



Reducing Stress: The Challenges of EMS SIM Labs
Simulation (SIM) is used to teach new techniques, the application of new devices, to develop students and staff through various scenario-based interactions. The final evaluation process determines if students are prepared to move on in a program or to employment through scaffolding and congruence of educational content.1-3 The quality of simulation has grown. Yhe first EMS simulations used a separate intubation head, IV arms, coupled with a CPR manikin. These “FrankenManikins” were replaced with next generation models where students could perform all of these skills, with connections for rhythm generators and defibrillation, on one manikin. SIM manikins now are of such an incredible quality that it’s staggering not only in the procedures that can be performed, but the physiologic responses that can be presented.
The use of SIM has helped improve the quality of clinical care for entry level student as well as new hires, helping to maintain competencies and evaluate prospective staff. Ask any educator during COVID when clinical experiences were limited—SIM was important to the success of not only their program but to their student.4-5
SIM shouldn’t be an exercise in intimidation; this attitude is counterproductive. The stress and anxiety associated with SIM will degrade its ability and worth associated with any type of formative development or summative assessment.6-7 If used in a hiring process, it may screen out qualified candidates.6-8
Building Confidence and Muscle Memory
With SIM, we develop muscle memory through repetition, we build confidence, we practice once in a lifetime scenarios, and we are work through the patient who is “crashing.” We want to fail, make mistakes during a SIM, so that we’re better prepared for the field. Practice makes perfect. This is where SIM thrives. If your organization has an inexperienced workforce, this is critically important. The SIM lab is the gym where we’re going to work our clinical skills. Instead of dumbbells we use the SIM manikin to build our mind (cognitive) and train our muscles (psychomotor).8-9
Most of what we need to do in this regard is in the mental process of how we approach SIM. You control this dynamic as the educator. Shift the narrative. During the pre-brief tell students that success is identifying one thing to improve. Reinforce effort and problem-solving over perfection.9 Avoid “gotcha” or convoluted scenarios. You can use more complex, challenging scenarios, but only later in the education journey. The process should feel developmental, not punitive. Your teacher didn’t rollout quadratic equations your first day in kindergarten. Education is about congruence, the natural sequence of things and how they relate to one another, and scaffolding, starting with a strong base and then building on each layer.2-3
Introduce students to the manikin. Start off with low-stress presentations, just like warm-ups if you are getting ready to workout. Single-practice skills such as opening an airway, assessing lung sounds, IV’s, intubation should be done one-on-one, just you and the person working through the scenario, without any observers. It reduces stress, and people don’t feel like all eyes are on them if they make a mistake.
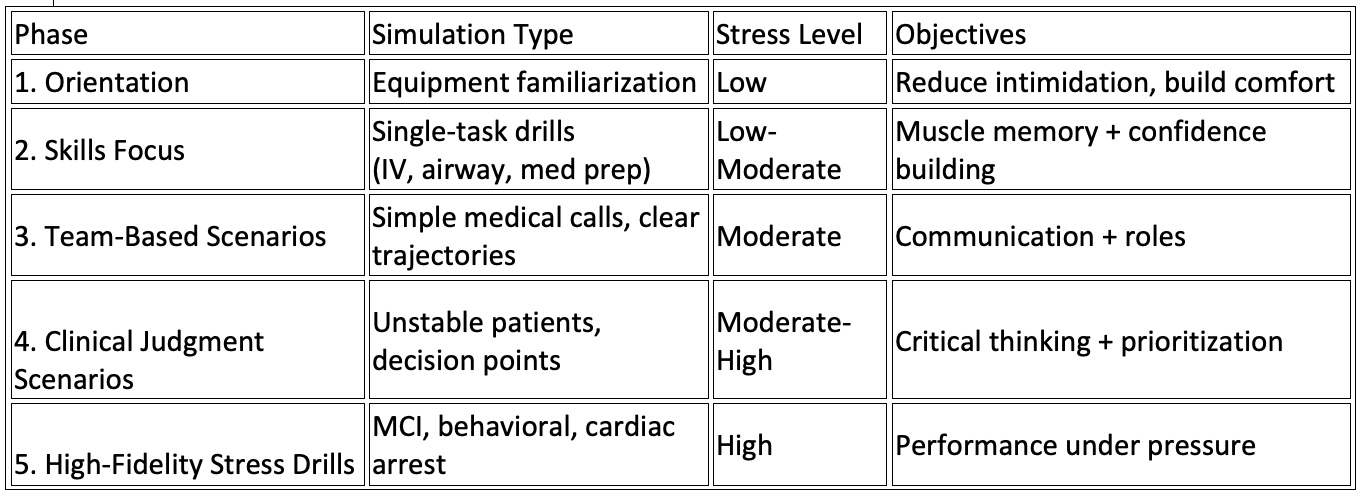
Here is a sample framework from 1 to 5 levels, representing each phase, by simulation type, stress level, and objectives that you could use as you gradually build confidence, reduce anxiety and stress.
