


Beyond Angiography: The Power of IVUS + NIRS in PCI
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
CLD talks with Dhananjay Chatterjee, MD
UCLA Health, Los Angeles, California
You are a big advocate for intravascular ultrasound (IVUS) imaging. Which systems do you have access to and which is your go-to system to use?
 I work across multiple facilities, and we have access to the Makoto™ Intravascular Imaging System from Nipro Medical, which combines IVUS and near-infrared spectroscopy (NIRS), as well as IVUS platforms from Boston Scientific and Philips, in addition to optical coherence tomography (OCT) from Abbott. I would say my workhorse intravascular imaging catheter is the DualPro because it combines high-definition IVUS with near-infrared spectroscopy. Beyond providing very high image quality, the NIRS component gives you a better sense of tissue characterization, which helps identify lipid-rich plaque and vulnerable plaque.
I work across multiple facilities, and we have access to the Makoto™ Intravascular Imaging System from Nipro Medical, which combines IVUS and near-infrared spectroscopy (NIRS), as well as IVUS platforms from Boston Scientific and Philips, in addition to optical coherence tomography (OCT) from Abbott. I would say my workhorse intravascular imaging catheter is the DualPro because it combines high-definition IVUS with near-infrared spectroscopy. Beyond providing very high image quality, the NIRS component gives you a better sense of tissue characterization, which helps identify lipid-rich plaque and vulnerable plaque.
What are the key features driving your decision in choosing an IVUS system?
There are a couple of factors. First and foremost is image quality. If you want actionable data, it needs to be high-quality data. Good images really help you determine vessel sizing and lesion morphology, choose the appropriate pre-dilation devices, and identify issues with stents, especially in cases of stent failure. In-stent restenosis (ISR) accounts for 10% to 15% of the percutaneous coronary intervention (PCI) cases we treat, so high image quality is essential.
Beyond that, deliverability is very important. If you cannot deliver the catheter, you cannot get the images, and the data are no longer actionable. People also talk a lot about ease of setup, but I think that has become less important over time. In a lab that does a high volume of intravascular imaging-guided PCI, the staff become very comfortable setting up IVUS for every case, so it usually adds very little time, whether it is a plug-and-play system or one that requires a sterile cover over the controller. To me, image quality and deliverability are the most important considerations.
How does image quality impact decision- making in the treatment of complex lesions (including calcified lesions, bifurcations, or long lesions)?
Image quality is essential in the treatment of complex lesions. As intravascular imaging has advanced over the last decade, we have gained a much better understanding of coronary lesion phenotypes that were not well appreciated in the past. Even with calcified lesions, there are many different subtypes to consider, including calcium arc, eccentric versus concentric calcium, and different types of nodules. Eruptive nodules, for example, carry a much worse prognosis than a traditional calcified nodule. High-quality imaging helps you distinguish among these lesion subtypes, and that directly influences the devices you choose.
With very good image quality, including a longitudinal view, you can determine whether a calcified lesion is a short segment and not especially dense, with limited image dropout behind it. In that setting, you may choose a lower-cost tool to pre-dilate the lesion and proceed with PCI. On the other hand, if the imaging shows dense, bulky calcification over a long segment, you may need a more aggressive approach, such as atherectomy or intravascular lithotripsy (IVL). High-quality imaging gives you a much clearer understanding of lesion morphology, which has a major impact on how you approach the intervention and the outcome you can achieve for the patient.
Do you have challenges with delivering catheters? How has your current solution improved the experience?
Catheter delivery can be challenging in complex disease and we are seeing that more often, with some estimates suggesting that more than 30% of PCIs are performed in severely calcified lesions. That said, most high-definition IVUS catheters today are well designed, with hydrophilic coating, good flexibility, and generally good deliverability. In long-segment disease, ISR, and heavily calcified lesions, though, delivery can still be challenging at times.
In those cases, pre-dilating the lesion is often helpful. For more complex interventions, I will often use a 7 French system, which can improve support. A support wire can help, and in some cases advancing a guide extension catheter and then delivering a 6 French IVUS system to the lesion can also be effective. The most difficult anatomy for IVUS delivery is usually a highly retroflexed circumflex artery, especially with ostial calcification, or an extremely tortuous right coronary artery. In a small number of cases, it is simply not physically possible to deliver the catheter, even without much obstructive disease, because there are too many bends. Those cases are relatively uncommon, though. While using the Makoto™, the DualPro catheter delivers even in complex anatomy.
