


The Radial Lounge, Revisited


The MedStar Union Memorial Hospital located in Baltimore, Maryland, is the cardiovascular hub for the MedStar Health system in its north region. We perform approximately 1,200 percutaneous coronary interventions (PCI), 150 transcatheter aortic valve replacements (TAVRs), and 30 WATCHMAN (Boston Scientific) procedures per year. Additionally, we have a full complement of structural heart procedures, including atrial septal defect and patent foramen ovale closure, percutaneous transvenous mitral commissurotomy, and alcohol septal ablation. We began our transradial program in 2010, at which point, the adoption rate was <10%. The landscape of our cardiac catheterization lab has changed significantly since that time. We have moved to a small group of hospital-employed interventional cardiologists that handle the vast majority of volume for the entire north system. This has allowed the lab to evolve more rapidly than it would have in previous iterations, with like-minded operators advancing new initiatives. By early 2017, the overall transradial rate for all-comers improved to nearly 90%. We saw this translate directly to significant improvements in our National Cardiovascular Data Registry (NCDR) outcomes. The next logical move was to start same-day discharge for select PCIs. Our initial criteria for same-day discharge was admittedly strict, but this would evolve as well, with continued experience. We soon realized we could improve the patient experience and contain healthcare costs simultaneously, and the decision was made to explore building a dedicated radial lounge.


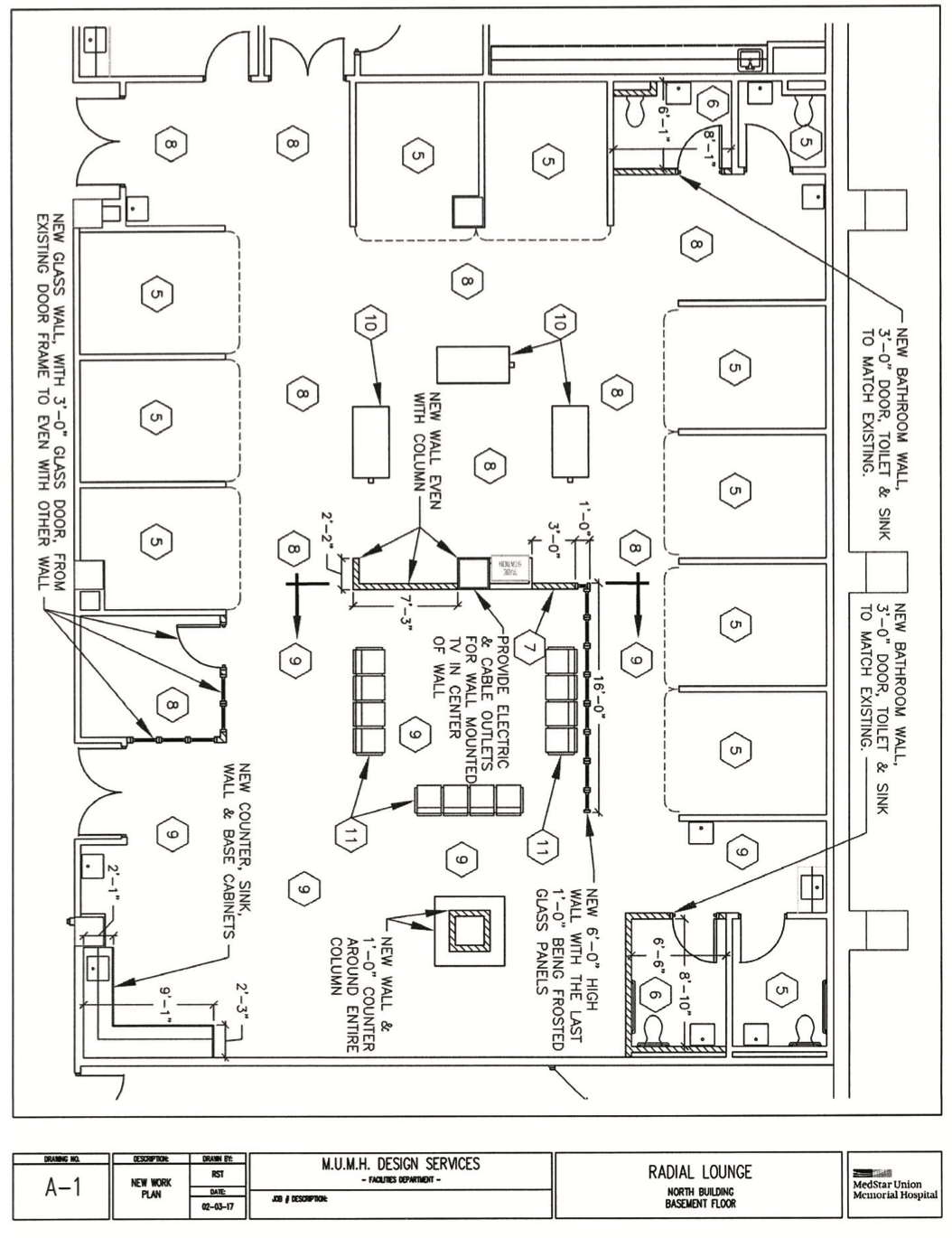
Our traditional 29-bed cardiovascular prep and recovery unit is adjacent to the catheterization lab and is open 24/7 for all cardiac, vascular, electrophysiology (EP), and interventional radiology (IR) patients. Early in the planning phases, we visited an existing radial lounge in Atlanta, Georgia, for design ideas. We felt there were a few “must-haves”; namely, that this space must be separate and dedicated for transradial cardiac cath lab patients. It needed to be as similar in feel to an “airport sky lounge” while still retaining the ability to function as a true recovery area, albeit without beds or stretchers. This would include having appropriate monitoring of all patients with wireless telemetry, a code cart, and a medication administration system (Pyxis) all discreetly placed and incorporated into the lounge. The existing observation unit attached to the lab area was relocated to a different part of the hospital and construction on the radial lounge began. After much discussion, we decided on 8 bays, a full cafe area, plenty of seating for family, and private consultation room where films can be reviewed with patients.
We officially opened our 3,400-square-foot radial discharge lounge in September 2017. We currently have it staffed with 2 nurses and 1 technologist. One nurse practitioner (NP) or physician assistant (PA) from our traditional recovery area is assigned to the radial lounge daily. Hours are from 7 am to 7 pm. Any diagnostic cath completed before 4 pm that is being discharged home that day is sent to the radial lounge post procedure. Patients spend approximately one hour in a recliner in their assigned private bay while on telemetry. They then change back into their street clothes with their TR Band (Terumo) in place and spend the remaining time in the cafe or TV area with their family while off telemetry. PCIs suitable for same-day discharge that are completed prior to 1 pm are also sent to the radial lounge post procedure. The recovery protocol is similar, except these patients require 6 hours total of recovery time and remain on telemetry the entire time.