When your EMS clinician is ready, after they have performed one-on-one skills labs using the SIM, begin to integrate team-based skills. People feel safer when they’re not alone. You know who your less experienced EMS clinicians are. Pair them with stronger partners at first. Reinforce communication, “Talk to me Charlene, tell me what’s happening?” especially when it applies to decision-making. “What do you think we need to do?” or “Is this patient a candidate for TXA?” and have those quick, brief discussions. Let them rotate roles to build competence gradually. This author had a partner, Tommy, and we would always tell each other, no matter how bad the call, “You are not alone, I have your back you have mine.” When it comes to SIM it’s the same thing; that shared responsibility with your partner lowers anxiety.
Incorporate Fun
Try and make the SIM man feel more human. Some organizations pick out names for the manikins. They dress them in old t-shirts, sportswear, and baseball caps. One program had the daughters of the instructors make friendship bracelets. Decorate the SIM space with posters and furniture. Jennifer McCarthy MAS, NRP, CHSE-A, FSSH, Director of Simulation and Clinical Associate Professor at Seton Hall University, develops EMS SIM competitions, and her simulations are as diverse as a bar, an outdoor barbecue, or car wreck, with all the props. Give the person who is going to work through the scenario a brief backstory, age, job, emotional cues. When the manikin feels like a person, people relax, like this is a normal call.
Shubik, an early academic who worked on game theory, talked about having fun to enhance learning.12-14 In that same spirit, have fun; invent games with your simulations. Timed challenges, such as securing an airway via intubation as fast as you can. CPR relay. Give out rewards. Provide positive reenforcement.
Instructor modeling is important, in the classroom, in the field, and in the SIM lab. Show vulnerability, demonstrate a scenario, and make intentional minor mistakes. Everyone is looking at you as their leader because you’re the teacher. As you work your way through the scenario, narrate your thinking, including uncertainty. When they see you do that, you give them permission to try and fail without fear. It lets them know it’s a shared experience and reduces shame. If the people you are bringing in to educate feel safe, respected, and supported, they’ll lean in.
Get it into their heads that you think of SIM as the “gym” of EMS. The goal isn’t to impress anyone, it’s to get stronger. Simulation anxiety is normal and expected. Consistently communicate that our goal is growth, not judgment.
How You Debrief Matters
Remember to debrief with psychological safety.10-11 It’s quick and supportive. It isn’t criticism or picking apart every detail. Be inviting; start off with “What went well?” This gives the EMS clinician control over the debrief and inspires confidence. Follow that up with “Great, now why don’t share what you would do different next time?” Most of the time they know what they need to do better, and it allows them to acknowledge this, but most important, it’s psychologically safe; you’re allowing them a measure of control here. They can proceed at their own pace.10-11 Reflection is just as important in the SIM lab as it is in the classroom.
You can make suggestions, but frame it with “those are all great points, tell us what else you could do…” You are providing validity to what they told you, plus you are giving them additional information to reflect on.10-11 It’s important to be specific when providing feedback for SIM, for example, “I like how you communicated clearly with your partner,” or “your lung sound assessment was very detailed. You listened through the respiratory cycle and told the patient to breath in and out with their mouth open.” This focuses on affective and psychomotor behavior and that feedback is critical to reinforcement.
Basic Rules for Psychological Safety:
1. Confidentiality is key: Performance stays in the SIM room
2. Mistakes are welcome, we learn through error.
3. Respect maintained: No shaming or sarcasm in the SIM room
What are the rules for the SIM lab? Can your students stop and ask questions? Do you encourage them to think out loud?
