Part 2 – Artificial Intelligence in the Cath Lab: A Pragmatic Current-State Analysis for the Practicing Interventional Cardiologist
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
 Jacob McAuliffe, MD is a cardiology fellow at Inova Schar Heart & Vascular in Falls Church, Virginia. He completed his residency training at Eastern Virginia Medical School. Prior to medical school, he completed a Master of Science & Technology Policy degree through the Consortium for Science, Policy, and Outcomes and worked as a Health Policy Fellow in Washington, D.C., cultivating an interest in advocacy, governance and responsible integration of emerging medical technologies into clinical practice. His scholarly and clinical interests converge at the intersection of interventional cardiology, health policy, and the responsible deployment of AI-enabled clinical tools.
Jacob McAuliffe, MD is a cardiology fellow at Inova Schar Heart & Vascular in Falls Church, Virginia. He completed his residency training at Eastern Virginia Medical School. Prior to medical school, he completed a Master of Science & Technology Policy degree through the Consortium for Science, Policy, and Outcomes and worked as a Health Policy Fellow in Washington, D.C., cultivating an interest in advocacy, governance and responsible integration of emerging medical technologies into clinical practice. His scholarly and clinical interests converge at the intersection of interventional cardiology, health policy, and the responsible deployment of AI-enabled clinical tools.
Disclosures: Dr. McAuliffe reports no conflicts of interest regarding the content herein.
Jacob McAuliffe, MD, can be contacted at Jacob.McAuliffe@inova.org
Read Part 1 – What is AI?
PART 2 – What Can AI Do?
Part 1 of this series established a working vocabulary and introduced foundational concepts related to AI, highlighting relevance to the cath lab. Building on that framework, this article surveys how AI applications are already empowering clinical care — and where they are headed — across the full spectrum of cath lab workflow.
III – Powerful, But Not Omnipotent
Beyond terminology, it is useful to think about AI in terms of functional categories — what these systems actually do — rather than how they are marketed.
The dominant paradigm for current cath lab AI applications is extractive utility: systems that identify, quantify, or classify patterns from captured data. These tools do not simply reproduce what a trained physician can observe; they harness information that is often physically imperceptible to the human eye or cognitively inaccessible at the scale and speed that modern procedural volumes demand. An algorithm that measures fractional flow reserve (FFR) from angiographic images draws on dozens of distributed geometric and hemodynamic features simultaneously across the coronary tree. Optical coherence tomography (OCT) analysis combines optical hardware with machine learning algorithms that, in a process unfolding in real time and remaining largely opaque to its internal mechanics, produces clinically actionable outputs: plaque characterization, lumen segmentation, and automated stent apposition maps. These represent the archetype of extractive AI in procedural cardiology as it is seen in practice today.
Generative AI operates differently. Rather than analyzing existing data to produce a classification or measurement (which can inform quantitative sizing or parameter recommendations), generative systems create entirely novel content. In the cath lab context, this readily includes examples such as AI-assisted procedural report generation or patient-facing documentation drafting. Generative AI is newer to clinical deployment and carries a distinct validation challenge: an extractive tool that is wrong produces what is in effect a number (and we treat patients, not numbers), while a generative tool that is wrong can produce a narrative or conclusion, one that may sound fluent and confident yet be inaccurate. This inaccuracy could be perpetuated if left uncorrected, propagating throughout the medical record through poorly disciplined copy-forward habits and referenced by other specialists.
Within these two broad use categories, three functional capacities deserve particular emphasis in the cath lab context. First, pattern recognition at superhuman scale: the ability to process imaging data with a consistency and throughput that human observers cannot replicate, particularly across repetitive analytical tasks at high procedural volumes. Second, real-time data adjudication: the synthesis of multimodal inputs (hemodynamic waveforms, angiographic and IVI data, biomarker and laboratory data) to support periprocedural clinical decisions and care delivery. Third, predictive modeling: the integration of complex, multivariable patient-level data to anticipate risk, guide triage, and inform procedural strategy from before a catheter is placed to after a procedure concludes.
