


Thrombus Burden in ALI and the Role of the Rotarex™ Catheter System
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
CLD talks with:
Jorge Miranda, M.D., RPVI1; M. Laiq Raja, M.D., FACC, FSCAI2
1Director, Limb Salvage Program, Texas Heart Institute; Chief of Vascular Surgery, Ben Taub General Hospital; Assistant Professor at Baylor College of Medicine; Houston, Texas
2El Paso Cardiology; President and Founder, Critical Limb Ischemia Fighters (CLIF) Conference; Founder, Limb Savers Society; Medical Director, Department of Cardiology and Critical Limb Ischemia Program, The Hospitals of Providence, Memorial Campus, El Paso, Texas
I. Dr. Jorge Miranda
Can you tell us about your background and the patients with Peripheral Arterial Disease (PAD) you treat?
 Dr. Miranda: I serve as director of limb salvage and chief of vascular surgery at Baylor College of Medicine in Houston, Texas. I practice in the Baylor St. Luke’s Medical Center in collaboration with the Texas Heart Institute, and approximately 70% of my work is dedicated to limb salvage.
Dr. Miranda: I serve as director of limb salvage and chief of vascular surgery at Baylor College of Medicine in Houston, Texas. I practice in the Baylor St. Luke’s Medical Center in collaboration with the Texas Heart Institute, and approximately 70% of my work is dedicated to limb salvage.
Most of the disease I treat is occlusive and typically multilevel, ranging from iliac and superficial femoral/popliteal disease to tibial and inframalleolar involvement. The majority of my patients present with chronic limb-threatening ischemia (CLTI), including nonhealing wounds, tissue loss, complex limb-threatening presentations that often require staged wound management and, in some cases, foot reconstruction.
How frequently do you encounter thrombotic or mixed disease?
Dr. Miranda: I encounter mixed morphology frequently and it is present more often than many people appreciate. A large portion of my practice involves patients who are three- or four-time redo cases and return with occlusions, including in-stent occlusions or failed prior bypasses, often with tissue loss. Many have been told elsewhere that there are no further options, and that is typically where I take over. In that context, mixed morphology makes up the bulk of what I treat.
When treating acute and subacute limb ischemia, how has the Rotarex™ Catheter System influenced your ability to restore flow, particularly in cases with heavy thrombus or mixed morphology lesions?
Dr. Miranda: The Rotarex™ Catheter System has enabled me to restore flow in acute and subacute limb ischemia. The 6 French (F) Rotarex™ Catheter is compatible with a 6F sheath, which helps limit access size, and it is efficient at clearing thrombus. Many patients present with what looks like subacute ischemia, such as an in-stent occlusion, bypass occlusion, or thrombosis, that is often driven by an acute thrombotic component superimposed on chronic disease. The Rotarex™ Catheter System allows me to address the acute thrombus while helping to minimize embolic risk, which I attribute to the device’s active aspiration.
In acute limb ischemia, recognizing that this is a distinct patient population, I often administer tPA before using the Rotarex™ Catheter System. As the catheter is opened and set up, a process that typically takes about 5-10 minutes, we allow the pretreatment to take effect and then proceed with thrombectomy. I’ve had positive results with this approach, and we are preparing our series on this strategy for publication.
In patients presenting with peripheral arterial in-stent restenosis (ISR), what clinical advantages have you observed when using the Rotarex™ Catheter System?
Dr. Miranda: Right now, in terms of cleared indications, the options for ISR debulking are limited. I favor the Rotarex™ Catheter System because it is a powerful tool with high RPM that can clear material within a stented segment efficiently.
It has a rotating, atraumatic catheter head with blunt facets to modify and detach mixed morphology lesions, while an internal rotating helix simultaneously creates continuous negative pressure at the tip, actively aspirating debris through large side windows as the catheter advances — these are features I find particularly helpful. The device is not actively suctioning until it is activated, so I can advance to the target lesion and then initiate therapy when I am positioned where I want to be. The front portion is rotating to engage and remove thrombus, and the segment immediately behind it helps aspirate. I like that I can see what is being removed. There is real-time visual confirmation through the port, which is important feedback on how effective the passes are. If that visual return drops off, whether because the device is clutching or the thrombus burden is high, I remove the catheter, clear it with heparinized saline, and reinsert to continue. I do not routinely flush the sheath itself. I will intermittently flush the device to clear thrombus within the catheter as I am evacuating material and to prevent overheating. I have found blood loss to be minimal.
