


What’s New in the “2026 Acute Pulmonary Embolism in Adults” Multi-Society Guidelines
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Morton J. Kern, MD, MSCAI, FACC, FAHA
Clinical Editor; Interventional Cardiologist, Long Beach VA Medical Center, Long Beach, California; Professor of Medicine, University of California, Irvine Medical Center, Orange, California
Disclosures: Dr. Morton Kern reports he is a consultant for Abiomed, Abbott Vascular, Philips, ACIST Medical, and Opsens Inc.
Dr. Kern can be contacted at mortonkern2007@gmail.com
On X @MortonKern
New guidelines for the evaluation and management of acute pulmonary embolism (PE) in adults, a report of the American College of Cardiology (ACC) and American Heart Association (AHA) Joint Committee on clinical practice guidelines, are now published in the Journal of the American College of Cardiology and Circulation.1 This 2026 update and expansion of the guidelines for the management of PE is a masterwork of guideline production, and is important for those managing patients with acute PE and developing care systems to expedite acute emergency management principles. I thought it would be worthwhile to recap the message of the guidelines for cath lab staff who are increasingly taking on roles with the PERT team (Pulmonary Embolism Response Team).
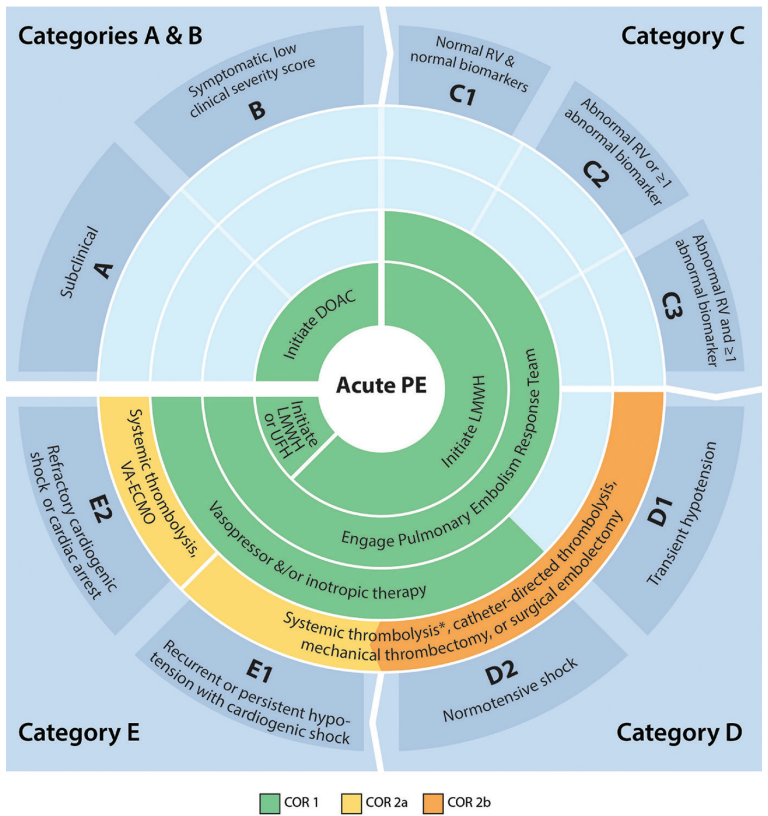
*If acceptable bleeding risk.
ACC = American College of Cardiology; AHA = American Heart Association; COR = Class of Recommendation; DOAC = direct oral anticoagulants; LMWH = low-molecular-weight heparin; PE = pulmonary embolism; RV = right ventricle; UFH = unfractionated heparin; VA-ECMO = veno-arterial extracorporeal membrane oxygenation.
Reprinted with permission from Dudzinski DM, Cibotti-Sun M, Moore MM. 2026 Acute Pulmonary Embolism Guideline-at-a-Glance. J Am Coll Cardiol. 2026 Apr 7; 87(13): 1620-1625. doi:10.1016/j.jacc.2025.12.023
It is recognized that most cardiac catheterization laboratories are not the first point of medical care and do not deal with PE immediately. However, it is worth understanding the presentation and pathways that some of our chest pain patients may encounter. Acute PE management begins in the emergency department (ED) with the clinical presentation and providers’ recognition of the syndrome and assessment of PE likelihood and risk (Figure 1). The patient’s story and risk factors will then establish the probability of having a PE, followed by a rapid progression through a variety of laboratory and imaging assessments, mostly involving computed tomography (CT) angiography and echocardiographic measurements of right ventricular (RV) function. The RV size and function will then determine whether a conservative or an aggressive, often invasive, approach is required. The highest risk patients are taken to the interventional lab for mechanical thrombectomy. This pathway is described below and often directed by the PERT team. Post-acute PE management involves treating underlying risk factors as well as long-term anticoagulation (described in the guidelines in detail).
