

Optimizing Periprocedural Patient Care in EP Labs: Impact of Noninvasive Hemodynamic Monitoring
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2025;25(6):8-10.
Theresa Briggs, MSN, RN, RCIS; Benjamin Olszewski, BSN, RN; Mohammad Mortada, MD; Jeanne Hlebichuk, PhD, RN, NE-BC
Aurora St Luke’s Medical Center, Advocate Health, Milwaukee, Wisconsin
In the rapidly evolving landscape of cardiovascular medicine, optimizing workflow efficiency within the electrophysiology (EP) lab has emerged as a pivotal concern for enhancing patient care and operational performance. EP labs, dedicated to the diagnosis and treatment of cardiac arrhythmias, operate in a high-pressure environment where precision and timeliness are critical. Typically, EP lab procedures consist of 3 phases: intraoperative/periprocedural phase (admission to room to procedure start), procedural phase, and postoperative phase (end of procedure until recovery).
At our 938-bed quaternary medical center, periprocedural efficiency in the EP lab is defined as “wheels in” to the start of the procedure and is crucial for optimizing patient outcomes and maximizing operational throughput. The periprocedural phase includes the time when a patient arrives at the specialized area through initiation of the procedure. This phase represents a crucial opportunity to streamline operations and improve efficiency. Inefficiencies during this phase can lead to delays, increased patient stress, and suboptimal use of resources, all of which impact the overall quality of care. Key aspects of this phase include patient positioning, patient monitoring, anesthesia, and supply readiness.
Patient monitoring consists of electrocardiographic monitoring and measuring invasive blood pressure and oxygen saturation. Invasive blood pressure monitoring has historically been used for precise anesthesia dosing, minimizing its duration and improving patient safety. Invasive monitoring uses arterial access, which increases the patient’s risk for access site infection, access site bleeding and hematoma, vascular injury, and thrombosis formation from the catheter, which could lead to distal limb ischemia.1 Bleeding due to access site complications is the most common adverse outcome, which is associated with increased morbidity and mortality.1
The use of noninvasive hemodynamic monitoring has emerged as a new technique in the EP lab. This technique avoids the risks associated with arterial access, is more comfortable for patients, and requires minimal training for implementation. With noninvasive monitoring, there is a reduction in the need for arterial access, and patient risks associated with invasive monitoring can be mitigated.2 Additional benefits include shorter procedural time and enhanced comfort, which can lead to improved workflow and patient satisfaction.
Noninvasive blood pressure monitoring technologies have been shown to balance the benefits of rapid noninvasive assessments with the critical accuracy of invasive monitoring,3 thereby facilitating improved procedure management and increased throughput in clinical settings. We hypothesized this technology could reduce the length of procedural time4 and potentially reduce complications associated with invasive monitoring. The noninvasive continuous blood pressure measurement technique is based on the volume clamp method. This method involves using an inflatable cuff placed around a finger to create a constant pressure around the artery. By maintaining this constant pressure, the device can detect the changes in arterial volume caused by the pulsatile blood flow with each heartbeat.5
The integration of noninvasive blood pressure monitoring systems into clinical practice has the potential to improve workflow efficiencies, particularly periprocedural time, anesthesia resources, and procedure volumes. However, the change to noninvasive monitoring in clinical practice has not yet fully been integrated into periprocedural practice in the EP lab. Its advantages include ease of application and reduced need for patient preparation, allowing for quicker assessments and continuous monitoring without requiring invasive access. This efficiency can impact periprocedural time, enabling more streamlined workflows and potentially increasing the volume of procedures performed.
Thus, a quality improvement project designed to evaluate the utilization of noninvasive blood pressure monitoring compared to invasive blood pressure monitoring during ablations and left atrial appendage occlusion (LAAO) procedures was initiated by an interdisciplinary team at Aurora St Luke’s Medical Center. The EP program at Aurora St Luke’s Medical Center has 10 electrophysiologists on staff and consists of 4 dedicated EP rooms and 1 shared room with cardiac catheterization. On average, 330 catheter ablations and 250 LAAO procedures are performed annually. The team members involved in the pilot were invasive cardiac technologists, registered nurses, electrophysiologists, and anesthesiologists. The project focused on comparing current practices regarding invasive blood pressure monitoring compared to noninvasive blood pressure monitoring. Specifically, the project sought to identify improvements in procedural workflow efficiencies, patient safety outcomes, and collaboration among patient care providers. The nonprofit health care system institutional review board reviewed the project and determined oversight was not required.