What are the benefits of identifying disease beyond angiography? How are you currently doing this?
Angiography is the most rudimentary tool we have to identify disease. It is really luminography, so it tells us the size of the lumen available for blood flow, but it does not tell us much about plaque burden or lesion morphology. That is especially true in the United States, where patients often have larger body habitus and angiographic resolution may not clearly show whether severe calcification is present. Intravascular imaging gives us much better insight into true vessel sizing and plaque morphology, and it helps us determine whether a calcified lesion needs to be modified before stenting.
Historically, PCI outcomes in calcified vessels were quite poor. A 2014 meta-analysis by Bourantas et al, for example, showed target vessel failure rates of 15% at one year and 23% at three years for severely calcified lesions.1
With modern tools, those rates have come down substantially. Having that additional set of eyes inside the vessel helps us identify higher-risk disease that may not be apparent on angiography alone. It allows us to treat those lesions more effectively up front, rather than leaving ourselves with stent regret and the patient with recurrent interventions over time.
Can you give us an example of disease missed by angiography?
This actually came up for me a handful of times over the last couple of weeks. I had patients present with non-ST elevation myocardial infarction (NSTEMI) and a hazy, moderate-looking lesion where angiography alone did not clearly identify the culprit. In two recent cases, both involving the circumflex, intravascular imaging made the difference. One patient had two moderate lesions, one in the mid left anterior descending (LAD) coronary artery and one in the proximal circumflex artery. I performed IVUS on both. The LAD showed fibrocalcific plaque with a lipid core burden index (LCBI) of zero, which suggested a chronic lesion. Angiographically, the circumflex looked like maybe a 50% to 60% stenosis, but on IVUS/NIRS I could see positive remodeling in that segment, plaque burden of more than 80%, and evidence of plaque rupture within lipid-rich plaque with some thrombus (Figure 1).
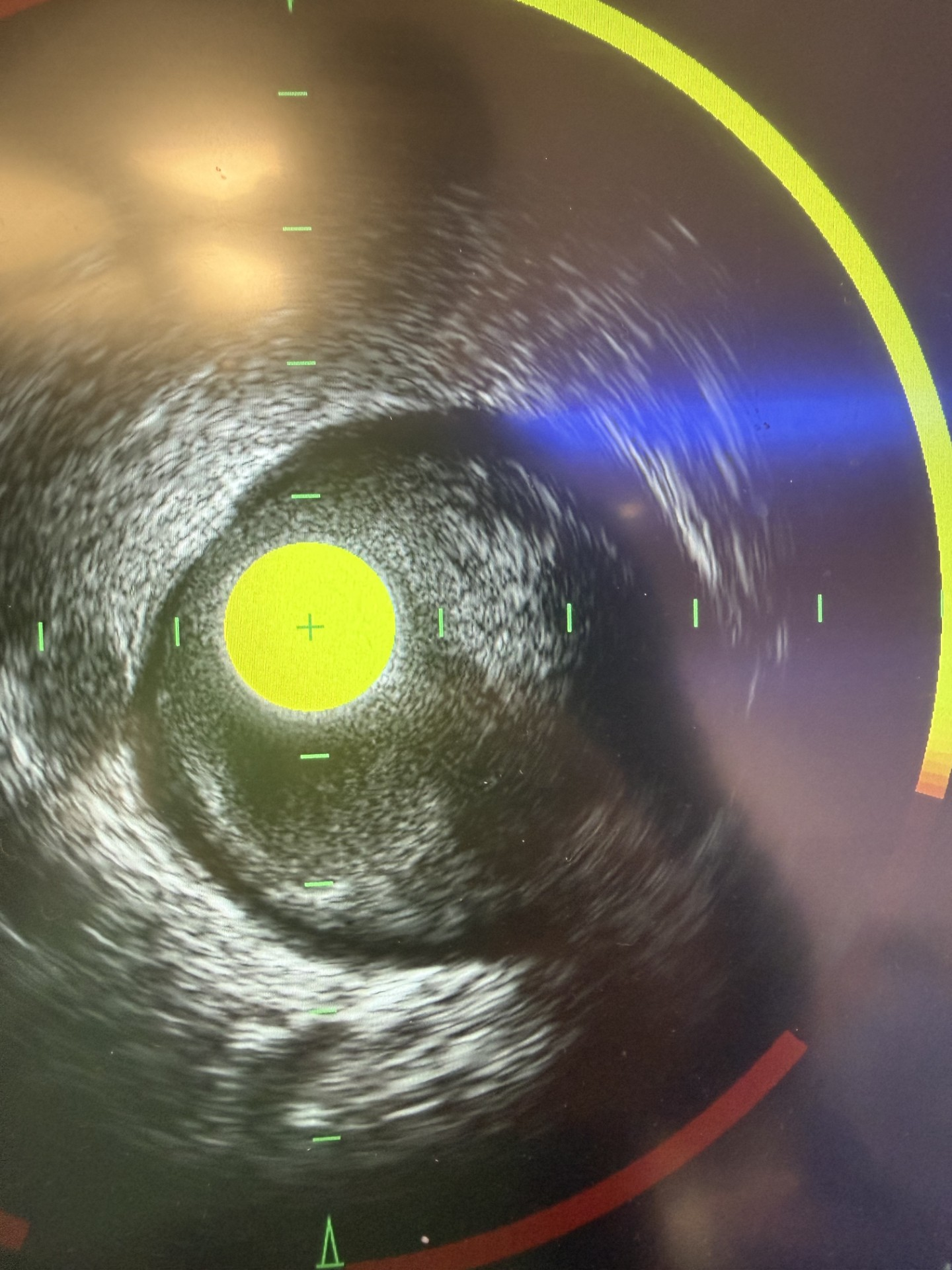
I intervened, and the patient felt much better afterward. The second case involved a proximal circumflex with mixed calcific and lipid-rich plaque which was identifiable by NIRS (Figure 2). The calcific plaque was disrupted, leading to the acute MI. Cases like that really show how intravascular imaging can completely change your treatment paradigm, especially with angiographically hazy or ambiguous lesions. With angiography alone, you might lean toward medical management or conclude this is an MI with non-obstructive coronary disease, when in fact, you may be missing a culprit lesion.
