


Percutaneous Transmural Arterial Bypass for Complex Femoropopliteal Disease: A Case Series Across Challenging Anatomies
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.

Haris Usman, MD, MS, FACC, FSCAI, and Ramzan M. Zakir, MD, RPVI, FACC, FSCAI
RWJBarnabas Health, New Jersey
Long femoral lesions of greater than ≥200 mm represent a subset of complex femoropopliteal disease that is classified as TASC C or D.1 These long, complex lesions have historically been associated with less favorable outcomes following conventional percutaneous revascularization compared to shorter lesions, with higher rates of restenosis and revascularization.2 In addition, many patients with extensive femoropopliteal disease have anatomical and clinical factors that limit suitability for surgical bypass.
The DETOUR System™ (Endologix) enables completion of percutaneous transmural arterial bypass (PTAB) and is designed to treat long femoropopliteal lesions by creating an extra-anatomic bypass through the femoral vein. This novel percutaneous technique involves creation of arterial-venous anastomoses between the femoropopliteal artery and the femoral vein, allowing delivery and deployment of the TORUS Stent Graft (Endologix) through these anastomoses to form a percutaneous bypass. This procedure expands treatment options in complex disease by offering the advantages of an endovascular safety profile and recovery time, while simultaneously providing benefits that may be similar to surgical bypass.3-6 Here, we discuss the utility of the DETOUR System in various anatomical scenarios in two case examples, with the intent of illustrating clinical considerations for patient and lesion selection.
Case 1: Endovascular Salvage of a “No-Landing-Zone” SFA: DETOUR PTAB Through Prior Stents
A 71-year-old female with hypertension, coronary artery disease, and prior CABG presented with recurrent resting limb ischemia, nocturnal calf pain, and a nonhealing toe ulcer. She had undergone multiple prior revascularizations, including endarterectomy, iliac angioplasty, and multiple left superficial femoral artery (SFA) interventions. Her ABI was 0.19. The patient declined surgical revascularization, so percutaneous transmural arterial bypass (PTAB) with the DETOUR System was performed.
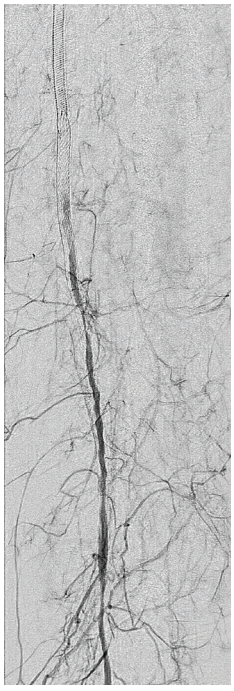
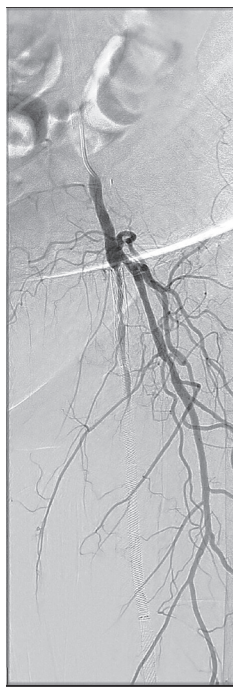
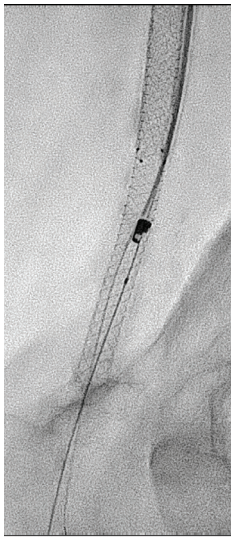
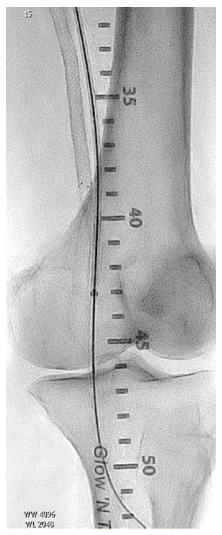