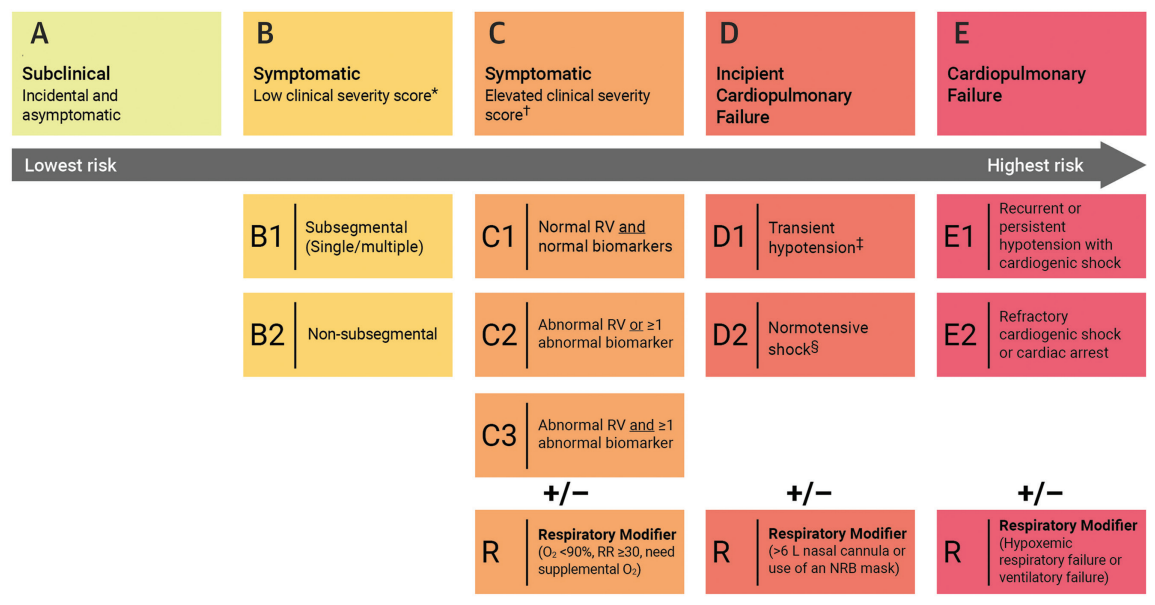
*Low Clinical Severity Score includes PESI #85 or sPESI =0 or Bova # 4.
†Elevated Clinical Severity Score includes PESI >85 or sPESI $1 or Bova > 4.
‡Systolic blood pressure <90 or decrease >40 mm Hg lasting <15 min or responding to IV fluids. Lactate >2 mmol/L, acute kidney injury, urine output <0.5 mL/kg/hr., mental status change, cardiac index <2.2 L/min/m2, mean arterial pressure <60 mm Hg, increased shock score/stage (SCAI stage, CPES score).
ACC indicates American College of Cardiology; AHA, American Heart Association; CPES, Composite Pulmonary Embolism Shock; IV, intravenous; NC, nasal cannula; NRB, nonrebreather; O2, oxygen; PE, pulmonary embolism; PESI, Pulmonary Embolism Severity Index; RR, respiratory rate; RV, right ventricle; and sPESI, simplified PESI.
Reprinted with permission from Creager MA, Barnes GD, Giri J, et al. 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the evaluation and management of acute pulmonary embolism in adults: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2026 Apr 7; 87(13): 1626-1710. doi:10.1016/j.jacc.2025.11.00
The 2026 acute PE guidelines establish 5 new risk categories (Figures 1-2). The categories are designated A through E, and each has sub-categories to provide a refined classification of prognostic accuracy to guide therapeutic decision-making across the spectrum of risk from the early acute phase of the PE. Categories A and B describe subclinical or mildly symptomatic, low-clinical severity patients in whom novel oral anticoagulants are administered.