Given ongoing cost pressures in PAD programs, how does the ability to address both thrombus and plaque with a single device like the Rotarex™ Catheter System impact overall procedural efficiency and resource utilization within your facility?
Dr. Miranda: This device is simple to assemble, with minimal steps required. Staff training is easier compared with platforms that require more complex preparation or additional specialized components. The system has a small console with catheters that are prepackaged, which is helpful when space is limited.
How does intravascular ultrasound (IVUS) guide your decision making during thrombectomy or atherectomy procedures?
Dr. Miranda: Especially for complex, multilevel reconstructions, IVUS is very important. If you wear glasses, when you wake up, in order to see clearly, the first thing you do is put on your glasses. That’s how IVUS feels when I am doing an intervention. It helps confirm whether my crossing is truly luminal, defines plaque morphology — whether there is mixed material, heavy calcium or soft material — and determines accurate vessel sizing. After I perform thrombectomy or atherectomy, I repeat IVUS to assess whether I have adequately treated the target segment or left residual disease behind.
Angiography is inherently two-dimensional, whereas IVUS provides a three-dimensional vessel assessment that can reduce the need for repeat angiography and associated radiation exposure.
How has the Rotarex™ Catheter System changed your approach to complex PAD, and what does it signal about the future role of peripheral arterial thrombectomy in limb ischemia?
Dr. Miranda: The Rotarex™ Catheter System is my go-to device for managing complex, long-segment, or multilevel PAD, particularly when thrombus is part of the lesion and the case requires a predictable workflow.
A major differentiator is how it can be used from retrograde pedal access. I have found pedal access to be effective in the right patients, especially those with adequate outflow. In my practice, I use the 6F Rotarex™ Catheter from a pedal approach in roughly 50% of my cases. I typically place a 6F Slender sheath (Terumo) and perform thrombectomy retrograde. Coming from below may also reduce embolic risk, and that is one reason I favor this approach when anatomy and outflow allow.
Traditionally, a Rutherford 2B limb, with motor and sensory loss, meant open surgical thrombectomy. More recent experience suggests percutaneous thrombectomy with devices like the Rotarex™ Catheter, can work well in the right patients. I don’t think the data are settled yet, but I do think we are heading toward a shift in where endovascular thrombectomy fits compared with open surgery, and that will likely shape practice patterns and, over time, guideline recommendations.