An initial diagnostic angiogram showed 300 mm of complete occlusion of the in-stent segment of the SFA, stented distally until the first segment of the popliteal artery, with distal reconstitution and three-vessel runoff (Figures 1-2). Since there was a need to have at least 3 cm of landing zone for proximal anastomosis with the DETOUR System, we proceeded to cross and treat this segment with a 5.0 mm x 60 mm Serranator balloon (Cagent Vascular). Simultaneous access was obtained to the left posterior tibial vein, and after verifying a sufficient size of the vein, an EN Snare (Merit Medical) was advanced and placed at the point of proximal entry for anastomosis. The proximal anastomosis was created with the ENDOCROSS needle (Endologix) into the proximal vein through the EN Snare. The captured .014-inch Grand Slam wire (Asahi Intecc) was externalized through the posterior tibial vein to create a robust rail. Serial dilatation using 2.0 mm x 40 mm and 4.0 mm x 40 mm NanoCross balloons (Medtronic), followed by a 6.0 mm x 40 mm Mustang balloon (Boston Scientific), enabled sufficient dilation through the SFA stent struts to allow for transition of the ENDOCROSS catheter (Figure 3).
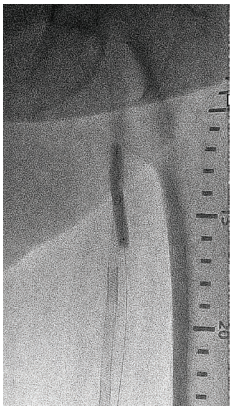
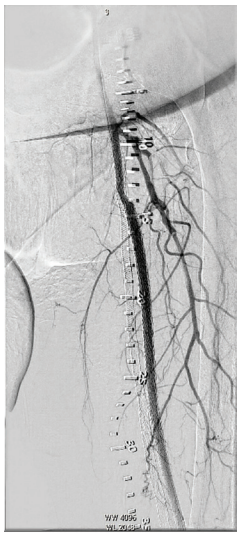
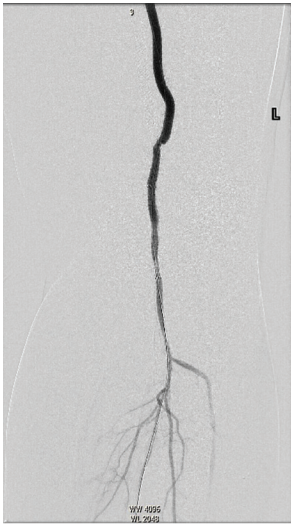
Distal crossing from the popliteal vein into the first segment of the popliteal artery stented segment was conducted using the ENDOCROSS catheter (Figure 4), followed by serial dilatation with the same 2.0 mm x 40 mm and 4.0 mm x 40 mm NanoCross balloons, and a 6.0 mm x 40 mm Chocolate balloon (Medtronic). Two TORUS Stent Grafts, a 6.0 mm x 200 mm and a 6.7 mm x 150 mm, were deployed from the distal to the proximal anastomosis. A 7.0 mm x 120 mm Mustang balloon was used for post dilatation, conducted over an .035-inch steel core wire that was 300 mm long (Figure 5). Repeat angiographic assessment showed robust flow from the proximal to distal anastomosis, and three-vessel distal runoff to the foot (Figures 6-7). At 3-month follow-up, the patient continued to do well, with repeat ABIs of 0.98 on the left side and healing of the great toe ulcer.
Conclusion: Case #1.
This case demonstrates:
• The feasibility of PTAB in treating long, Tosaka Class III ISR SFA segments;
• Technical considerations for anastomosis within prior stents;
• The importance of vessel preparation for device delivery;
• Successful restoration of blood flow (improvement to ABI of 0.79), enabling subsequent wound healing.