Matching the functional type of AI to the clinical problem it is intended to address is not a technical nicety; it is the foundation of suitability assessments. It also informs risk assessments, a nuanced conversation beyond the scope of this article. Here are two quick examples of risk though. Example one: an extractive imaging tool validated on a specific angiographic platform in a European multicenter cohort may perform meaningfully differently on equipment from another vendor, in a different patient population, using different image acquisition protocols. Example two: a generative language model deployed for documentation requires a completely different validation framework compared to extractive applications, with considerations regarding the nature of its generated content, especially for patient-facing applications (i.e., tone, level of medical detail, gender consciousness, etc.). There are well-documented examples of racial and sociodemographic biases introduced and propagated through LLMs in healthcare settings. All four major commercially available LLMs were previously found to propagate race-based medical misconceptions in clinical scenarios, including perpetuating debunked race-based equations for estimating kidney function and lung capacity.4 These models similarly projected longer hospital stays and more optimistic survival estimates for white patients, reflecting real-world healthcare disparities embedded in training data.5
There is a dearth of guidance from reputable societies and/or regulatory agencies to inform general assessment of AI applications. Meaningful examples include the FDA’s AI/ML-Based Software as a Medical Device Action Plan,6 along with scientific statements from the American Heart Association addressing AI in cardiovascular imaging7 and AI in improving cardiovascular outcomes.8 These represent important starting points, though the field requires more prescriptive, specialty-specific guidance commensurate with the pace of clinical adoption. In the interim, the interventional cardiology community must build the analytical vocabulary to assess AI tools critically, develop institutional frameworks for evidence-informed adoption, and advocate for the specialty-specific guidance and regulatory standards that our patients require.
IV – AI Use Cases Across the Spectrum of Cath Lab Workflow
With this functional framework in mind, use cases for AI applications can be mapped across the three dominant phases of cath lab workflow: preprocedural planning, periprocedural decision and therapeutic delivery support, and postprocedural analysis and care.
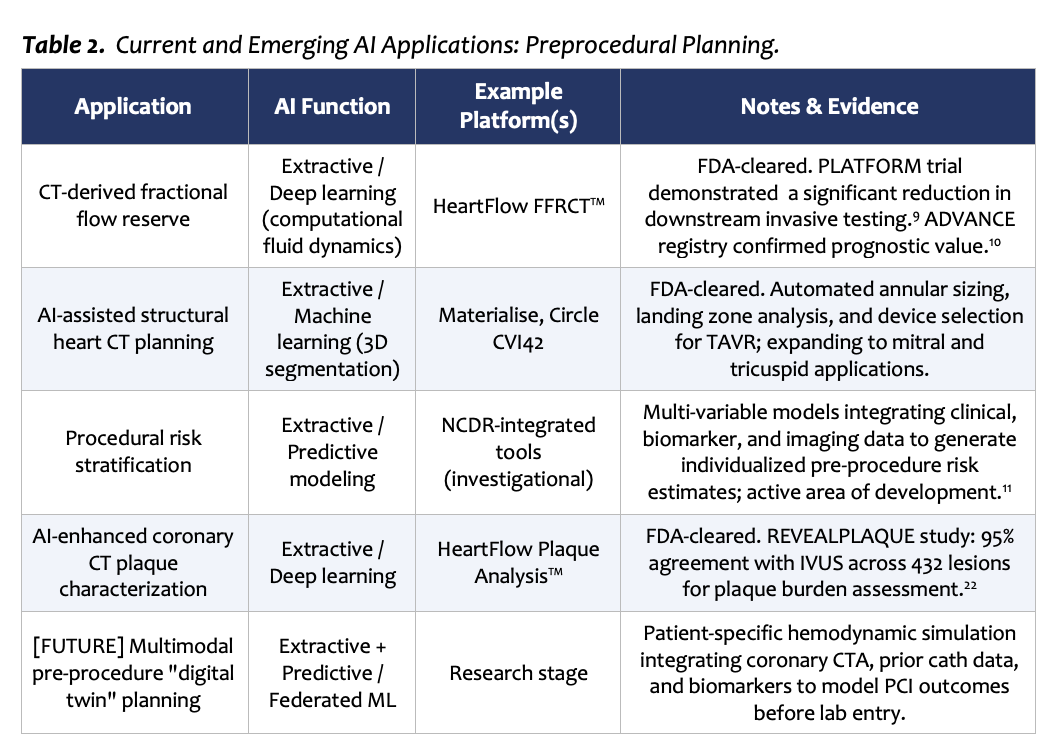
Preprocedural Planning
Some of the most validated AI applications in cardiology are those that inform decision-making before the patient enters the cath lab. HeartFlow’s FFRCT platform derives patient-specific coronary physiology from coronary computed tomography angiography (CTA) data, providing lesion-specific hemodynamic assessment without coronary instrumentation. The PLATFORM study demonstrated a significant, appropriate reduction in downstream invasive testing when FFRCT was incorporated into the diagnostic pathway.9 The ADVANCE registry subsequently confirmed its prognostic value across a large international cohort.10