We hope that by outlining our roadmap to achieving a successful radial lounge with a robust transradial catheterization program that other cath labs can learn from both our success and avoid potential pitfalls along the way. The single most important tenet prior to opening a radial lounge is first having adequate transradial volume to support its ongoing use. We did not believe in the concept of “if you build it, they will come.” Instead, we pushed our transradial rates to over 80% of all-comers prior to breaking ground on our radial lounge. The radial lounge should be the final cherry on top of a successful transradial program. We have multiple reasons for this rationale. Dedicated space in the hospital is prime real estate, but it is imperative that the space is both a separate area and protected from use by other service lines. This is important for preserving the patient experience of the “airport sky lounge” and to protect it from being used as just another recovery unit for femoral cases. In terms of patient satisfaction, we have found that the patient education room with a film viewer has been a huge draw for both patients and their families, some of whom have had prior procedures and never had such an opportunity to review their films. Our initial vision of the patient flow through the lounge was that each patient would rotate through every area, spending some time in the recovery bay, transitioning to the cafe, moving to the TV lounge area, and using the patient education room. What we actually learned from real-world experience is that just like in an airport sky lounge where every area is not interacted with by every traveler, patients are the same way. They use parts of the radial lounge in the way they see fit. Some patients desire to just stay within the confines of the recovery bay, while others enjoy sitting with their families in the cafe. We encourage them to relax and enjoy any or all of the spaces, which can de-stress an otherwise potentially stressful situation.
From a physician standpoint, we have found that having a radial lounge and same-day PCI discharge program allows our physicians and physician extenders to perform today’s work today. Patients who underwent PCI that were routinely kept overnight would then require additional rounds the following morning, which are no longer required with same-day PCI discharge. This frees up additional resources to improve cath lab flow. Additionally, by sending a patient to the radial lounge post procedure, it opens up another bed in our traditional recovery unit, which can be used to accept additional transfers.
As far as our same-day discharge criteria, this has continued to evolve with the opening of our radial discharge lounge. First and foremost is patient safety when considering a same-day PCI discharge. Many facilities have strict same-day discharge criteria, which are necessary when patients recover in a traditional cardiac catheterization recovery unit. These patients are usually assessed by a mid-level practitioner and if they meet all of the ‘same-day discharge criteria’, they are discharged home. What we found was that most same-day discharge criteria were somewhat arbitrary (e.g., age cut-offs and angiographic subsets such as bifurcation lesions, etc.) and were not relevant to the modern era of PCI performed transradially. Therefore, we have taken an approach where we assess each patient on the table as soon as we are done with their PCI for suitability for same-day discharge. If we agree that they are a reasonable candidate based on clinical presentation, final angiographic result, and social support situation, then we send them to the radial lounge with the plan of discharge later that day. If the patient’s clinical situation changes, they can be transferred back to the traditional recovery unit and even be admitted if necessary. We find that this real-time decision made by the interventional cardiologist that incorporates the whole clinical picture immediately after the PCI is the best approach.
Lastly, we would like to justify the cost of undertaking such an endeavor, as it is an area of significant importance to hospital administrators. A recent study by Amin and colleagues showed that in a center performing 1,000 PCIs, there is a cost savings of one million dollars annually if 30% of PCI cases are sent home as same-day PCI discharges.1
From its inception on September 6th through November 15, 2017, a total of 184 patients were sent to our radial lounge and discharged home thereafter. This includes 48 PCIs that qualified for same-day discharge. By early December 2017, we had reached the point where we filled all 8 patient bays simultaneously for the first time. We have continuously learned from other programs and hope the description of our own experience further advances this rapidly growing field.
Reference
- Amin AP, Patterson M, House JA, et al. Costs associated with access site and same-day discharge among Medicare beneficiaries undergoing percutaneous coronary intervention: an evaluation of the current percutaneous coronary intervention care pathways in the United States. J Am Coll Cardiol Intv. 2017; 10: 342-351.
The authors can be contacted via Nauman Siddiqi, MD, at nauman.h.siddiqi@medstar.net.


