


Cross-Sectional Imaging is Reshaping CLTI Care

Houston Methodist DeBakey Heart & Vascular Center, Texas
In a Thursday morning session, vascular surgeon Trisha Roy, MD, PhD, FACS, from Houston Methodist DeBakey Heart & Vascular Center, outlined why modern cross-sectional imaging performed before peripheral vascular intervention can be the difference between limb salvage and treatment failure in patients with CLTI. Her central message was that modern imaging technology not only improves procedural planning but also reduces complications, boosts success rates, and protects renal function.
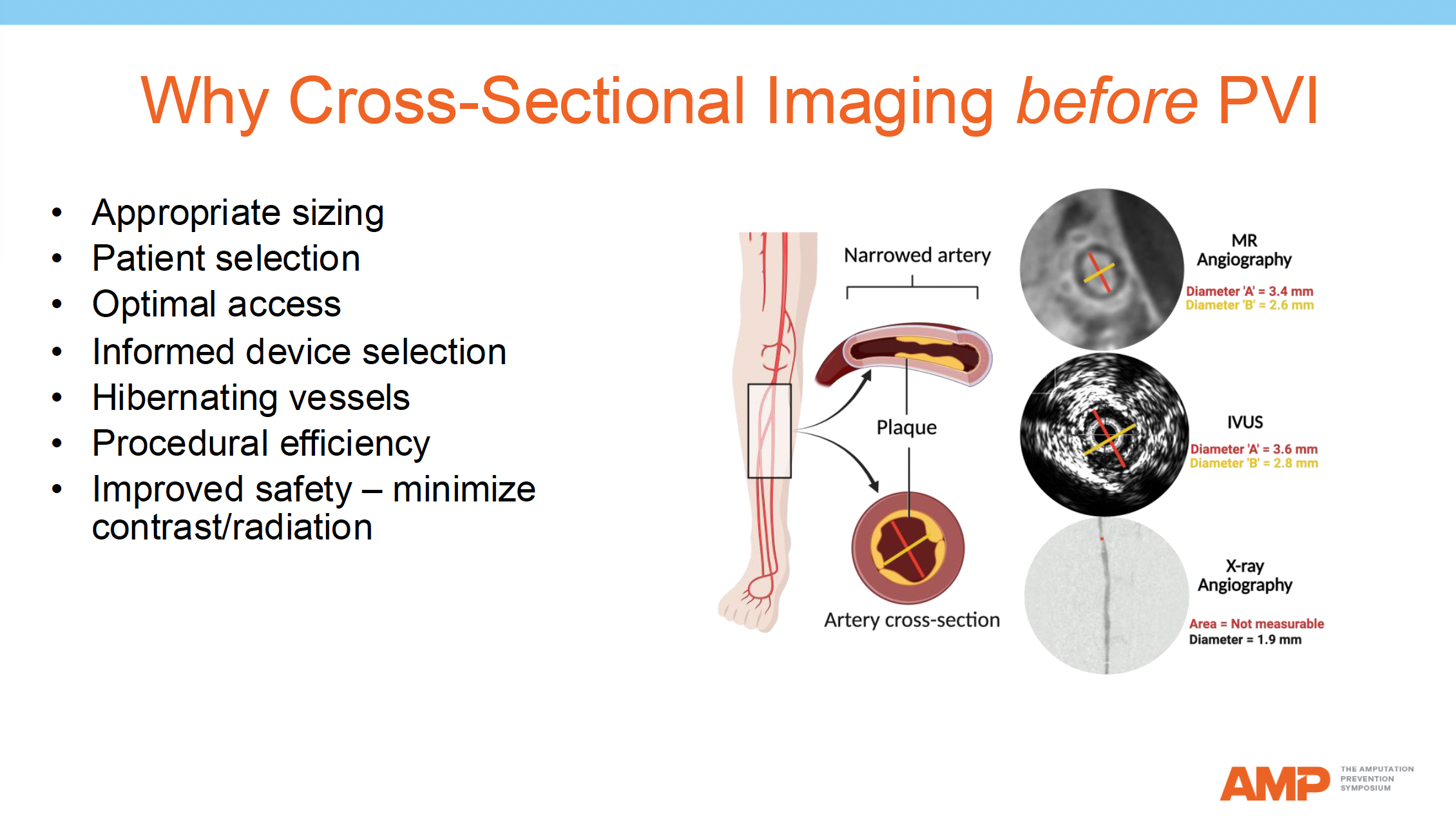
Dr. Roy emphasized that imaging prior to intervention allows clinicians to properly size vessels, select the right patients, identify optimal access points, choose devices more accurately, detect hibernating vessels, enhance procedural efficiency, and minimize both contrast exposure and radiation risk. She discussed how imaging modalities such as magnetic resonance angiography and intravascular ultrasound provide different and often more accurate vessel diameter measurements compared with traditional X-ray angiography.
Dr. Roy then addressed 5 misconceptions that have historically limited imaging use:
1. “MRI doesn’t see calcium”: Using ultrashort echo time magnetic resonance imaging (MRI), Dr. Roy demonstrated that both calcified and noncalcified plaques can be visualized with precision, enabling clinicians to detect “hard” chronic total occlusions that might otherwise resist conventional wire passage during endovascular procedures.
2. “CTA is useless for below-the-knee vessels”: Photon-counting CT (PC-CT) was highlighted as a major advancement, offering 0.25 mm resolution that can clearly show 2–3 mm tibial arteries. With submillimeter sizing accuracy, calcium subtraction algorithms, and rapid single-helical scanning in under 7 minutes using only 40–60 mL of contrast, PC-CT is redefining the role of computed tomography angiography (CTA) in CLTI.
3. “It’s unsafe for renal patients”: Dr. Roy reviewed QISS MRA, a noncontrast MRI technique ideal for renal-impaired patients. In a study of 570 vessels across 41 patients, QISS MRA detected 66% patent below-the-knee segments, outperforming digital subtraction angiography.
4. “It takes too long and is too expensive”: Dr. Roy countered this by illustrating that imaging is a cost-effective investment compared with the risks of failed interventions. She also noted that 20% of endovascular procedures still fail technically, a rate unchanged for nearly 2 decades across multiple landmark trials (BASIL, BEST-CLI, BASIL-2).
5. “I don’t need it, my patients do awesome”: Dr. Roy challenged this by presenting data showing high readmission rates for unplanned revascularization or amputation post-discharge in CLTI patients. She presented histopathology slides of uncontrolled dissections, distal embolization, and calcium nodule disruption, all of which could have been predicted or avoided with proper imaging.

To unify practice across centers and reduce missed opportunities for limb salvage, Dr. Roy proposed an “MRI-first” strategy, particularly for renal-impaired patients. This approach allows plaque-level visualization without contrast, better identification of tibial targets, and a reduction in renal injury risk.
In conclusion, Dr Roy encouraged vascular teams to validate and implement a pragmatic, renal-safe imaging algorithm by 2025 by emphasizing that we “can’t fix what we can’t see”.
