Artificial Intelligence in the Cath Lab: A Pragmatic Current-State Analysis for the Practicing Interventional Cardiologist
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
 Jacob McAuliffe, MD is a cardiology fellow at Inova Schar Heart & Vascular in Falls Church, Virginia. He completed his residency training at Eastern Virginia Medical School. Prior to medical school, he completed a Master of Science & Technology Policy degree through the Consortium for Science, Policy, and Outcomes and worked as a Health Policy Fellow in Washington, D.C., cultivating an interest in advocacy, governance and responsible integration of emerging medical technologies into clinical practice. His scholarly and clinical interests converge at the intersection of interventional cardiology, health policy, and the responsible deployment of AI-enabled clinical tools.
Jacob McAuliffe, MD is a cardiology fellow at Inova Schar Heart & Vascular in Falls Church, Virginia. He completed his residency training at Eastern Virginia Medical School. Prior to medical school, he completed a Master of Science & Technology Policy degree through the Consortium for Science, Policy, and Outcomes and worked as a Health Policy Fellow in Washington, D.C., cultivating an interest in advocacy, governance and responsible integration of emerging medical technologies into clinical practice. His scholarly and clinical interests converge at the intersection of interventional cardiology, health policy, and the responsible deployment of AI-enabled clinical tools.
Disclosures: Dr. McAuliffe reports no conflicts of interest regarding the content herein.
Jacob McAuliffe, MD, can be contacted at Jacob.McAuliffe@inova.org
PART 1 – What is AI?
This article series is intended as a current-state analysis of artificial intelligence within the cath lab and field of interventional cardiology.
• Part 1 will provide a contextual framing and seek to establish working terminology.
• Part 2 will examine diverse applications of AI and review examples already integrated in the cath lab across the full procedural workflow.
• The final, Part 3, will help operators develop a critical perspective and set of questions to inform suitability assessments for future AI applications.
Over its course, this series will highlight broader implications of AI’s continued evolution for the field of interventional cardiology, and the professional responsibility these thrust upon operators to engage critically and deliberately in preparation to best utilize the emerging generation of AI clinical tools.
I – A Blooming, Not an Emergence
Contemporary discussion of AI is largely framed with an air of anticipation toward healthcare, as if the technology has only in the past years begun to mature and is still to come of age. Conversations with colleagues are likely still treating AI as something to prepare for, emphasizing a need to evaluate emerging applications with skepticism. For the cath lab, that framing is already obsolete. AI will not be coming to the cath lab; it has already arrived.
For over a decade, machine learning algorithms have empowered interventionalists through applications such as quantitative coronary angiography, intravascular imaging, and real-time hemodynamic analysis. These platforms deliver valuable clinical information at speed and scale irreplicable by human operators, representing an invaluable addition to the interventionalist’s war chest already in comfortable daily use in cath labs across the world.
The achievement of functional generative AI has been a key igniting factor driving the current AI craze; however, it represents the maturation of a broad field, one that has achieved a plurality of advancements that will have clinical impact.1 What has changed is not the fundamental nature of machine learning, but rather the degree and sophistication of our ability to train and deploy AI models at scale for widespread use. The emergence of generative AI reflects less a novel computational capacity than the dramatic result of training methodology refinement coupled with hardware sophistication and proliferation of data center infrastructure. The enthusiasm surrounding generative AI is not misplaced. The leap is genuine and represents a milestone for human society. The critical observation, however, is that this leap was made from a foundation that has existed within healthcare, within the cath lab, for decades.
The advent of generative AI inspires a wealth of new potential clinical applications. Broadly, AI tools can be understood as serving one of two primary functions, or a combination thereof: extractive and generative. Extractive capacity has been the dominant function utilized thus far in cath lab applications (real-world examples will be discussed in Part 2). Novel generative capabilities attract well-deserved attention and have the potential to influence how we plan, execute, and analyze interventional procedures.
The central question facing practicing interventionalists is not whether to engage with AI, but rather when they engage, will they do so on their own terms as informed, critical participants in the development and deployment of the next generation of AI clinical tools.
The state of our current electronic health records (EHR) system is an instructive precedent. The fractured, commercially driven landscape of EHRs in the United States emerged, in no small part, from how that technology was first introduced, regulated, and subsequently entrenched.2 It is an enterprise that reached conclusive momentum before clinicians had the framework or organized voice to shape the paradigm’s architecture in foundational ways. The political, financial, and social capital now required to substantially reform the EHR industry would be immense. Future AI applications, especially those destined to become embedded in the daily workflow of a broad swath of healthcare workers, face precisely this same entrenchment risk. If interventional cardiologists are to use these tools in practice, our community should develop a prominent voice in the conversations that will determine how these tools are developed, validated, and regulated.
