Atherectomy + DCB vs Stent-Based Repair for Severely Calcified Femoropopliteal Disease
Nagoya Heart Center, Japan
As part of Wednesday’s afternoon session on Drug Elution Technology in CLTI, interventional cardiologist Dr. Takahiro Tokuda, from Nagoya Heart Center in Japan, outlined new evidence comparing 2 contemporary revascularization options for heavily calcified femoropopliteal lesions: (1) rotational atherectomy followed by a drug-coated balloon (DCB) and (2) implantation of current-generation stents. His talk summarized the multicenter CORVUS study, a retrospective observational analysis spanning 8 Japanese institutions, designed to clarify which strategy best balances patency, safety, and limb preservation in this challenging anatomy.
CORVUS enrolled 121 lesions treated with atherectomy + DCB and 467 lesions treated with stents. A rigorous propensity-score match produced 2 well-balanced cohorts of 82 patients each, equalized for age, Rutherford class, comorbidities, lesion length, runoff status, intravascular ultrasound use, and adjunctive ballooning techniques. Follow-up was set at 12 months.
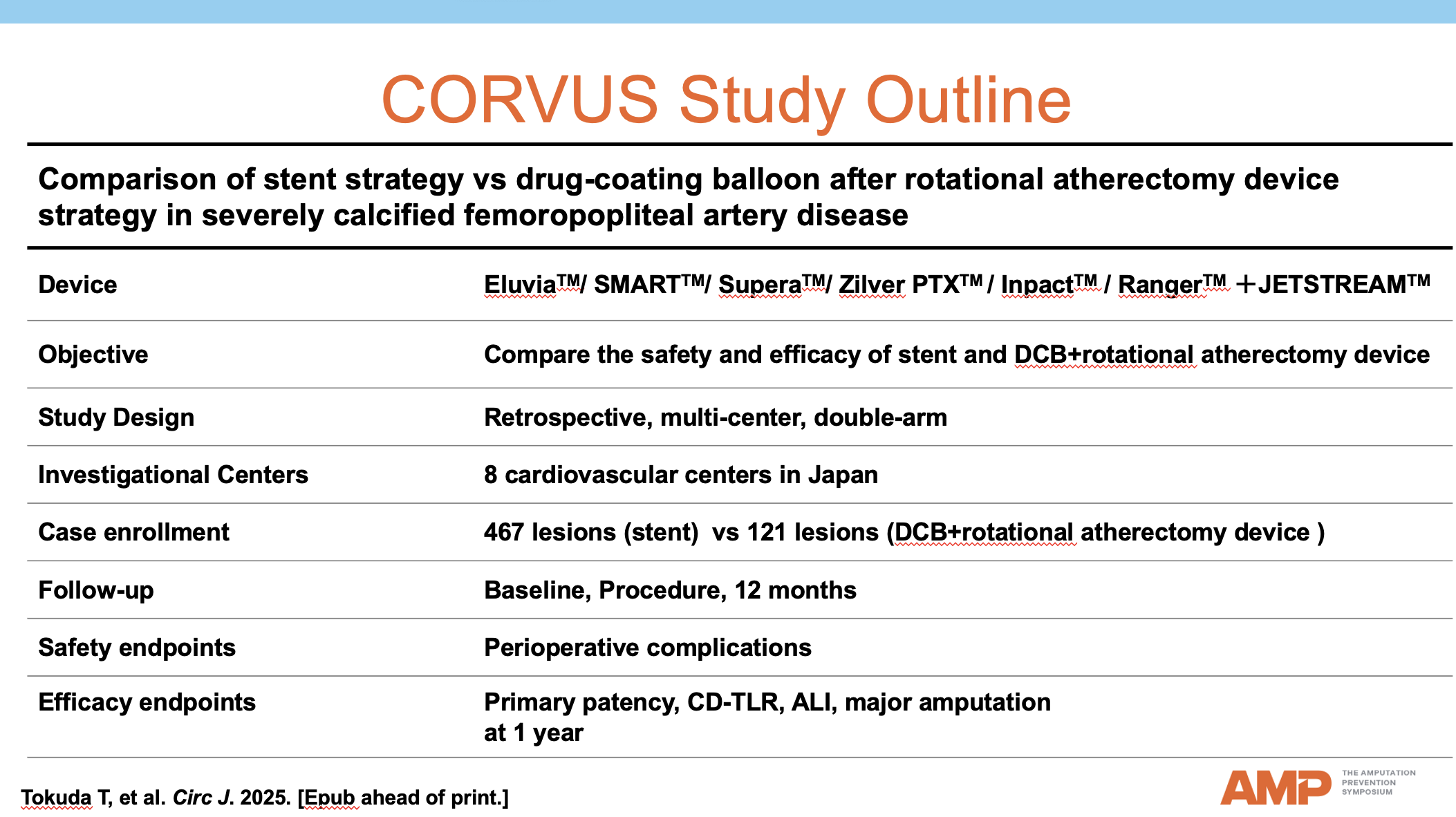
At 1 year, the matched analysis demonstrated statistical parity between the 2 strategies: primary patency, logrank P = 0.76; freedom from clinically driven target-lesion revascularization (CD-TLR), logrank P = 0.68; acute limb ischemia, logrank P = 0.31; and major amputation, logrank P = 0.88. No baseline characteristic, including diabetes, dialysis, or lesion length, modified the relationship between treatment type and restenosis risk.