Case 2: Initial Treatment Approach Using the DETOUR System With a Long, Heavily Calcified SFA Chronic Total Occlusion
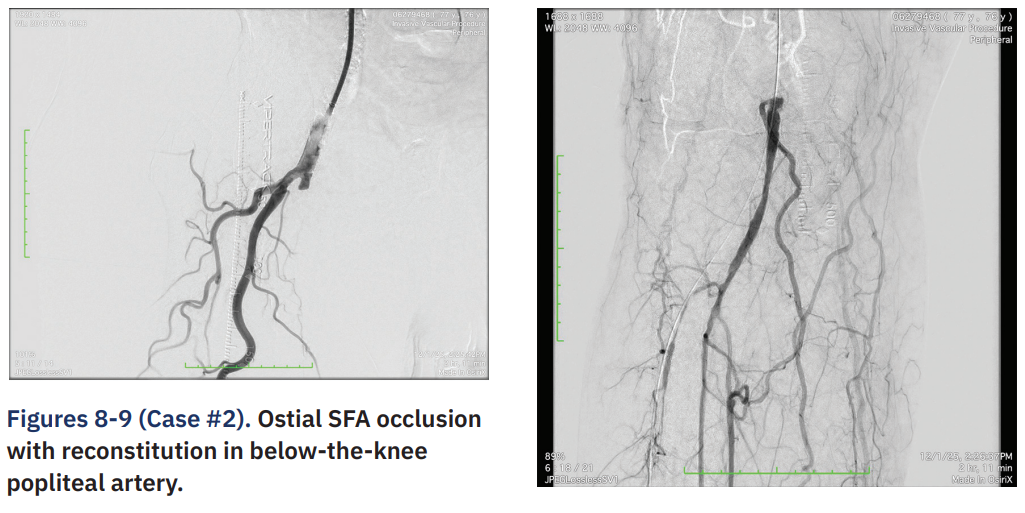
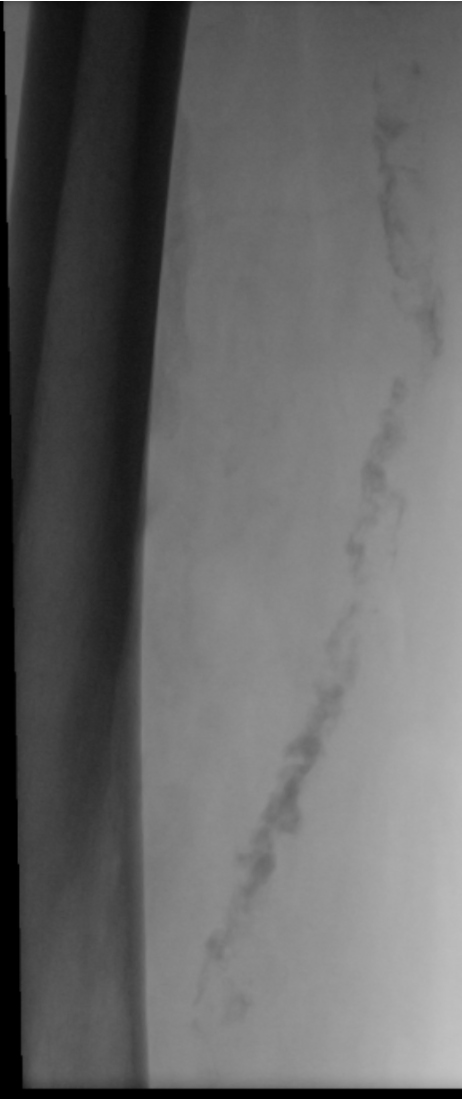
A 76-year-old male with dyslipidemia and venous insufficiency with prior bilateral great saphenous vein ablation presented with severe lifestyle-limiting claudication despite compliance with a structured exercise program and was referred for revascularization. An arterial duplex ultrasound revealed bilateral SFA occlusions. Initial angiography revealed an ostial SFA occlusion with reconstitution in the below-the-knee popliteal artery (Figures 8-9). Given the lesion complexity with a long segment occlusion and severe calcium and lack of surgical conduit (Figure A [Online only]), PTAB was selected as the preferred strategy.