Case Study: Successful Revascularization of Occluded Iliac Stents Using Rotational Thrombectomy Via Rotarex™ Catheter System
M. Laiq Raja, M.D., FACC, FSCAI
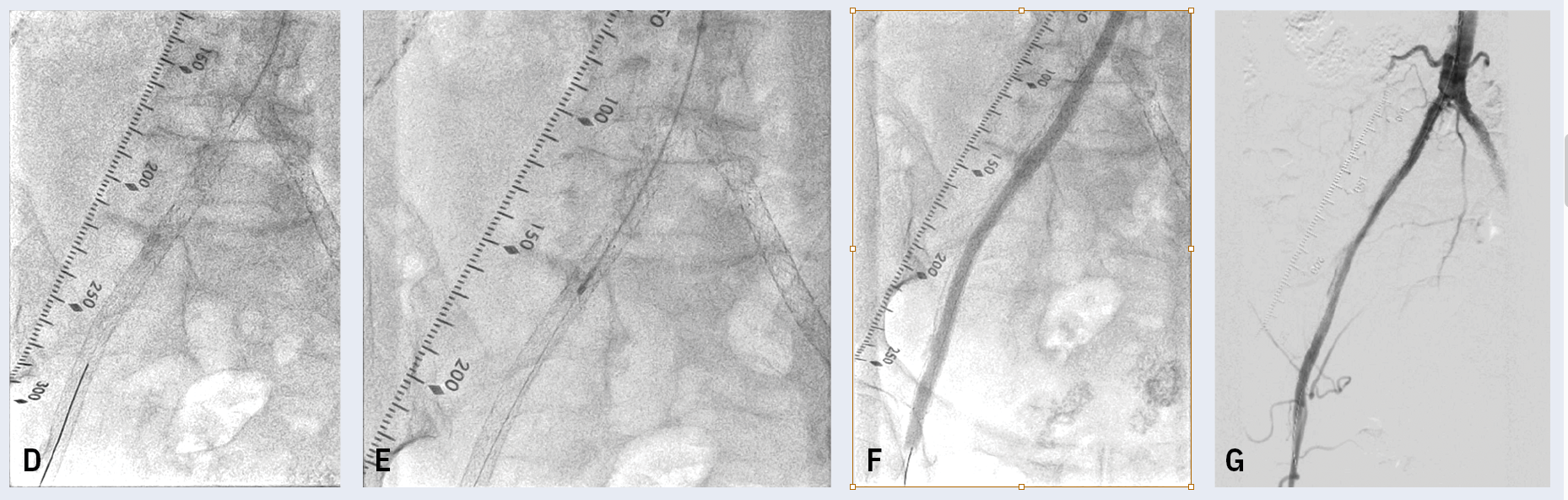
This is a 75-year-old female with a long-standing history of insulin-dependent diabetes, hypertension, coronary artery disease and peripheral vascular disease. A few years ago, the patient had undergone an extensive endovascular revascularization of the bilateral lower extremities. She was found to have an occluded distal aorta also involving the bilateral iliac arteries. The patient underwent successful endovascular revascularization with recanalization of the distal aorta and the bilateral common iliac arteries with placement of stents from the external iliac arteries going into the aorta. She had done fairly well until recently, when she started experiencing significant claudication to the right lower extremity. A noninvasive study showed possible occlusion of the right iliac stents. Angiography confirmed occlusion of the right common iliac and external iliac artery stent going into the aorta. The patient underwent a repeat endovascular procedure. From the brachial access, a long sheath was advanced all the way into the distal aorta. With some difficulty, the occlusion was crossed; subsequently, intravascular ultrasound showed mixed morphology involving subacute thrombus and intimal hyperplasia. At that point, I decided to proceed with the Rotarex™ Catheter System, which has both the qualities of mechanical thrombectomy and atherectomy, followed by percutaneous transluminal angioplasty using a drug-coated balloon. The patient did quite well and was discharged the following day, with instructions to proceed with our critical limb ischemia protocol to maintain optimal perfusion.
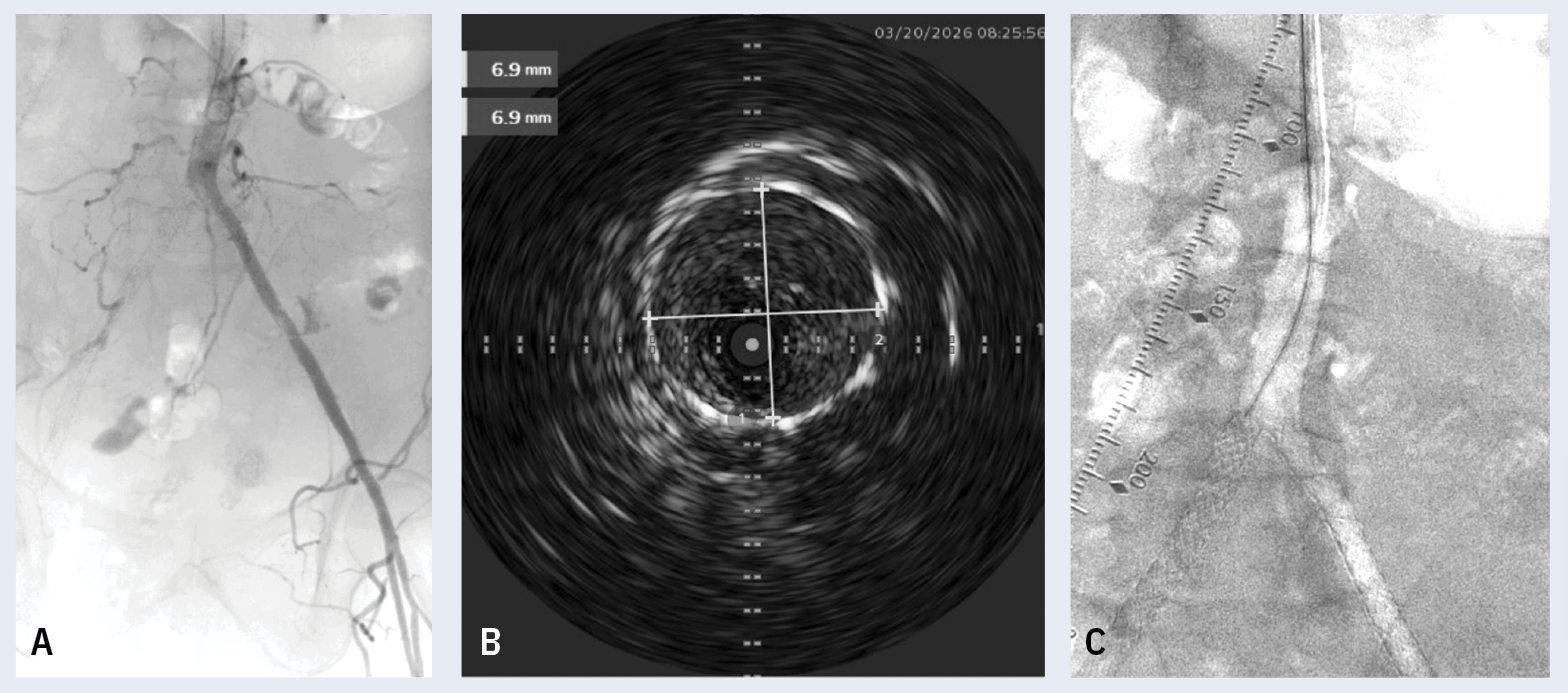
(C) Occluded stents.
II. Dr. M. Laiq Raja
Can you tell us about your background and the patients with PAD you treat?
 Dr. Raja: I am an interventional cardiologist in El Paso, Texas. My practice covers both coronary and peripheral vascular disease, and over time it has shifted to a heavier peripheral focus, with about 60% peripheral interventions and 40% cardiology. In parallel, my team and I have built a critical limb ischemia program that operates under a multidisciplinary model across both the hospital and outpatient settings. The program includes two nurse practitioners and a nurse navigator, and we work closely with podiatry, infectious disease and vascular specialists.