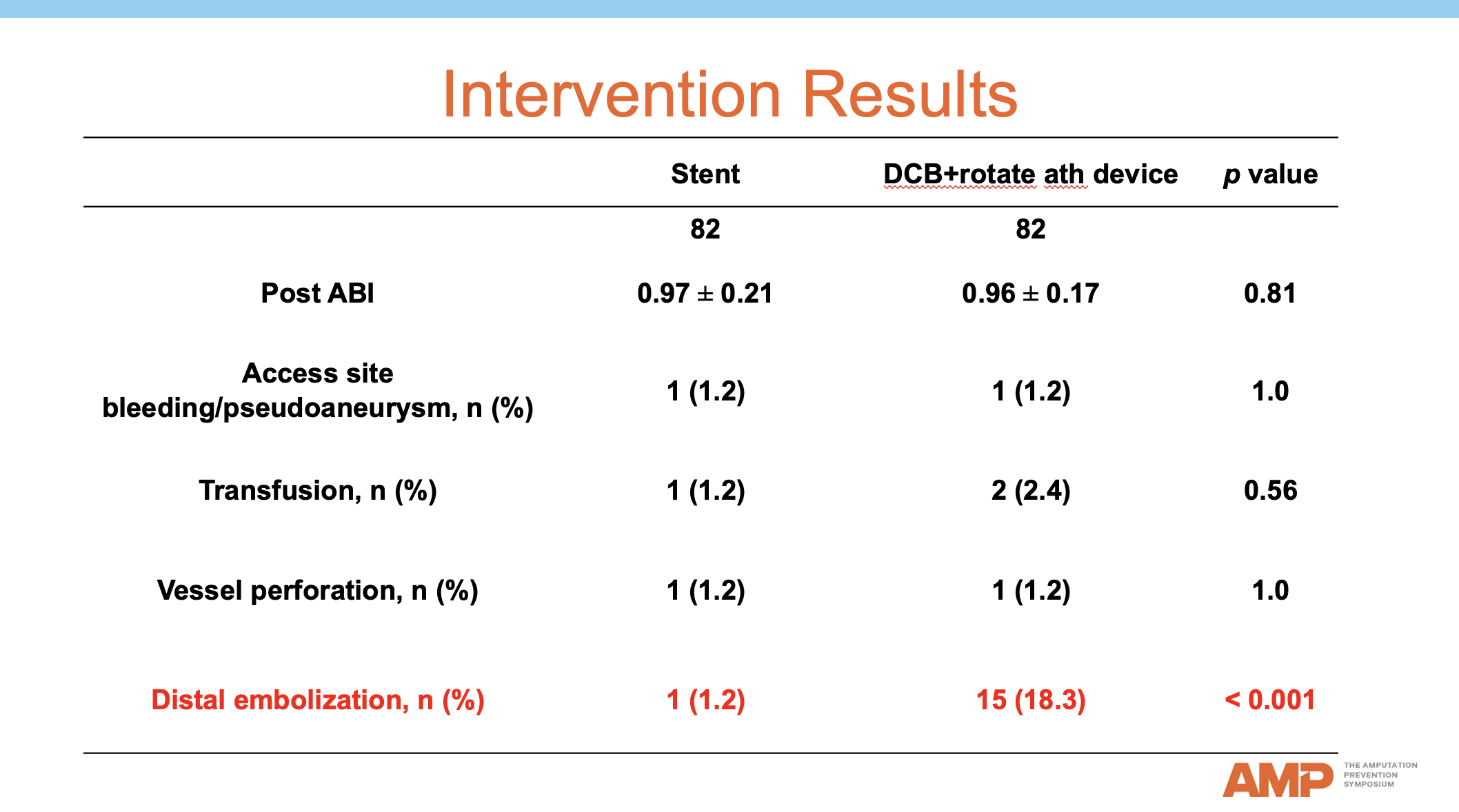
While efficacy was comparable, distal embolization occurred more often after atherectomy, mirroring real-world registry rates of 5.8% to 9.7% (JSUPREME-1, JSUPREME-2, PMS datasets). Conversely, modern stents continue to improve: Japanese data suggest severe calcification no longer predicts restenosis when current devices are used properly, and polymer-coated paclitaxel-eluting stents outperform polymer-free alternatives, although patency at 5 years is only 65%.
Dr. Tokuda’s presentation positions atherectomy + DCB as a credible alternative to stent-based therapy for severely calcified femoropopliteal lesions. At 1 year, both approaches yield comparable patency, repeat-procedure freedom, and limb-salvage outcomes; the principal tradeoff is a higher but clinically acceptable rate of distal embolization with atherectomy. These findings give interventionalists greater flexibility when tailoring treatment to patients with calcified femoropopliteal disease.