Access was obtained in the left common femoral artery and an 8 French (Fr), 45 cm sheath was advanced into right common femoral artery. Venous access was obtained in the right anterior tibial vein and a 6Fr sheath was inserted. Systemic anticoagulation was achieved with heparin. A 9-15 mm snare was inserted into the venous sheath and advanced to the lesser trochanter (Figure 10). Selective access was obtained into the right SFA, which was predilated with a 5.0 mm x 40 mm Mustang balloon. The ENDOCROSS was inserted over a .014-inch Glidewire Advantage (Terumo) 3-4 cm distal to the SFA/profunda bifurcation. The ENDOCROSS was fired 1 time to create a proximal anastomosis, and a Grand Slam .014-inch wire was advanced into the vein and captured by the snare system, which was then removed. The ENDOCROSS was removed and re-prepped. A 4.0 mm x 40 mm Coyote balloon (Boston Scientific) was used to dilate the proximal anastomosis from the artery into the vein. The ENDOCROSS was then re-inserted, advanced over the wire through the proximal anastomosis into the vein and positioned distal to the occlusion. The ENDOCROSS was superimposed over the popliteal artery. The ENDOCROSS was fired 1 time, creating a distal anastomosis and obtaining access into the popliteal artery. The Glidewire Advantage was advanced into the PT artery distally to maximize wire purchase. The ENDOCROSS was removed, and a 4 mm x 40 mm Coyote balloon and then a 4.0 20 NC Emerge balloon (Boston Scientific) was used to dilate the distal venous/artery anastomosis. A .035-inch x 135 cm NaviCross was then advanced and used to exchange the .014-inch wire for a Supra Core .035-inch x 300 cm wire.
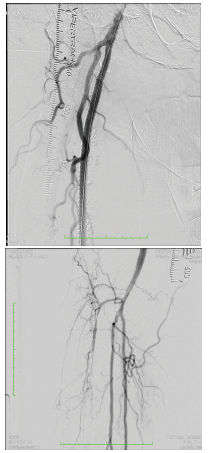
Three TORUS Stent Grafts were used. The first 6 mm x 200 mm TORUS Stent Graft was deployed to provide a 3 cm distal landing zone in the popliteal artery. The second 6.7 mm x 200 mm TORUS Stent Graft was deployed with 8 cm overlapping into the first stent graft. An angiogram was used to visualize the bifurcation of the proximal SFA and profunda. The third 6.7 mm x 200 mm TORUS Stent Graft was deployed with 10 cm overlapping into second stent graft. The entire series of TORUS stent grafts were post-dilated with a 7.0 mm x 100 mm Mustang balloon proximally and a 6.0 mm x 200 mm Armada balloon (Abbott) distally, focusing on the anastomosis site. Final angiography revealed brisk filling down the stent grafts and good outflow (Figures 11-12). Our patient has remained claudication-free with normal non-invasive testing.