Dr. Raja: I am an interventional cardiologist in El Paso, Texas. My practice covers both coronary and peripheral vascular disease, and over time it has shifted to a heavier peripheral focus, with about 60% peripheral interventions and 40% cardiology. In parallel, my team and I have built a critical limb ischemia program that operates under a multidisciplinary model across both the hospital and outpatient settings. The program includes two nurse practitioners and a nurse navigator, and we work closely with podiatry, infectious disease and vascular specialists.
How frequently do you encounter thrombotic or mixed disease?
Dr. Raja: PAD often has a thrombotic component on top of chronic occlusive disease. If I had to estimate, about 10% to 15% of our patients have a thrombotic presentation, and acute limb ischemia accounts for a large share of the transfers we receive.
When treating acute and subacute limb ischemia, how has the Rotarex™ Catheter System influenced your ability to restore flow, particularly in cases with heavy thrombus or mixed morphology lesions as compared to other therapies?
Dr. Raja: Before this device was available, if a patient presented with extensive clot, I would place long catheters for ultrasound-guided EKOS treatment (Boston Scientific), which requires ICU monitoring with overnight thrombolytic infusion, followed by angiography the next morning. The trade-off is the bleeding risk: compartment syndrome from spontaneous intramuscular bleeding, GI bleeding, and intracranial hemorrhage. That is why a single-session mechanical approach can be so valuable. If you can clear thrombus without exposing the patient to systemic thrombolytics, you reduce the risk of those complications.
Acute thrombotic occlusions often show little to no collateral filling, and you may see a flush occlusion rather than the tapered appearance typical of chronic disease. At times, you can even see clot movement.
For subacute thrombus, my options are typically the Rotarex™ Catheter System or a catheter-directed tPA infusion across the clot. The Rotarex™ Catheter System performs well in both acute and subacute settings and can be used across a long segment — from the common femoral or iliac down to the popliteal — allowing removal of extensive clot in a single setting.
When I use the Rotarex™ Catheter System, I try to reduce the thrombus burden in a controlled way. If thrombus extends from point A to point B with distal reconstitution, I will work the device and stop a couple of centimeters short of point B. I will make several passes to debulk the thrombus first and then address the distal cap once the overall clot burden is much lower. That sequence likely helps reduce the risk of embolization when crossing distally.