You should have a short briefing and debriefing script that is meant to define the SIM experience and reduce anxiety and stress. Read it before the simulation begins and after the scenario is complete.11 Post the rules on the walls of the SIM lab so that everyone can see them (Click here for a downloadable scripts and copy of sample SIM lab rules https://bit.ly/SimScript). Allow everyone to express how they felt, and most importantly identify that one thing they need to improve. No one should walk out of the room feeling as if they failed. They should feel as if they had an intense workout in the gym; they should feel confident because they had the opportunity to perform skills they rarely perform; and they should feel that camaraderie that comes from working together as a team, something we try hard to instill in all of our EMS clinicians.
SIM is not an obstacle to be feared; it’s the path to mastery. It can be used for summative evaluations, but it should be approached with care and forethought. When we intentionally design SIM experiences around psychological safety, graduated challenge, deliberate practice, and supportive debriefing, we reclaim SIM: a protected space where clinicians are allowed to struggle, reflect, and grow. As EMS educators, we don’t simply teach procedures, we are shaping identities, confidence, and professional courage. If we shift the culture from punishment to purpose, from judgment to development, and from intimidation to invitation, simulation becomes the gym of EMS once again: a place where clinicians show up imperfect, leave stronger, and return eager to train. The true measure of a successful SIM lab is not flawless performance in the room, but safer, more thoughtful, more resilient clinicians in the field, and that responsibility rests squarely with us.
References
- Bloom, B. S. (Ed.). (1956). Taxonomy of educational objectives: The classification of educational goals. Handbook I: Cognitive domain. David McKay Company.
- Ormrod, J. E. (2016). Human learning (8th ed.). Pearson.
- Price, K. M., & Nelson, K. L. (2018). Planning effective instruction: Diversity responsive methods and management. Cengage Learning
- Rojo-Rojo, A., Maestre, J. M., del Moral, I., Roldán, J. L., & Ayuso, D. (2021). Training with high-fidelity clinical simulation for emergency and ICU teams in the care of COVID-19 patients: A mixed pilot study. Journal of Clinical Medicine, 10(21), 4923. https://doi.org/10.3390/jcm10214923
- Walker, A., McNally, K., & Ganti, L. (2024). Impact of virtual simulation to teach EMS personnel respiratory failure management during the COVID-19 pandemic. Academic Medicine & Surgery, 6(1), 1–9.
- Stein, C., Hiemstra, L. A., Louw, Q. A., & Strydom, C. (2020). The effect of clinical simulation assessment on stress and anxiety in emergency care students. PLoS ONE, 15(3), e0230731. https://doi.org/10.1371/journal.pone.0230731
- Barbadoro, P., Moretti, F., Piroddi, C., De Sio, S., Ricciardi, W., & La Torre, G. (2023). Stress responses in high-fidelity simulation and standard simulation for healthcare students: A quasi-experimental study. Scientific Reports, 13, 2067. https://doi.org/10.1038/s41598-023-29233-9
- Våge, G., Gormley, G., McKeown, P., & Hamilton, D. (2024). Simulate to stimulate? A systematic review of simulation-related stress and learner performance. Medical Education, 58(1), 28–41. https://doi.org/10.1111/medu.15293
- Violato, E., Virostek, L., Ragasa, J. P., Lewis, M., & Violato, E. (2025). A systematic review of the evidence for using simulation to replace clinical experience for paramedic students. International Journal of Paramedicine, (9), 30–42. https://doi.org/10.56068/GXSE4776
- Konzelmann, J. (2024). A literature supported model for implementing effective use of simulation and debriefing in paramedic education. International Journal of Paramedicine, (8), 205–215. https://doi.org/10.56068/GWRR2621
- Bienstock, J., Heuer, A., & Zhang, Y. (2023). Simulation-based training and its use amongst practicing paramedics and emergency medical technicians: An evidence-based systematic review. International Journal of Paramedicine. https://doi.org/10.56068/VWHV8080
- Shubik, M., 1978. Opinions on how to play some simple games. Simulation and Games. 9: 67-88
- Hausner, M., J. Nash, L. Shapley and M. Shubik, 1964. “So Long Sucker: A Four-Person Game” in M. Shubik (ed.), Game Theory and Related Approaches to Social Behavior. New York: Wiley, pp. 359–361
- Shubik, M. (2001). The uses of teaching games in game theory classes and some experimental games (Cowles Foundation Discussion Paper No. 1542). Cowles Foundation for Research in Economics, Yale University. https://elischolar.library.yale.edu/cgi/viewcontent.cgi?article=2541&context=cowles-discussion-paper-series