For structural heart disease, AI-assisted CTA analysis platforms, including Materialise and Circle CVI42, support automated annular sizing, landing zone assessment, and device selection for transcatheter aortic valve replacement (TAVR) procedures. As the landscape of transcatheter mitral and tricuspid interventions continues to expand, compounded by the increasing sophistication of cardiovascular magnetic resonance (CMR) and positron emission tomography (PET) imaging modalities, the scope of imaging-based, AI-enhanced preprocedural planning is expected to grow substantially.
Risk stratification represents an evolving preprocedural use case. Machine learning models capable of integrating high-dimensional clinical, biomarker, and imaging data to generate individualized procedural risk estimates are in active development, with the maturation of National Cardiovascular Data Registry (NCDR)-level datasets serving as a primary substrate for model training.11
Periprocedural Decision and Therapeutic Delivery Support
The periprocedural space encompasses the use case domain that is arguably the most anticipated, while simultaneously harboring the highest degree of anticipated scrutiny. It is, however, already an area where ML-empowered tools have long been employed.
AI-derived FFR from invasive angiography, commercially available through CathWorks FFRangio and Medis QFR, among others, allows physiologic lesion assessment without the use of a pressure wire. The FAST-FFR trial, a prospective multicenter international study, demonstrated sensitivity and specificity of 93.5% and 91.2%, respectively, compared to wire-based FFR, with an overall diagnostic accuracy of 92%.12 The ALL-RISE randomized controlled trial subsequently demonstrated non-inferiority of Medtronic/CathWorks’ FFRangio to wire-based FFR for one-year major adverse cardiovascular events, with full results published in the New England Journal of Medicine in 2026.13
Intravascular imaging (IVI) represents the most established home for AI in the cath lab. Abbott’s Ultreon software, deployed through the OPTIS Next platform, empowers OCT to provide automated calcium detection, external elastic lamina identification, lumen and vessel segmentation, stent apposition analysis, and stent under-expansion flagging in near-real time.14 These advanced capabilities will only become more accurate. IVI platforms already function as in-room second opinions, and their sophistication with newer AI applications will see this role grow. It will be important for operators to understand the training and validation of their AI tools, just as an attending gauges the experience and capabilities of the fellows and residents in the room to ensure all members and equipment are being harnessed to their full and appropriate scope.
Hemodynamic monitoring is another domain where AI has already demonstrated success. The SmartAssist technology integrated into the Impella platform (Johnson & Johnson MedTech) enables real-time acquisition and display of hemodynamic parameters to support pump management and to set and trigger alarm parameters.15 This is a limited but illustrative example of AI’s capability to help manage mechanical circulatory support (MCS) and other platforms requiring critical, real-time assessment.