For patients presenting in category C or higher, the PERT team becomes active, and all patients receive low-molecular-weight heparin. The ‘C’ subcategories include those patients with normal RV without biomarkers (C1), abnormal RV with one or more biomarkers (C2) and abnormal RV with positive biomarkers (C3). As the patient’s status becomes more clinically severe, they enter risk category D1 transient hypotension or D2 with normotensive shock. Depending on the severity of hypotension, vasopressor/inotropic therapy may be required, as well as systemic thrombolysis, catheter-directed thrombolysis or mechanical/surgical embolectomy. For those patients with cardiogenic shock with either recurrent (E1) or refractory (E2) courses, the management escalates. In addition to vasopressors, inotropes, and pharmaco-mechanical thrombolysis, systemic mechanical circulatory support with venoarterial extracorporeal membrane oxygenation (VA-ECMO) may be required.
The complex and escalating care of the acute PE patient is facilitated in large measure by the PERT team2,3 with multiple care disciplines activated and ready to participate when called upon (Figure 3). The benefits of the PERT team are derived from the various members which include vascular medicine, pharmacy, intensive care unit/ED nursing, emergency medicine, cardiac surgery, and pulmonologists and cardiologists.
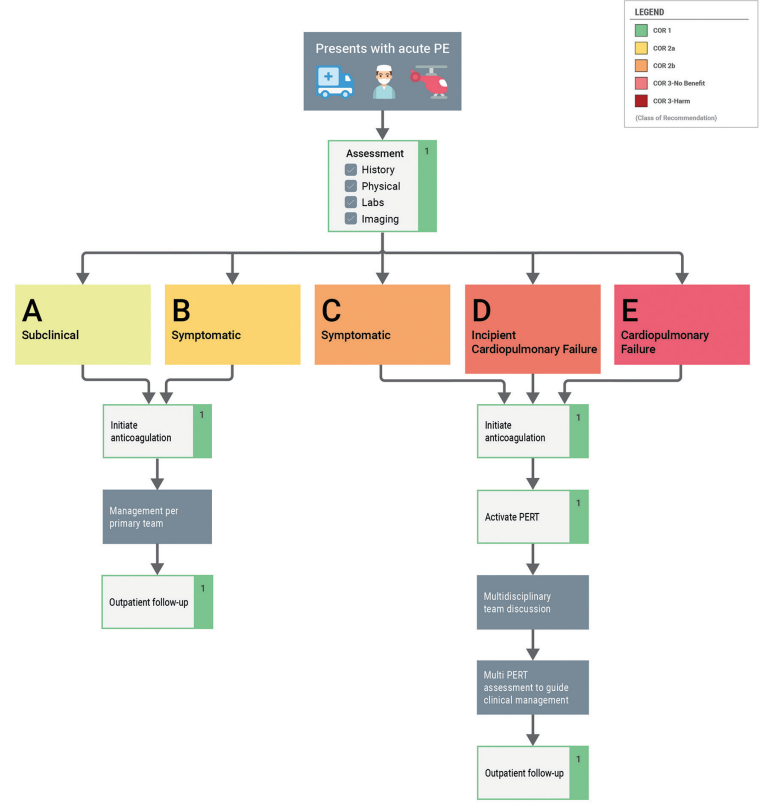
COR indicates class of recommendation; PE, pulmonary embolism; PERT, pulmonary embolism response team.