II – Clarifying & Understanding Terminology
It’s interesting: now that the post-Turing-test functionality of generative chatbots is mainstream, there is less hesitancy to use the moniker of “artificial intelligence.” In fact, there is now an enthusiasm to employ the term. In the past, terminology such as “machine learning” helped shield genuine academic, innovative efforts from reflexive skepticism, from those who dismissed the concerted efforts towards developing generative AI as a moonshot. Now with fluent AI models, the technical and common terminology we use to discuss this field has become muddied.
Before evaluating any AI-powered clinical tool, a working vocabulary is essential. In common conversational use, terms surrounding AI are frequently employed interchangeably and imprecisely. This is a phenomenon resulting from individuals not trained in a specific field trying to employ technical terms in contextually accurate ways, with an end result that may not be accurate.
The ambiguity of common parlance is compounded by a deliberate trend within industry toward marketing new products with the latest AI-adjacent vocabulary, for example “AI-powered,” “deep learning-enabled,” or (also becoming outdated) simply, “smart.” Just as interventional cardiologists have formalized a working vocabulary for coronary anatomy and lesion morphology, a parallel pragmatic vocabulary for AI has become a professional necessity for the modern interventionalist.
Artificial Intelligence (AI) describes a field of innovation. It is the broadest umbrella term and encompasses any computational system designed to perform tasks independently that would otherwise require human intelligence to complete with reliable accuracy. To say an application is “AI” holds similar descriptive power to saying the Cybertruck is an “automobile.” Just as all four-wheeled vehicles share core engineering yet serve vastly different functions (i.e., a school bus, a dump truck, a Formula 1 car, a backhoe), so too should “AI” be understood as a category that includes a vast range of functions and utilities. As a label, it is so broadly applied and so commercially loaded that “AI” carries very little descriptive value on its own.
Machine Learning (ML) can be thought of as a computational approach that forms the basis for more advanced AI models. ML concerns training software to identify patterns in complex data via goal-oriented training methodologies. By consuming massive amounts of data and running the same training “scenarios” countless times, ML develops internal algorithms capable of producing outputs with increasing accuracy. Here’s an example: remember how your eyes felt when you saw your first angiogram — could you make heads or tails of what was abnormal? Through countless cases, your brain trained itself. It knows what to pay attention to and can interpret coronary angiograms in real time, something we take as second nature yet struggle to articulate as a set of explicit rules. Our brains have developed a fluency through training built from pattern recognition, not from a consciously learned algorithm. ML has been the dominant AI paradigm in cardiovascular medicine for years, yet one seldom encounters the term in contemporary product positioning.
Neural Networks are a computational architecture (software) based on discrete processing nodes, interlinked in a fashion inspired by organic neural circuitry (i.e., the human brain). Individual nodes are arrayed in processing layers, each performing discrete analytic functions, with the processed output of one node feeding into subsequent nodes. The collective processing of nodes, which may number in the thousands or millions, produces a final output that is evaluated for accuracy.
Consider 15 first-year interventional cardiology fellows, say in a July bootcamp, arranged in three rows of five. The first row is provided a full angiogram study (raw data) and tasked to select up to 10 key frames that best capture the lesions present; they must also try to label each vessel in the frame. (For a NN to do this, it would first have to turn the angiograms into understandable data, effectively turning pixels into “1s and 0s”, a process called “encoding.”) Each first-row fellow reviews, labels, and then passes back their set of partially annotated frames. Each second-row fellow thus receives five sets of up to 10 frames. They are tasked with selecting up to five frames, then highlighting the extent of the 3 most critical lesions (color coded for priority). In the same fashion as before, the third-row fellows each receive annotated sets from the second row. This final row is tasked with considering all annotated frames provided, then making a list of targets, with recommendations for prioritization and lesion length approximation. The five recommendations from the final row are aggregated (via a prespecified protocol, a concept similar to “decoding” within NN architecture); this produces a single final output. No single fellow could be said to have made the ultimate recommendation, as the output of this process emerged from collective, layered processing. If ran 10 or 100 times, while a surely timely endeavor, would you trust this relatively clumsy system to produce recommendations more often aligned with a practicing interventionalist compared to the average performance of the 15 first years in isolation?
