Atrial Lead Failure Secondary to Hemostatic Surgical Clip Entrapment
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2025;25(9):8-10.
Aimee E Willett, DO; Wesley F Kim, MD; Ankur Shah, DO; Anish Amin, MD
OhioHealth Riverside Methodist Hospital, Columbus, Ohio
Pacemaker leads are resilient with built-in fail-safes designed to prevent and detect potential complications during implantation and use. Common mechanisms to ensure early pacemaker lead dysfunction detection include remote device monitoring, algorithm-based prediction, and regular device interrogations.1 Transvenous device leads also undergo rigorous evaluation in preclinical testing to assure long-term durability. Despite these efforts, some leads inevitably experience mechanical breakdown, dislodgement, and infection.1 A less common and unpredictable etiology of pacemaker lead dysfunction is iatrogenic injury. When it occurs, lead failure can result in sequelae including inappropriate shock, incorrect pacing, or arrhythmia generation, leading to undesirable patient outcomes. Management for pacemaker lead failure involves prompt repositioning, removal, or extraction of malfunctioning leads depending on the underlying cause.
This report highlights a unique etiology, diagnostic evaluation, and management of iatrogenic atrial lead failure secondary to hemostatic surgical clip entrapment. We
highlight a systematic approach to lead malfunction that emphasizes the importance of device interrogation, chest radiography, and clinical context consideration to build a differential diagnosis.2 Additionally, we emphasize the importance of recognizing that cardiac implantable electronic devices (CIEDs) are susceptible to malfunction and damage after open-heart surgery; therefore, close postoperative monitoring should be considered in these patients.
Case Presentation
A 77-year-old man presented with complete heart block in the setting of known aortic insufficiency and mitral regurgitation. At the time of presentation, valvular intervention was not indicated. As such, a conduction system pacemaker was implanted via the left axillary vein using a CapSureFix Novus MRI SureScan Pacing Lead (model 5076, Medtronic) in the right atrial (RA) position and SelectSecure MRI SureScan Pacing Lead (model 3830, Medtronic) using a preshaped sheath (C315 Delivery Catheter, Medtronic) in the left bundle branch area (LBBA) position. Sensing at the time of implant was 4.7 mV in the RA lead and 10.8 mV in the LBBA lead. Thresholds were stable below 1 V @ 0.4 ms for both leads.