To begin the project, key change agents for use of the noninvasive blood pressure monitoring technology were identified. This included 2 cardiology EP providers (MDs), a nurse educator, and the manager of interventional cardiology. The department manager and educator engaged with the team of early adopters and sought their insights on the use of noninvasive monitoring. Anesthesiology was approached on a case-by-case basis. A company representative for the beat-to-beat noninvasive hemodynamic system provided procedural support as well as training for the physicians and interdisciplinary staff. This real-time support was critical, allowing the team some time to answer questions and to support implementation of the technology.
Following training and logistics, the team began to pilot the use of the noninvasive blood pressure monitoring technology for hemodynamic monitoring as an alternative to invasive arterial lines for 2 EP lab procedures (LAAO and ablations) in June 2024. Patients were excluded from the pilot if they had cardiomyopathy or were in critical condition. To foster confidence in the reliability and accuracy of the noninvasive blood pressure monitoring technology compared to invasive monitoring, both were utilized simultaneously for side-by-side comparison. This comparison provided valuable insights into the reliability and accuracy of noninvasive methods.
The specific process outcome measures compared were total procedure time (procedure start time to out of room) and periprocedural efficiency (time in room to procedure start time). These data points were extracted directly from the electronic health record (EHR) documentation as de-identified data. Additionally, access site location and complications between groups were assessed for safety. Two cardiology/EP providers who were early adopters of the change were selected to include in pre- and post-analysis data due to workflow similarities, to limit confounders and performance bias.
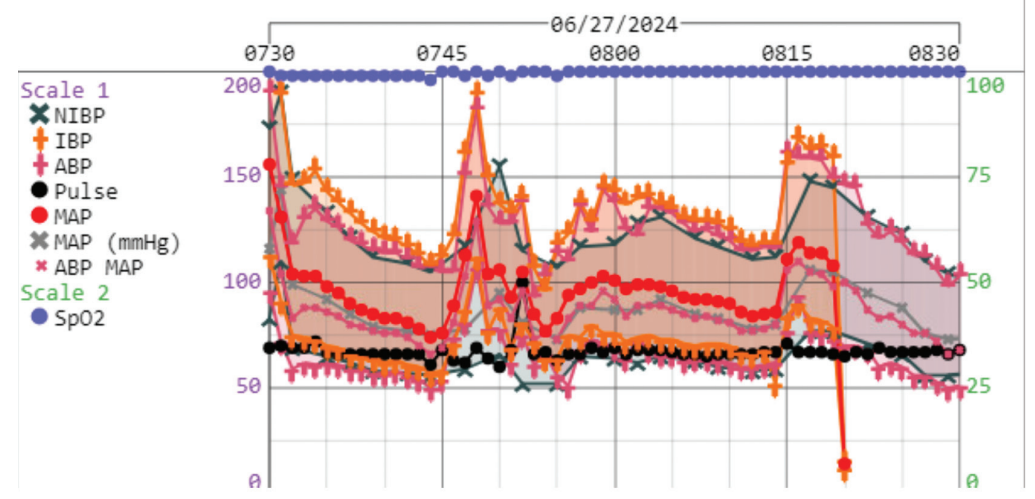
Previous literature shows precision and linear correlation between noninvasive and invasive blood pressure methods.3 For the first month, both methods were utilized simultaneously, with waveforms compared in each case by the team. The Figure shows a sample waveform comparison obtained during the pilot; the noninvasive data points are less than 5 mm of the invasive arterial blood pressure. This concurrent use of monitoring and comparison of waveforms during the pilot increased the interdisciplinary team comfort and transition to the change. After the first month of the pilot using this new technology concurrent with invasive monitoring, the team proceeded with transitioning to solely noninvasive blood pressure monitoring for select ablations and LAAO procedures.