Within NN training methodologies, architectures (aka, “nodal pathways”) that yield correct results are reinforced; those that do not are deprioritized through iterative training. This optimization gives rise to what is referred to as the "black box." This term describes a system whose internal logic, while computationally powerful, is not readily interpretable by outside (i.e., human) observers. Let’s return to our first-year fellow analogy. It is relatively easy to piece together how each layer’s processing task contributed to the overall computation. Now consider a NN with hundreds of layers. While the action of a single node might still be readily dissectible, just as understanding the firing pattern of a single neuron cluster doesn’t inform cognitive function, so too does the ability to intuit the AI’s “thought process” steeply decline as more nodes and layers are incorporated into the parallel processing schema. This processing opacity is among the most frequently cited concerns about the rapid integration of AI into clinical decision-making and represents a genuine epistemological challenge for a field grounded in mechanistic and pathophysiologic reasoning. Much active research is dedicated toward increasing the transparency into computational reasoning of advanced AI models.
Deep Learning (DL) is a newer term describing the sophistication of ML through neural network architecture, enabling AI models to recognize increasingly complex patterns from less pre-processed or annotated data. Deep learning has proven especially powerful for image recognition tasks, making it particularly relevant to angiographic, intravascular imaging, and echocardiographic applications.
Large Language Models (LLMs) represent a distinct and increasingly prominent category of AI applications. Trained on vast corpora of text drawn from across the internet, LLMs such as GPT-4, Claude, Gemini, and Grok can utilize natural language with remarkable fluency. These are the defining expression of generative AI functionality. At their core, LLMs are built on deep learning architectures trained toward a deceptively simple goal: predict the next word given everything that came before it, including what has so far been generated in the drafted output, as well as with reference to the original prompt. All of this consideration simply boils down to computing which word will have the highest probability of making the most contextual sense. Trained iteratively across billions and billions of examples, this ultimately produces models with emergent reasoning and language capabilities far beyond word completion (“fill in the blank”) capacity. LLMs represent advanced specialization of AI models. While they represent a broad and powerful use case, LLMs are not omnipotent agents, and their word prediction abilities begin to fail when tasked with highly specific or advanced analytical inquiries if the model was not trained on sufficient specialty-specific content.
Natural Language Processing (NLP). LLMs utilize NLP like cars utilize motors. In clinical settings, NLP enables systems to extract structured data from free-text documentation, power automated transcription, and underpin chatbot-style interfaces. NLP is a foundational component of the large language models now entering clinical workflows. NLP is not a ubiquitous ability. Different models will employ different architectures that achieve the functional use, in a process resemblant of convergent evolution. NLP might be considered similar to the transmission system of a car; different models of cars employ separately engineered transmissions (e.g., a luxury supercar compared to a commuter sedan or pickup).