Reprinted with permission from Creager MA, Barnes GD, Giri J, et al. 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the evaluation and management of acute pulmonary embolism in adults: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2026 Apr 7; 87(13): 1626-1710. doi:10.1016/j.jacc.2025.11.00
Modified from Rosovsky R, Borges J, Kabrhel C, Rosenfield K. Pulmonary embolism response team: inpatient structure, outpatient follow-up, and is it the current standard of care? Clin Chest Med. 2018 Sep; 39(3): 621-630. doi:10.1016/j.ccm.2018.04.019
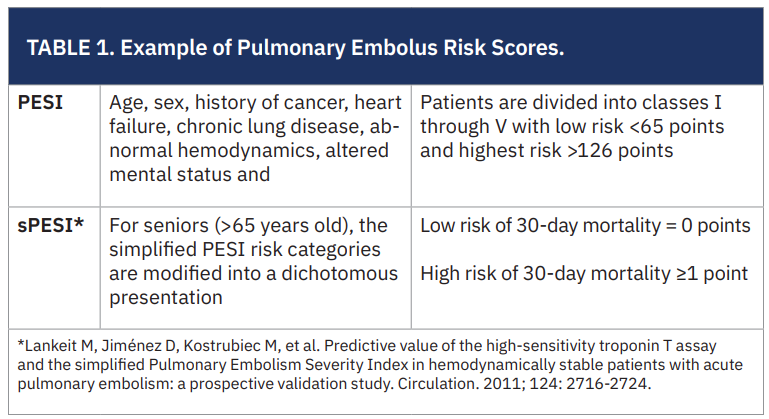
Acute PE Clinical Risk Prediction Scores
Predicting clinical risk of PE is critical to the initial decisions for patient management. The risk score supports decisions to take a conservative or aggressive approach. There are many different acute risk prediction scores used by EDs, the choice of which is usually determined by local custom. Table 1 shows two common scores for PE risk assessment. Many others can be seen in the guidelines document. The PERT activation pathway (Figure 3) identifies where interventions are most needed. Additional clinical decision rules about invasive treatment also may incorporate the reassessment with additional scoring systems, like Wells’ Criteria or the Geneva Score (Revised).4,5
 2026 AHA/ACC Acute PE Guidelines: Take-Home Messages
2026 AHA/ACC Acute PE Guidelines: Take-Home Messages
I’ve encapsulated some of the take-home points to consider when perusing the guidelines. I think this will promote more in-depth reading for those involved in the care of the PE patient.
- The clinical risk of the acute PE patient falls into one or more of the 5 categories A-E. These groups provide an evidence-based approach to therapeutic decision making.
- Acute PE patients who are asymptomatic in category A or who are symptomatic but have a low clinical severity score (category B) can be candidates for early hospital discharge, sometimes from the ED.
- Symptomatic patients with elevated clinical severity score (category C or D) with biomarkers, RV dysfunction, or cardiopulmonary failure should be hospitalized to optimize treatment approaches.
- The more acutely ill patients (category D2 or E) with hypotension should be considered for mechanical or catheter- based thrombolysis as well as hemodynamic cardiac support.
- PERT teams are recommended to improve timeliness of care delivery.
- Low-molecular-weight heparin is recommended over unfractionated heparin for patients with acute PE requiring parental anticoagulation (category A-C).
- Direct oral anticoagulants (DOACs) are recommended over vitamin K antagonists (warfarin) unless contraindicated to prevent recurrent venous thromboembolism and bleeding.
- For post-acute PE care, in patients with first PE without major reversible risk factors, continue anticoagulation beyond 3-6 months. Annual screening of patients who have had acute PE should assess symptoms and functional status to reduce the likelihood of chronic thromboembolic pulmonary disease or other cause of dyspnea, and functional limitation.
The Bottom Line
Cath labs are increasingly involved in PE care. The role of the cath lab in the management of pulmonary embolus is more often in the chronic phase, where dyspnea and pulmonary hypertension play a major role as the cause of the patient’s symptoms. Right heart catheterization with or without coronary angiography becomes a paramount diagnostic test to determine where this patient lies in the management spectrum of their dyspnea and chronic disease.
The 2026 acute PE guidelines are worth reading for all those involved in the care of these patients. As some in the cath lab may work in interventional radiology, we should all be aware of patients with pulmonary embolism who can be acutely managed and supported to prevent future adverse events and improve their overall clinical course.
References
- Creager MA, Barnes GD, Giri J, et al. 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the evaluation and management of acute pulmonary embolism in adults: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2026 Apr 7; 87(13): 1626-1710. doi:10.1016/j.jacc.2025.11.00
- Rosovsky R, Borges J, Kabrhel C, Rosenfield K. Pulmonary embolism response team: inpatient structure, outpatient follow-up, and is it the current standard of care? Clin Chest Med. 2018 Sep; 39(3): 621-630. doi:10.1016/j.ccm.2018.04.019
- Bejjani A, Khairani CD, Campia U, Piazza G. Pulmonary embolism response teams: theory, implementation, and unanswered questions. J Clin Med. 2022 Oct 18; 11(20): 6129. doi:10.3390/jcm11206129
- Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients’ probability of pulmonary embolism: increasing the model’s utility with the SimpliRED D-dimer. Thromb Haemost. 2000; 83(3): 416-420.
- Klok FA, Mos IC, Nijkeuter M, et al. Simplification of the revised Geneva score for assessing clinical probability of pulmonary embolism. Arch Intern Med. 2008 Oct 27; 168(19): 2131-2136. doi:10.1001/archinte.168.19.2131