Conclusion: Case #2
In patients who are not candidates for an open surgical approach, as was the case with our patient, PTAB may be considered an alternative strategy to achieve durable patency. Within the DETOUR2 pivotal study, primary patency was 81.8% and 58.2% through 12 and 36 months, respectively.3 Freedom from clinically driven target lesion revascularization was 87.7% and 66.8% through 12 and 36 months, respectively.3
Discussion and Conclusion
In this case series, PTAB using the DETOUR system successfully utilized across a range of challenging anatomic and clinical scenarios that traditionally limit the feasibility of conventional endovascular or open surgical revascularization. Our experience demonstrates safe and effective use in heavily calcified, fully stented vessels and in single-vessel runoff scenarios, where preserving distal perfusion is critical and procedural tolerance for embolic or flow limiting complications is low. These findings support the therapy’s utility in complex anatomies. Crossing through stent interstices did not appear to limit device delivery or conduit formation, and no stent-related mechanical complications were observed. Prior stenting, even when extensive, may not preclude use of the DETOUR System in selected patients and may expand treatment options for patients with recurrent in-stent occlusions. Similarly, by leveraging the extravascular pathway, the DETOUR System avoids many of the limitations imposed by calcified plaque morphology, reinforcing its utility in “no-option” femoropopliteal disease where traditional endovascular tools are unlikely to achieve durable luminal gain. Finally, favorable outcomes observed in single- vessel runoff limbs represent a high-risk cohort in whom distal embolization, flow disruption, or prolonged ischemia can have outsized clinical consequences. The absence of major periprocedural complications and the preservation of distal perfusion in our series support the feasibility of PTAB using the DETOUR system, even in tenuous runoff conditions. While long-term patency in this subgroup warrants further study, the early technical and clinical success is encouraging.
In conclusion, these cases illustrate the versatility of the DETOUR System and its potential role in expanding revascularization options for patients with complex femoropopliteal occlusive disease. Although our experience is limited by sample size and follow-up duration, the consistency of technical success across diverse anatomic challenges suggests that the device may fill an important niche between conventional endovascular therapy and open surgical bypass. Larger studies with longer follow-up are needed to continue to define durability, patient selection, and comparative outcomes, but our findings contribute to the growing evidence supporting the use of percutaneous transmural arterial bypass in real world, high-complexity scenarios.
This article is sponsored by Endologix.
The DETOUR™ System and associated components, ENDOCROSS™ Device and TORUS™ Stent Graft System, are not available in all countries or regions. Please contact your Endologix representative for details regarding product availability. Prior to use, refer to Instructions for Use for more information concerning Indications, Contraindications,Specific Anatomic Considerations, Warnings, Precautions, and Adverse Events. Rx only. ©2026 Endologix LLC. All rights reserved. MM3008-US Rev 01
References
1. Norgren L, Hiatt WR, Dormandy JA, et al; TASC II Working Group. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg. 2007 Jan; 45 Suppl S: S5-S67. doi:10.1016/j.jvs.2006.12.037
2. Horie K, Takahara M, Nakama T, et al. Three-year outcomes of contemporary endovascular treatment in over 25-cm femoropopliteal artery disease from a retrospective multicenter registry: A retrospective observational study. Catheter Cardiovasc Interv. 2024 Oct; 104(4): 782-789. doi:10.1002/ccd.31202
3. Lyden SP, Soukas PA, De A, et al; DETOUR2 Trial Investigators. DETOUR2 trial outcomes demonstrate clinical utility of percutaneous transmural bypass for the treatment of long segment, complex femoropopliteal disease. J Vasc Surg. 2024 Jun; 79(6): 1420-1427.e2. doi:10.1016/j.jvs.2024.02.004
4. Lyden SP. Results of the DETOUR2 Study: Durability of Percutaneous Transmural Arterial Bypass for Treatment for Complex Femoropopliteal Disease. Presented at: Vascular InterVentional Advances (VIVA) 2024; November 3-6, Las Vegas, Nevada.
5. Rumba R, Krievins D, Ezite N, et al. Endovascular transvenous versus open femoropopliteal bypass. Medicina (Kaunas). 2024 May 8; 60(5): 777. doi:10.3390/medicina60050777
6. Sayfo S, Ryschon AM, Sood A, et al. Long femoropopliteal lesions challenge the limits of endovascular technique: contemporary systematic review and meta-analysis. J Soc Cardiovasc Angiogr Interv. 2026 Feb 3; 5(3): 104158. doi:10.1016/j.jscai.2025.104158
Find More
PTAB With the DETOUR™ System: Expanding Treatment Options for Complex PAD Patients
CLD talks with Jaafer A. Golzar, MD, FACC, FSCAI.