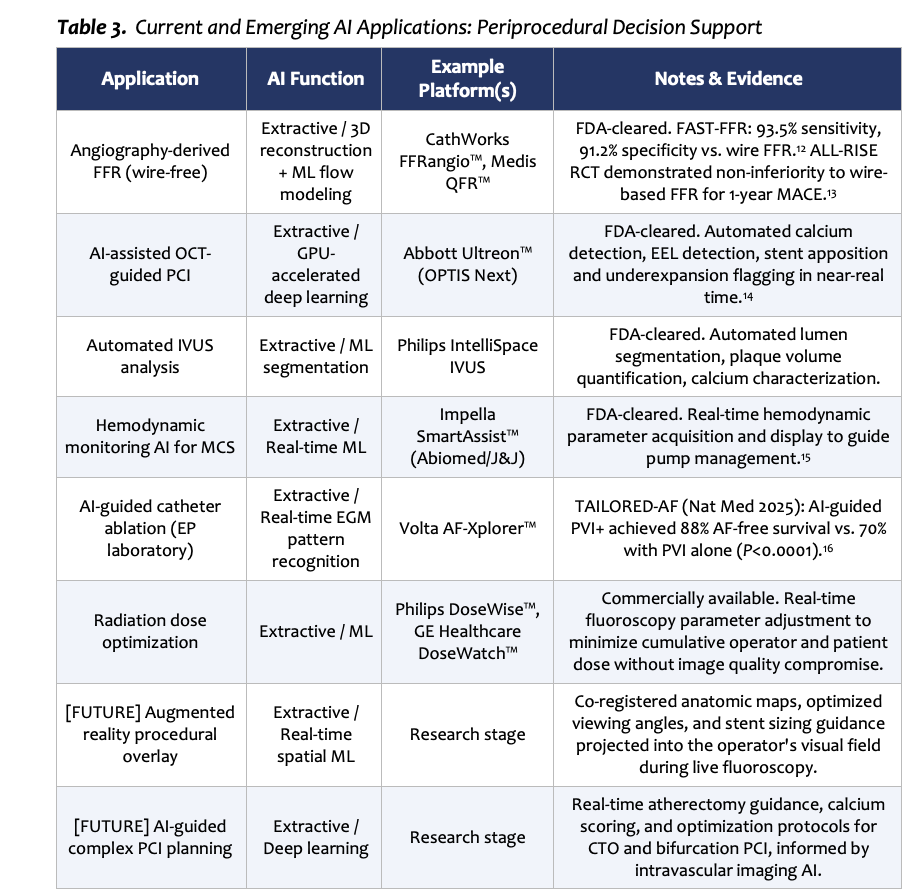 A landmark example of AI utilization to guide therapeutic delivery comes from our peers in the electrophysiology (EP) lab. The recently published TAILORED-AF trial was a multicenter, transatlantic, randomized clinical trial that evaluated Volta Medical’s AF-Xplorer, an AI-powered system designed to facilitate real-time identification of spatiotemporal dispersed electrograms (indicative of abnormal atrial conduction and a proposed marker for atrial tissue remodeling) to guide ablation targets beyond standard pulmonary vein isolation (PVI) in patients with persistent atrial fibrillation. Published in Nature Medicine in 2025, the trial demonstrated that AI-assisted ablation, in addition to PVI, achieved freedom from AF at 12 months in 88% of patients, compared with 70% in the PVI-only arm.16 TAILORED-AF stands as a compelling demonstration of what becomes possible when AI’s capacity for real-time complex data adjudication is coupled with the technical skills and expertise of a trained operator, a model directly parallel to the cath lab.
A landmark example of AI utilization to guide therapeutic delivery comes from our peers in the electrophysiology (EP) lab. The recently published TAILORED-AF trial was a multicenter, transatlantic, randomized clinical trial that evaluated Volta Medical’s AF-Xplorer, an AI-powered system designed to facilitate real-time identification of spatiotemporal dispersed electrograms (indicative of abnormal atrial conduction and a proposed marker for atrial tissue remodeling) to guide ablation targets beyond standard pulmonary vein isolation (PVI) in patients with persistent atrial fibrillation. Published in Nature Medicine in 2025, the trial demonstrated that AI-assisted ablation, in addition to PVI, achieved freedom from AF at 12 months in 88% of patients, compared with 70% in the PVI-only arm.16 TAILORED-AF stands as a compelling demonstration of what becomes possible when AI’s capacity for real-time complex data adjudication is coupled with the technical skills and expertise of a trained operator, a model directly parallel to the cath lab.
