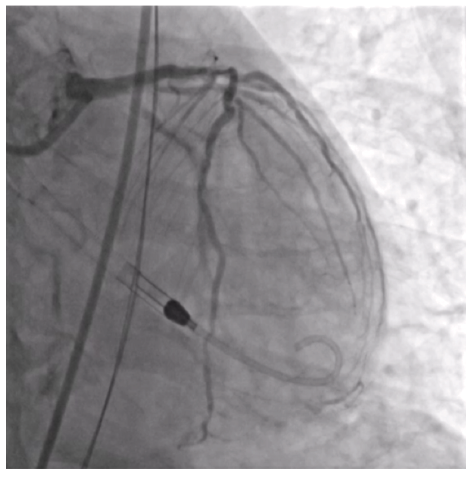
Impella (Abiomed) was chosen due to the lesion complexity and patient characteristics. For large-bore access, the common femoral artery (CFA) was prepped with a Shockwave M5+ to allow for passage of the Impella.
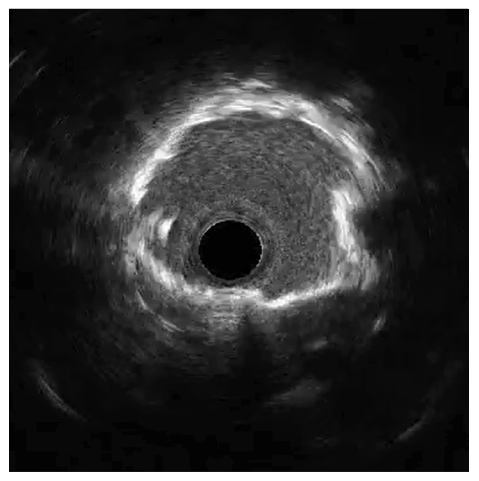
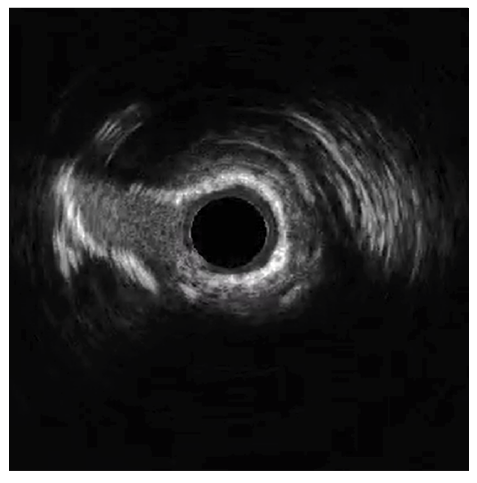
The circumflex (Cx) artery was treated with a 4.0 mm Shockwave C2 Aero due to heavy calcification identified by intravascular ultrasound (IVUS) (Figures 3-4).

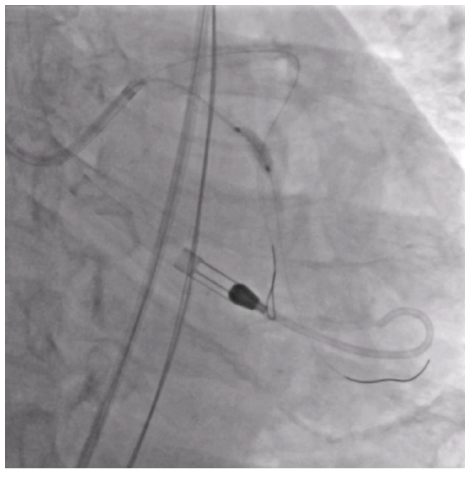
Because of the improved deliverability and crossability with Shockwave C2 Aero, an IVL-first strategy was chosen. Shockwave C2 Aero traversed the vessel well and thus there was no need for a guide extension; the IVL catheter crossed and 60 pulses were delivered to the Cx lesion. Shockwave expanded the calcified segments in the Cx well enough to move forward with stent placement. A 3.5 mm x 38 mm stent expanded well for an excellent result (Figure 5).
The LAD also showed signs of heavy calcification (Figure 6). The LAD was pre-dilated with a 2.0 mm Takeru (Terumo) and used the same Shockwave C2 Aero that was used in the Cx. The rewrapped 4.0 mm Shockwave C2 Aero delivered and crossed the diffuse LAD calcium, and the remaining 60 pulses were used to treat the lesion (Figure 7). The ability to reinsert Shockwave C2 Aero after multiple inflations is a significant benefit not only for multivessel disease but for repositioning in the same vessel. IVL modified the heavily calcified LAD, allowing a drug-eluting stent to pass easily. After multiple stents were placed in the LAD, simultaneous post-dilatation balloon inflations were done in the LAD and Cx to avoid involving the left main, leading to an excellent result (Figure 8).
The deliverability, crossability, and reinsertion ability of Shockwave C2 Aero streamlined this complex case for us. We were able to avoid using adjunctive therapies when treating the Cx by using an IVL-first approach without guide extension support. With the legacy Shockwave C2+ catheter, we likely would have needed additional tools up front to be able to deliver the catheter. We were also able to reinsert the same rewrapped Shockwave C2 Aero catheter to treat the LAD after 60 pulses were used with minimal prep — that is game-changing!
This article is supported by Shockwave Medical.
Dr. Brown is a paid consultant of Shockwave Medical.
SPL-80667 Rev. A Shockwave C2 Aero CLD Article