Two months following pacemaker implant, the patient was recommended to undergo valvular surgery. He underwent aortic valve replacement using a 25-mm Inspiris Resilia
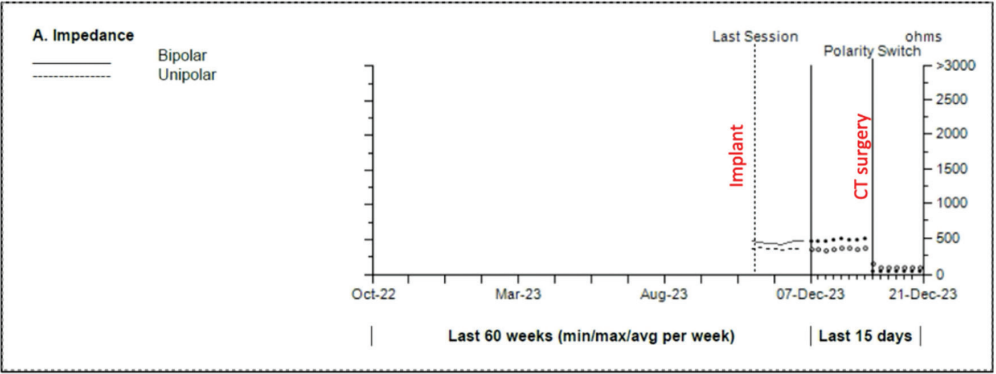
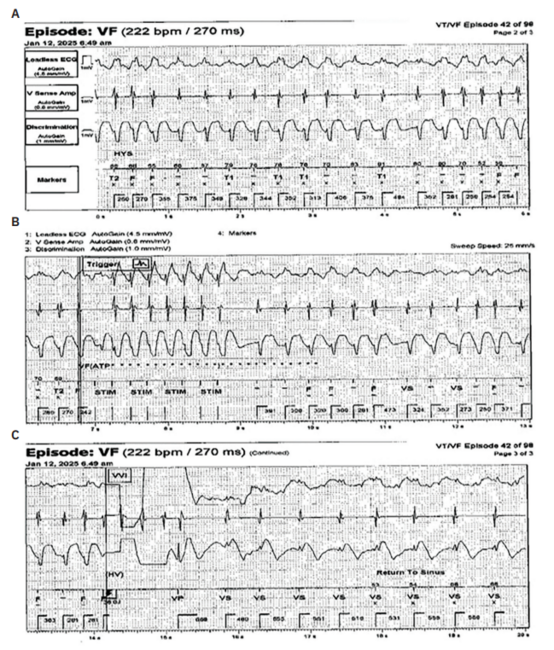
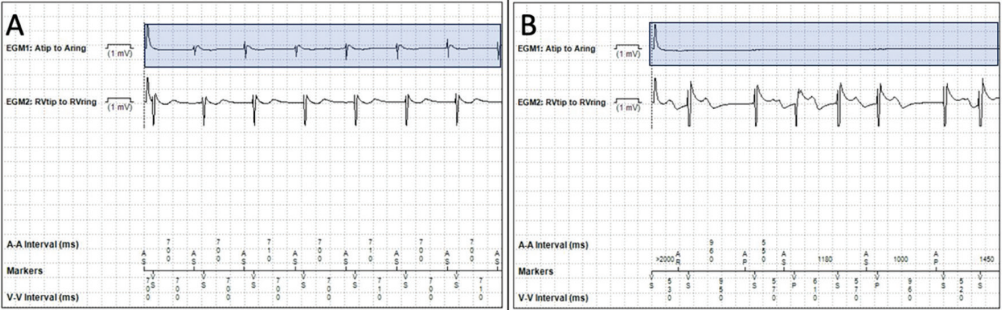
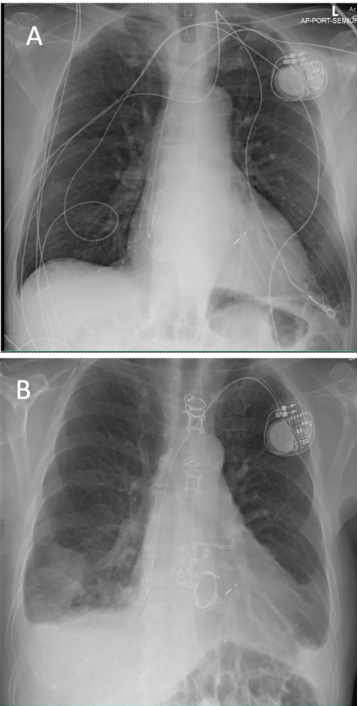
Aortic Valve and posterior chordal-sparing mitral valve replacement using a 31-mm valve (Edwards Lifesciences) without complications. After his surgical recovery, the patient presented to device clinic follow-up for routine pacemaker monitoring. Evaluation showed lack of atrial sensing and no atrial electrograms (Figure 1). A concurrent decrease in atrial unipolar and bipolar lead impedance from 400 ohms to <100 ohms (Figure 2) was also noted. This initial evaluation was consistent with oversensing and possible lead dislodgement. Given these concerns, a chest radiograph was obtained, which confirmed stable lead position without obvious dislodgement (Figure 3). Atrial lead revision was recommended for diagnostic and therapeutic purposes.
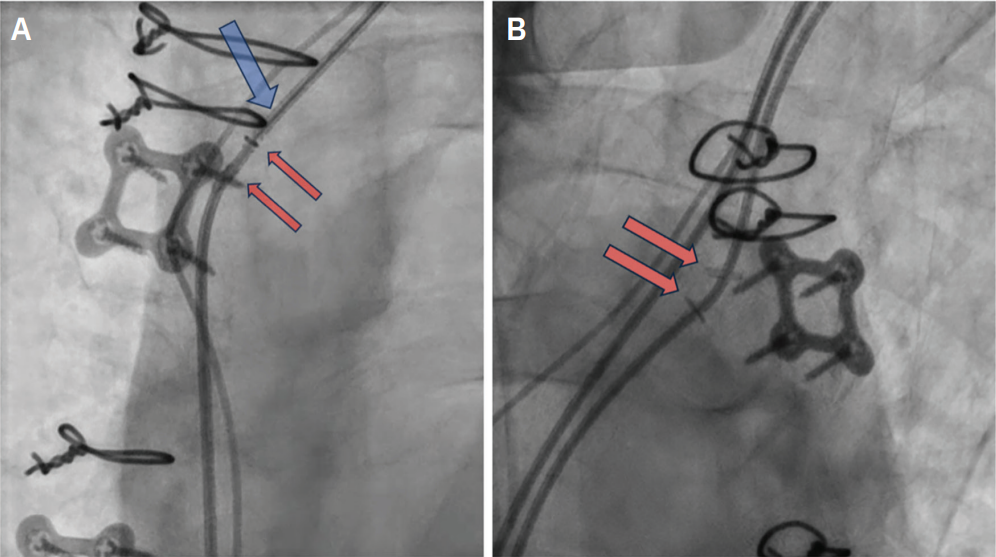
During revision, the stylet encountered resistance along the atrial lead (Figure 4, blue arrow). Fluoroscopic imaging revealed 2 radiopaque clips adhered to the lead
(Figure 4, red arrows). Figure 4B also clearly shows the hemostatic clips. These clips were determined to be the cause of the resistance encountered by the stylet; they were noted to be compressing the atrial lead in the brachiocephalic vein proximal to the superior vena cava junction. The clips were identified as metal hemostatic surgical clips inadvertently placed around the lead during the patient’s valvular surgery. Lead extraction was deferred as the hemostatic clips were extravascular in position. A new atrial lead was successfully placed with no complications and stable parameters. The old atrial lead was capped and abandoned. At 6-month follow-up, the device interrogation was stable with the new atrial lead.