I also run saline through the sheath so there is a steady drip that travels with the device as I am clearing thrombus. I will advance to create a small channel, then come back so fluid can track distally. Without constant catheter movement, it will not function as effectively.
In patients presenting with peripheral arterial ISR, what clinical advantages have you observed when using the Rotarex™ Catheter System?
Dr. Raja: The Rotarex™ Catheter System is the only thrombectomy device FDA-cleared for peripheral arterial ISR—an indication also limited among atherectomy devices. I have found the Rotarex™ Catheter System to be effective in ISR and it is my preferred device for these lesions.
Given ongoing cost pressures in PAD programs, how does the ability to address both thrombus and plaque with a single device like the Rotarex™ Catheter System impact overall procedural efficiency and resource utilization within your facility?
Dr. Raja: When using the Rotarex™ Catheter System, treatment is often completed in a single session. After the case, patients are observed overnight mainly for sheath removal and routine monitoring, and most are ready to leave the next day.
How does IVUS guide your decision-making during thrombectomy or atherectomy procedures?
Dr. Raja: IVUS keeps me from guessing. I match the device to the lesion instead of treating blindly. Angiography has real limitations in these cases. You cannot always tell thrombus from plaque, you cannot define calcium the same way, and you are still working from a two-dimensional picture when you are trying to size the vessel and plan treatment. IVUS gives me the details I need, whether it is thrombus versus plaque, soft material versus calcium, and whether I crossed in the true lumen versus subintimal. It also helps with accurate lumen sizing.
From your experience, what makes the Rotarex™ Catheter System your choice for managing complex, long segment or multilevel PAD lesions?
Dr. Raja: I have found the Rotarex™ Catheter System easy to use, and it removes a substantial thrombus burden. In acute and subacute presentations, including ISR, the Rotarex™ Catheter System performs well.
I also like the BD-supplied guidewire that comes packaged with the Rotarex™ Catheter System. It is an atraumatic wire and, in my experience, does not kink easily. I park it distally, keep an eye on it throughout the case, and make sure it is stable and not migrating or causing vessel injury.
For operators managing acute and subacute limb ischemia, the Rotarex™ Catheter System should be one of the options in the toolbox. The more we learn about PAD and the more complicated the disease becomes, the more important it is to have options. The best outcomes come from using the right device for the right situation.
This article is sponsored by Becton, Dickinson and Company.
Disclaimers: This article is sponsored by Becton, Dickinson and Company (BD). Drs. Miranda and Raja are paid consultants of BD. The opinions and clinical experiences presented herein are for informational purposes only. The results from the case study discussed herein may not be predictive for all patients. Individual results may vary depending on a variety of patient specific attributes.
The Rotarex™ Atherectomy System is intended for use as an atherectomy device and to break up and remove thrombus from native peripheral arteries or peripheral arteries fitted with stents, stent grafts or native or artificial bypasses. The Rotarex™ Atherectomy System is contraindicated in patients not suitable for atherectomy/thrombectomy; in the cardiopulmonary, coronary, carotid, cerebral and renal vasculature; in vessels that are undersized for the device used; and in the venous vasculature. Potential adverse events include, but are not limited to: · Embolization, especially distal embolization · Pulmonary embolisms of all degrees of severity · Thrombosis · Re-occlusion · Vessel wall injury · Vessel dissection / perforation / rupture · Perforation as a result of mural calcium being torn out of the vessel wall · Arteriovenous fistula / pseudo-aneurysm · Hematoma, bleeding, hemorrhage · Organ perforation · Implants such as stents / stent grafts / bypass grafts getting damaged, caught or dislodged · Disruption of the catheter: debris remaining in the body · Allergic reactions, including allergic reactions to device components · Infections or necrosis at the puncture site · Catheter-induced sepsis · Death. Please consult respective product labels and instructions for use for indications, contraindications, hazards, warnings and precautions.
BD, the BD Logo and Rotarex are trademarks of Becton, Dickinson and Company or its affiliates.
© 2026 BD. All Rights Reserved. BD-174954
Read More
Insights into Acute Limb Ischemia Management With Rotarex™ Atherectomy System
Micah Watts, MD, FSIR, Atlantic Medical Imaging, New Jersey