![Chatterjee Figure 2. Additional image for a separate proximal LCx lesion with evidence of plaque rupture within mixed calcific/ vulnerable plaque (as seen by yellow arc on near-infrared spectroscopy [NIRS]).](https://hmp-websites.s3.amazonaws.com/hmp_ln/inline-images/Chatterjee%20Figure%202.png)
How does identifying non-culprit lesions impact your treatment strategy?
This is a question that has come up much more often over the last few years, especially as more work has been done on non-culprit lesion PCI and complete revascularization. In many ways, this concept goes back to surgery. When a patient with multivessel disease undergoes bypass surgery, long-term outcomes are often favorable in part because the non-culprit lesions are addressed as well. In the MI space, multiple trials have now evaluated complete revascularization and treatment of non-culprit lesions. Across several randomized controlled trials in both STEMI and NSTEMI,2-4 there appears to be a benefit to a complete revascularization strategy.
Intravascular imaging can make a meaningful difference in how you approach those lesions. Different strategies have been studied, including physiology-based revascularization and intravascular imaging-guided revascularization. I think intravascular imaging, especially with NIRS, offers an advantage because it not only helps determine whether a lesion has vulnerable plaque and significant plaque burden, but also provides insight into the overall PCI strategy, including vessel sizing, lesion preparation, and stent optimization. So intravascular imaging can help you decide whether to intervene, and it also helps you perform the intervention with more precision.
What is the risk of landing a stent near or within vulnerable plaque?
It has actually been studied. In a sub study from PROSPECT II, investigators looked at patients who developed target vessel failure after PCI in the setting of MI. They found that among patients with target vessel failure, the vast majority had a high plaque burden at the distal stent edge of greater than 50% and a LCBI greater than 108.5 So, in general, landing a stent edge in a diseased segment of the target vessel does appear to increase the risk of target vessel failure, especially when vulnerable plaque is present. Based on the PROSPECT II data, it certainly makes you think twice about accepting that as the final result.
I have also extrapolated that into my own clinical practice. In patients with long-segment disease who may not be surgical candidates, I will sometimes complete an intervention and then notice an angiographic step-down at the distal stent edge after post dilation. I routinely perform post-PCI imaging to assess the distal stent edge and look for areas of underexpansion. In cases where I find a high plaque burden and elevated LCBI at the landing zone, I will sometimes extend the stent if there is a suitable, healthy distal landing zone available. I do that with the understanding that prior studies have shown that landing in a diseased vessel is associated with worse outcomes.