Postprocedural Analysis and Reporting
The postprocedural space is where generative AI is most visibly entering clinical workflows. Many health systems have already integrated LLM-based ambient documentation tools, such as Abridge and Nuance DAX, directly into their EMR platforms.17 Dictation microphones are a key example of a ML-enabled technology that has literally been in the palm of our hands for years. The latest generation of AI-enabled dictation software enables ambient, real-time transcription and automated structured note generation with remarkable accuracy. The benefit extends well beyond convenience. Accurate, structured, complete procedural documentation directly supports high-fidelity registry data for research and quality assurance, supports downstream risk stratification, and enhances longitudinal care management.
AI-driven models to guide contrast-associated AKI risk stratification represent a maturing postprocedural use case. These tools can integrate multivariate inputs such as baseline and serial renal function, contrast volume and administration frequency, hemodynamic trends reflecting periprocedural renal perfusion, body habitus, and concurrent nephrotoxin exposure, to generate individualized risk estimates that inform post-procedure management.
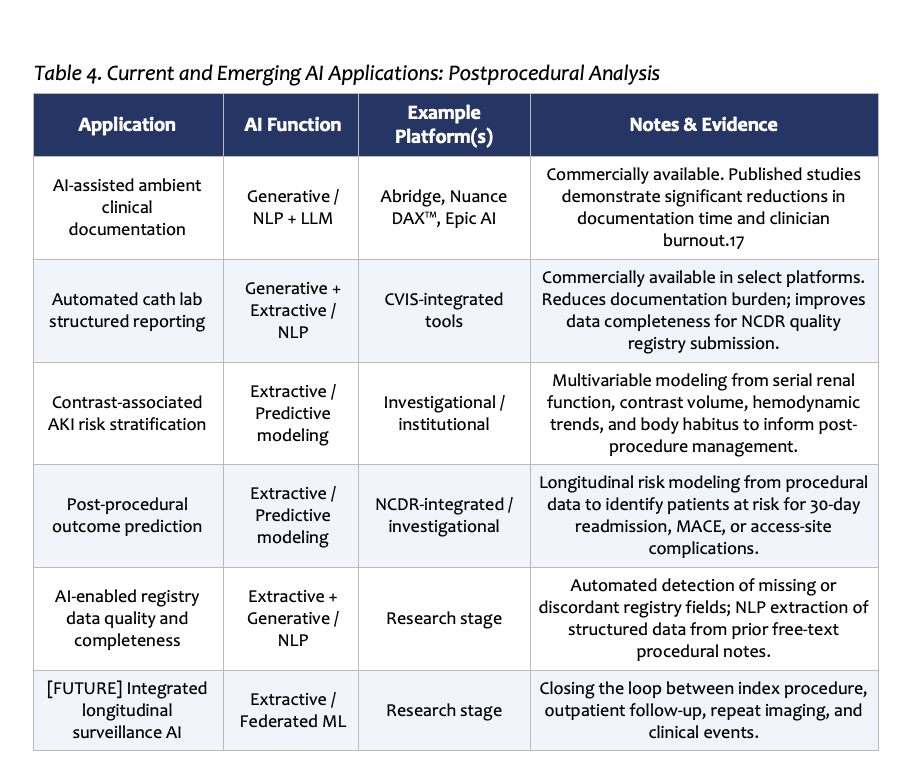 Outcome prediction tools integrated into cardiovascular information systems have the potential to close the longitudinal loop between procedural events and longer-term patient follow-up. This capability will mature substantially as registry-level, time-stamped datasets become available for model training. AI-enabled quality assurance applied to registry data itself — detecting missing fields, discordant entries, and extracting structured data from prior free-text procedural notes — represents a further application for AI tools to help meaningfully improve the integrity of the data substrate on which future AI tools will be trained.
Outcome prediction tools integrated into cardiovascular information systems have the potential to close the longitudinal loop between procedural events and longer-term patient follow-up. This capability will mature substantially as registry-level, time-stamped datasets become available for model training. AI-enabled quality assurance applied to registry data itself — detecting missing fields, discordant entries, and extracting structured data from prior free-text procedural notes — represents a further application for AI tools to help meaningfully improve the integrity of the data substrate on which future AI tools will be trained.