Foundational Models are LLMs that are broadly trained, usually under semi-supervised methodologies, to be able to perform NLP in a “jack of all trades” level of competence. The commercial AI agents such as Claude and ChatGPT are examples. Foundational models aren’t trained with a specific field or use case in mind. Rather the goal of their development is broad, adaptive use. As the name implies, once adequately trained, foundational models can serve as the basis for training more specialized agents or models. The nature of foundational model training, in particular the constant iterative development, raises several important considerations in regard to assessing specialized clinical applications. These are numerous, with the most important being consideration for planned updates and re-validation processes.
Extractive AI refers to systems that identify, quantify, or classify patterns within existing data. The idea is to surface signals inaccessible to routine human observation at scale or speed, potentially recognizing patterns the human eye or brain are incapable of identifying in isolation. These systems do not create new information so much as render existing information clinically actionable.
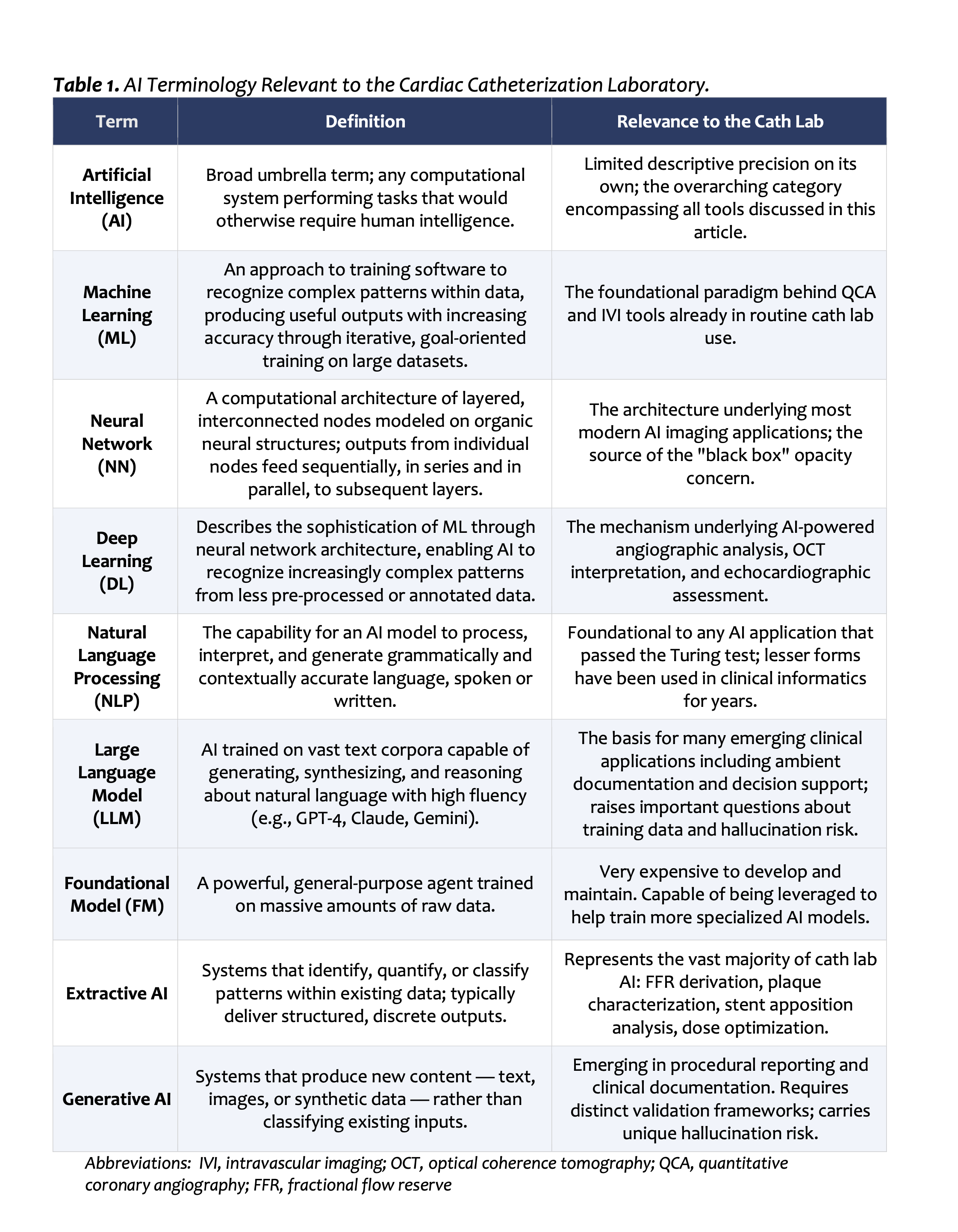
Generative AI refers to systems that produce new content — text, images, or other synthetic data — rather than analyzing existing inputs to produce a classification or measurement. The validation and risk considerations for generative systems differ fundamentally from those applicable to extractive tools, a distinction discussed further below. One of the largest concerns around clinical application of generative AI is the well-documented phenomenon of “hallucinations,” where an AI model confidently presents a factually incorrect conclusion. There has been substantial research toward mitigating the incidence and severity of hallucinations, and many strategies are already commonly employed. For example, requiring a generative AI model to cite the source material informing its conclusion, be it a prior note in the chart or a specific guideline or article, greatly reduces the incidence of hallucinations and makes their detection more readily identifiable.
Why does this vocabulary matter in practice? Because a physician who cannot pragmatically distinguish a deep learning image classifier from a generative LLM documentation tool is poorly equipped to evaluate the suitability or clinical validity of novel AI tools presented by vendors or colleagues. Formal AI education remains strikingly absent from most medical training programs worldwide. A 2022 systematic review examining AI knowledge among physicians and medical students across 35 studies found that 74% reported a significant knowledge gap in AI fundamentals.3 Practicing interventionalists without institutional frameworks to fill this gap will need to pursue at least an intermediate level of self-directed education in order to contribute meaningfully to deliberative conversations about AI deployment in the cath lab and the broader healthcare environment.
In summary, AI is already deeply integrated within the cath lab. Practicing interventionalists and those currently in the training pipeline will need to educate themselves on the fundamentals of AI to be able to functionally appraise the next generation of clinical applications.
References
1. Khera R, Oikonomou EK, Nadkarni GN, et al. Transforming cardiovascular care with artificial intelligence: from discovery to practice. J Am Coll Cardiol. 2024;84(1):97–114. doi:10.1016/j.jacc.2024.05.003
2. Adler-Milstein J, Jha AK. HITECH Act drove large gains in hospital electronic health record adoption. Health Aff. 2017;36(8):1416–1422. doi:10.1377/hlthaff.2016.1651
3. Chen M, Zhang B, Cai Z, et al. Acceptance of clinical artificial intelligence among physicians and medical students: a systematic review with cross-sectional survey. Front Med. 2022;9:990604. doi:10.3389/fmed.2022.990604