Baseline data was obtained from April-May 2024 for comparison. The pilot began in June 2024 and data collection continued through August 2024. An independent sample t-test comparing total procedure time (in minutes) did not change from baseline (n= 57), (M=114.93, SD=32.89) to pilot period (n=65) (M=115.69, SD=39.99; t (120) = -0.11, P = .34). Similarly, the periprocedural time (in minutes) remained unchanged between times (baseline: M=32.98, SD=15.12, pilot: M=32.46, SD= 12.47; t (120) = 0.21, P = .84). Further, separating cases between baseline and pilot period by type (ablation and LAAO) did not show any differences. However, for the 14 baseline data cases that utilized a radial approach for anesthesia arterial access site, there was an average time saved of 34 minutes per case. This time savings can be attributed to patients with the noninvasive monitoring in the pilot not requiring an arterial line placement, thereby removing the periprocedural time waiting for arterial line placement prior to procedure start. Access site complications between groups were assessed for safety. The baseline group had 2 cases with ecchymosis and 1 with shadowing, while there were no cases with access site complications noted during the pilot period. No other complications were noted in cases from either group. Of note, pulsed field ablation (pulmonary vein isolation technology) was implemented at the same time, but no impacts were observed.
Despite projected time and workflow efficiencies, the EHR data did not show numeric changes in process procedural metrics between baseline and pilot groups. While the team verbally reported improvements in workflow efficiency, the EHR may not fully capture change due to data entry documentation processes. However, from a clinical perspective, noninvasive monitoring still showed multiple benefits. First, patients experienced decreased risk associated with invasive line placement and recovery time. There was also a decrease in medical supply material waste due to invasive monitoring requiring an arterial line kit, pressure line, and normal saline. Notably, this pilot resulted in savings of normal saline, which proved critical due to a hurricane impacting the national supply of normal saline in Fall 2024.6 At the start of the pilot, normal saline supply was not a concern; however, the unintended conservation of medical supplies in the pilot was beneficial to the department and organization, especially since much of the normal saline in these cases is hung but not fully utilized.
Overall anecdotal feedback from staff was positive, reporting that they found the new technology easy to use and intuitive. The ease of use helped staff embrace the practice change. While not captured in this project, there is further opportunity to determine how this clinical practice change affects patient experience, case volume, and capacity, or whether it impacts other workflow within EP labs.
Patient safety, interdisciplinary teamwork, and workflow efficiency are integral to the success of high-volume EP procedural areas. The quality improvement project at our quaternary medical center focused on evaluating the use of noninvasive blood pressure monitoring compared to invasive monitoring during ablations and LAAO procedures. Despite the lack of numeric changes in procedural metrics, this project highlighted several benefits of noninvasive monitoring, including reduced patient risks, ease of use, and positive staff feedback. These findings suggest that while the transition to noninvasive monitoring may not immediately reflect in procedural time metrics, it offers advantages in patient safety, material waste, and overall EP lab workflow efficiency. As we continue to use this technology, further evaluation could contribute to improved clinical outcomes and operational performance in EP labs.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest, and report no conflicts of interest regarding the content herein.
References
1. Eltelbany M, Fabbri M, Batchelor WB, et al. Best practices for vascular arterial access and closure: a contemporary guide for the cardiac catheterization laboratory. Front Cardiovasc Med. 2024;11:1349480. doi:10.3389/fcvm.2024.1349480
2. Echeverri D, Pizano A, Cabrales J, et al. Validation of central and peripheral non-invasive hemodynamic variables using an oscillometric method. High Blood Press Cardiovasc Prev. 2018;25(1):65-77. doi:10.1007/s40292-017-0238-8
3. Maggi R, Viscardi V, Furukawa T, Brignole M. Non-invasive continuous blood pressure monitoring of tachycardic episodes during interventional electrophysiology. Europace. 2010;12(11):1616-1622. doi:10.1093/europace/euq333
4. 510(k) Premarket Notification. Acumen Hypotension Prediction Index. U.S. Food and Drug Administration. Published December 9, 2024. Accessed December 11, 2024. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPMN/pmn.cfm?ID=K203224
5. Critical insights: noninvasive continuous blood pressure monitoring. Edwards Lifesciences Clinical Education. Published August 17, 2023. Accessed May 5, 2024. https://youtu.be/sPPlVJGQGnk
6. American Medical Association. IV shortage update: Baxter facility damage after hurricane in North Carolina 2024. Published October 23, 2024. Accessed May 5, 2024. https://www.ama-assn.org/delivering-care/public-health/iv-shortage-update-baxter-facility-damage-after-hurricane-north