Discussion
A thorough investigation is important when considering and identifying rare etiologies of lead failure, including iatrogenic hemostatic surgical clip entrapment. Notable aspects of device interrogation relevant to this case include absence of atrial electrogram tracings, oversensing on the atrial marker channel, and drastic changes in impedance.
Oversensing can result from nonphysiologic currents sensed by the pacing system leading to atrial pacing inhibition along with impaired current conduction along the atrial
lead. The differential diagnosis for oversensing includes lead mechanical breaks or fractures, lead fixation dislodgement, and device-related infection.2 Correction of oversensing can be completed by reducing atrial sensitivity, changing timing periods, or changing sensing polarities. Despite these interventions applied in this case, no atrial signal was detected by the device in any configuration.
Pacemaker impedance describes the structural integrity and electrical performance of leads. Decreases in impedance measurements are consistent with lead insulation breeches, which introduce a second current pathway in parallel to the circuit. Impedance for this patient dropped to below <100 ohms after his surgical intervention, which raised concerns for either lead dislodgement or insulation failure.3 Chest radiography was used to evaluate and showed a stable atrial lead with normal slack. Due to this unremarkable finding, the authors proceeded with lead revision, which showed the entrapment of the lead due to hemostatic clips.
This case highlights a unique cause of atrial lead failure due to inadvertent lead entrapment from surgical hemostatic clips. Device-related complications post open-heart surgery have been reported, with a tenfold risk within 6 months of surgery.4 Atrial leads are the most impacted due to the need for right atrial appendage cannulation for cardiopulmonary bypass. In this case, the ascending aorta was accessed, and the clips were used for hemostasis at the conclusion of the case. The brachiocephalic vein was inadvertently clipped during the process, thereby entrapping the atrial lead. Hemostatic clips are widely used in all types of surgical interventions from general, cardiothoracic, and even endoscopic procedures. Hemostatic clips allow operators to reliably ligate blood vessels during open-heart surgery.5 Hemostatic clips do not dissolve when applied and are at risk for potential dislodgement or damage to the structure applied.
Summary
Atrial lead failure secondary to iatrogenic hemostatic surgical clip entrapment, as identified in our review, has not been reported as a postoperative complication from open-heart surgery. We hope this adds to the literature of known device-related malfunctions from cardiothoracic surgery and brings insight to operators using hemostatic clips in patients with CIEDs.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Drs Willett, Kim, and Shah report no conflicts of interest regarding the content herein. Dr Amin reports grants or contracts from Abbott and Biosense Consulting (medical advisory), Medtronic and Boston Scientific (consulting, medical advisory, and research support), Philips (honoraria and research support), and Biostar (equity); consulting fees from Abbott, Johnson & Johnson MedTech, Medtronic, and Boston Scientific, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Philips; participation on a medical advisory board from Abbott, Johnson & Johnson MedTech, Medtronic, and Boston Scientific; stock or stock options from Biostar; and other financial or non-financial interests from Medtronic, Boston Scientific, and Phillips (research support).
References
1. Nair SG, Swerdlow CD. Monitoring for and diagnosis of lead dysfunction. Card Electrophysiol Clin. 2018;10(4):573-599. doi:10.1016/j.ccep.2018.07.004
2. Safavi-Naeini P, Saeed M. Pacemaker troubleshooting: common clinical scenarios. Tex Heart Inst J. 2016;43(5):415-418. doi:10.14503/THIJ-16-5918
3. Ellenbogen KA, Wilkoff BL, Kay GN, Lau CP, Auricchio A, eds. Clinical Cardiac Pacing, Defibrillation, and Resynchronization Therapy. Elsevier; 2017.
4. Frausing MHJP, Nielsen JC, Johansen JB, et al. Lead complications after cardiac surgery in patients with cardiac implantable electronic devices. Eur J Cardiothorac Surg. 2022;62(2):ezac318. doi:10.1093/ejcts/ezac318
5. Mehra S, Clymer JW, Ricketts CD. A review and comparison of vessel ligation with Ligaclips. J Surg. 2022;7:1660. doi:10.29011/2575-9760.001660
Related Content