


The Role of Ultrasound in Identifying and Treating Complications

AMize Consulting Services LLC, Grand Rapids, Michigan
During Friday morning’s “Complications Happen: Deal With It” session, Abigail Mize, BS, RDCS, RVT, from AMize Consulting Services LLC in Grand Rapids, Michigan, gave a presentation entitled "Utilization of Ultrasound to Identify and Treat Complications." She emphasized that while prevention remains the best strategy, complications can arise even with the most skilled operators.
Ms Mize began by reaffirming that avoidance is the most effective prevention strategy. She outlined best practices, including ultrasound-guided access and closure, in-room hemostasis confirmation, and prompt re-evaluation at the first sign of changes. However, she acknowledged that complications could occur despite meticulous technique, positioning ultrasound as an indispensable tool for real-time detection and assessment both intra- and post-operatively.
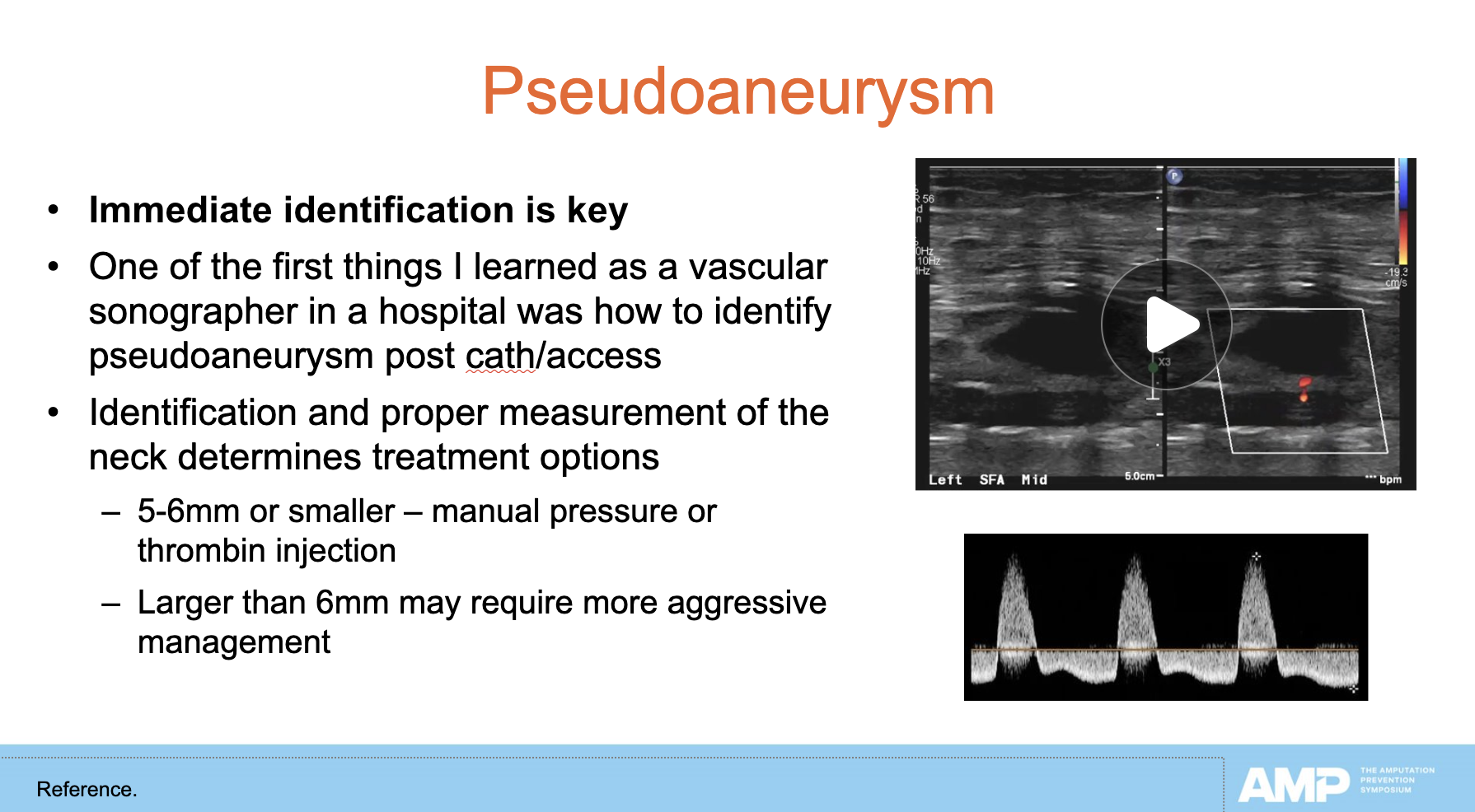
Ultrasound’s ability to rapidly identify issues such as pseudoaneurysms, perforations, ruptures, hematomas, flow-limiting dissections, and distal embolizations was central to Ms Mize’s discussion. She highlighted how sonographic imaging can distinguish between active bleeding sources, such as pseudoaneurysm rupture, and less urgent issues such as track oozing. Importantly, ultrasound can monitor intraprocedural perforations or hematomas for changes over time and re-evaluate vessels in cases of acute re-occlusion.
Ms Mize emphasized that using ultrasound during closure device deployment ensures the device is placed without compromising the vessel and allows for immediate confirmation of successful hemostasis. This proactive approach reduces the risk of missed complications and facilitates prompt intervention when needed.
She presented a case involving an older adult patient who presented at follow-up with a noticeable thigh lump but no pain or discomfort. Ultrasound imaging revealed stent migration with possible vessel rupture, and the patient was taken immediately to the catheterization lab, where angiography confirmed stent separation and a large extravascular flow pocket consistent with rupture or aneurysm. Given her age, a covered stent was chosen as the treatment approach. Ultrasound guided the wire through the aneurysmal area, assisted during covered stent deployment, and confirmed the end of abnormal flow post-procedure.
Ms Mize concluded by urging clinicians to think creatively about ultrasound’s applications, noting that its value extends far beyond initial diagnostics and vascular access. “The more you use it,” she said, “the more versatile it becomes.”