Are there any recent advances in IVUS technology that have helped streamline procedures or improve treatment for your patients?
The elephant in the room is AI, which is now permeating nearly every facet of medicine and daily life. In this setting, I think it has been genuinely helpful. In the cath lab, having AI overlay for IVUS saves time and improves efficiency. There are multiple systems available, but in my practice, AI overlay helps me quickly identify fairly accurate vessel sizing and minimal luminal area immediately after an automatic IVUS pullback.
Instead of manually going frame by frame to look for areas of underexpansion or to make exact measurements of the distal and proximal landing zones, I can rely on the AI in the vast majority of cases. There is more than 95% concordance in my practice with SmartImaging from Makoto™, so it has been a reliable tool in my workflow. It may only save a few minutes, but in high-stress cases, especially complex interventions or acute coronary syndromes cases, those minutes matter. It has made my procedures more efficient and has been a meaningful improvement in day-to-day practice.
What would you say to non-imaging users in light of the recent changes to American College of Cardiology/American Heart Association coronary imaging guidelines?
I do not want to put my peers in the hot seat regarding the 1A recommendation in support of intravascular-imaging guided PCI,6 but I would take a step back and ask why we scrub into cases in the first place. We do this to identify disease, treat it appropriately, and improve outcomes for our patients. The goal is to improve quality of life and provide freedom from major adverse cardiac events and cardiac death. If you look at what has evolved in the cath lab over the last couple of decades, intravascular imaging is one of the most impactful advances we have had.
There are now multiple meta-analyses involving tens of thousands of patients who have undergone intravascular imaging-guided PCI, and they show that imaging does make a difference in outcomes. Sizing is different, lesion preparation is different, post dilation and stent optimization are different, and that translates into larger stent area and better long-term outcomes, including greater freedom from major adverse cardiac events and even cardiac death. Even with some recent trials that have raised questions, the overall body of evidence still supports a clear benefit for intravascular imaging. So to colleagues who remain hesitant, I would say this: ask yourself why you are there in the first place. We are there to take care of patients and achieve the best possible outcomes. Given that, it makes sense to leverage technology that is now very good and can help optimize both workflow and patient outcomes.
This interview is sponsored by Nipro Medical.
References
1. Bourantas CV, Zhang YJ, Garg S, et al. Prognostic implications of coronary calcification in patients with obstructive coronary artery disease treated by percutaneous coronary intervention: a patient-level pooled analysis of 7 contemporary stent trials. Heart. 2014 Aug; 100(15): 1158-1164. doi:10.1136/heartjnl-2013-305180
2. Mehta SR, Wood DA, Storey RF, et al; COMPLETE Trial Steering Committee and Investigators. Complete revascularization with multivessel PCI for myocardial infarction. N Engl J Med. 2019 Oct 10; 381(15): 1411-1421. doi:10.1056/NEJMoa1907775
3. Biscaglia S, Guiducci V, Escaned J, et al; FIRE Trial Investigators. Complete or culprit-only PCI in older patients with myocardial infarction. N Engl J Med. 2023 Sep 7; 389(10): 889-898. doi:10.1056/NEJMoa2300468
4. Diletti R, den Dekker WK, Bennett J, et al; BIOVASC Investigators. Immediate versus staged complete revascularisation in patients presenting with acute coronary syndrome and multivessel coronary disease (BIOVASC): a prospective, open-label, non-inferiority, randomised trial. Lancet. 2023 Apr 8; 401(10383): 1172-1182. doi:10.1016/S0140-6736(23)00351-3
5. Kjøller-Hansen L, Maehara A, Kelbæk H, et al. Impact of lipidic plaque on in-stent and stent edge-related events after PCI in myocardial infarction: A PROSPECT II substudy. Circulation: Cardiovascular Interventions. 2024; 17(10): e014215. doi:10.1161/CIRCINTERVENTIONS.124.014215
6. Rao SV, O’Donoghue ML, Ruel M, et al; Peer Review Committee Members. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2025 Jun 10;85(22):2135-2237. doi:10.1016/j.jacc.2024.11.009