References
1. Khera R, Oikonomou EK, Nadkarni GN, et al. Transforming cardiovascular care with artificial intelligence: from discovery to practice. J Am Coll Cardiol. 2024;84(1):97–114. doi:10.1016/j.jacc.2024.05.003
2. Adler-Milstein J, Jha AK. HITECH Act drove large gains in hospital electronic health record adoption. Health Aff. 2017;36(8):1416–1422. doi:10.1377/hlthaff.2016.1651
3. Chen M, Zhang B, Cai Z, et al. Acceptance of clinical artificial intelligence among physicians and medical students: a systematic review with cross-sectional survey. Front Med. 2022;9:990604. doi:10.3389/fmed.2022.990604
4. Omiye JA, Lester JC, Spichak S, et al. Large language models propagate race-based medicine. NPJ Digit Med. 2023;6:195. doi:10.1038/s41746-023-00939-z
5. Yang Y, Liu X, Jin Q, Huang F, Lu Z. Unmasking and quantifying racial bias of large language models in medical report generation. Commun Med. 2024;4:202. doi:10.1038/s43856-024-00601-z
6. U.S. Food and Drug Administration. Artificial Intelligence/Machine Learning (AI/ML)-Based Software as a Medical Device (SaMD) Action Plan. January 2021. Accessed June 9, 2026. Available at: https://www.fda.gov/media/145022/download.
7. Hanneman K, Playford D, Dey D, et al. Value creation through artificial intelligence and cardiovascular imaging: a scientific statement from the American Heart Association. Circulation. 2024;149(6):e296–e311. doi: 10.1161/CIR.0000000000001202
8. Armoundas AA, Narayan SM, Arnett DK, et al. Use of artificial intelligence in improving outcomes in heart disease: a scientific statement from the American Heart Association. Circulation. 2024;149(14):e1028–e1050. doi:10.1161/CIR.0000000000001201
9. Douglas PS, De Bruyne B, Pontone G, et al. 1-year outcomes of FFRCT-guided care in patients with suspected coronary disease: the PLATFORM study. J Am Coll Cardiol. 2016;68(5):435–445. doi:10.1016/j.jacc.2016.05.057
10. Patel MR, Nørgaard BL, Fairbairn TA, et al. 1-year impact on medical practice and clinical outcomes of FFRCT: the ADVANCE registry. JACC Cardiovasc Imaging. 2020;13(1):97–105. doi:10.1016/j.jcmg.2019.03.003
11. Niimi N, Shiraishi Y, Sawano M, et al. Machine learning models for prediction of adverse events after percutaneous coronary intervention. Sci Rep. 2022;12:6262. doi:10.1038/s41598-022-10346-1
12. Fearon WF, Achenbach S, Engstrøm T, et al. Accuracy of fractional flow reserve derived from coronary angiography (FAST-FFR). Circulation. 2019;139(4):477–484. doi:10.1161/CIRCULATIONAHA.118.037350
13. Fearon WF, Kirtane AJ, Jeremias A, et al. Angiography-derived fractional flow reserve to guide PCI (ALL-RISE). N Engl J Med. 2026. doi:10.1056/NEJMoa2600949
14. Abbott Vascular. Ultreon™ software for OCT intravascular imaging. Abbott Laboratories; 2025. Accessed June 9, 2026. Available at: https://www.cardiovascular.abbott/us/en/hcp/products/percutaneous-coronary-intervention/intravascular-imaging/ultreon-software.html
15. Consolo F, Tessari M, Morici N, et al. The intelligent Impella: future perspectives of artificial intelligence in the setting of Impella support. ESC Heart Fail. 2024. doi:10.1002/ehf2.14865
16. Deisenhofer I, Albenque JP, Busch S, et al. Artificial intelligence for individualized treatment of persistent atrial fibrillation: a randomized controlled trial (TAILORED-AF). Nat Med. 2025;31(4):1286–1293. doi:10.1038/s41591-025-03517-w
17. Olson KD, Meeker D, Troup M, et al. Use of ambient AI scribes to reduce administrative burden and professional burnout. JAMA Netw Open. 2025. doi:10.1001/jamanetworkopen.2025.34976