

Shock to the Heart: A Case of Holiday Heart With Recurrent Arrhythmias in a Patient With Alcohol Use Disorder and an Implantable Cardioverter-Defibrillator
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2026;26(5).
Bilal Niazi, BS1; Demetra Menoudakos, BS1; Ermin Tale, DO2; Todd Cohen, MD1
1New York Institute of Technology College of Osteopathic Medicine, Old Westbury, New York;
2Jacobi Medical Center/Albert Einstein College of Medicine, Bronx, New York
The cardiovascular effects of alcohol consumption, both acute and chronic, have been extensively studied.1 In 1978, Ettinger and colleagues first described the association between heavy alcohol intake and cardiac arrhythmias in a case series of 24 patients, coining the term “holiday heart” syndrome.2 This phenomenon is most commonly associated with paroxysmal atrial fibrillation (AF) following episodes of binge drinking; however, more significant arrhythmias, including ventricular tachycardia (VT) and ventricular fibrillation (VF), have also been reported.3
In patients with structurally normal hearts, episodes of holiday heart are typically self-limited and may require only supportive care.4 In contrast, patients with underlying cardiac disease or an implantable cardioverter-defibrillator (ICD) may experience more complicated clinical courses, including recurrent arrhythmias and inappropriate device therapies. This case describes recurrent alcohol-induced arrhythmias in a patient with a single-chamber ICD resulting in multiple shocks, illustrating the challenges of arrhythmia discrimination, patient adherence, and long-term management in this population.
Case Presentation
A 54-year-old man was referred for cardiac electrophysiology (EP) evaluation to establish care for management of an ICD. His medical history was notable for chronic alcohol abuse, AF, VT, and tachycardia-induced cardiomyopathy. The patient reported that he had not been evaluated by an electrophysiologist for several years and had previously undergone 2 ablation procedures (type uncertain). Additionally, the patient had a single-chamber implantable cardioverter-defibrillator (Fortify Assura VR model 1357-40Q, Abbott) in situ that was implanted approximately 8 years earlier.
At the initial visit, the patient reported feeling well but described prior episodes of palpitations associated with alcohol consumption, some of which were accompanied by ICD shocks. He reported consuming 5 to 8 shots of vodka multiple times per week over the preceding year, with the exception of the week prior to presentation, during which he remained abstinent.
Current medications included rivaroxaban 20 mg daily and metoprolol succinate 50 mg daily; however, the patient reported nonadherence to metoprolol over the preceding year. He was hemodynamically stable and denied chest pain, palpitations, dyspnea, edema, or presyncope/syncope.
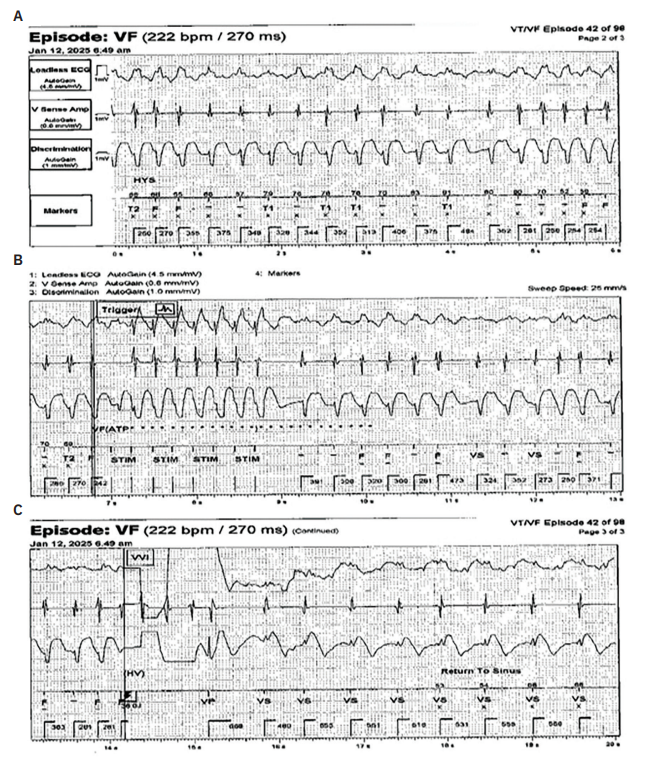
Device interrogation showed 91 recorded arrhythmic episodes over a 9-month period. Most treated episodes appeared consistent with AF with rapid ventricular response (Figure 1A), though definitive discrimination was limited by the presence of only a single ventricular lead, and episodes of nonsustained VT could not be conclusively excluded.
Antitachycardia pacing (ATP) was automatically delivered based on programmed rate criteria, followed by shocks when necessary (Figures 1B and 1C). Device programming included a VT-1 monitor-only zone at ≥150 bpm, a VT-2 zone at ≥181 with ATP ×3 followed by shocks of 36 J and 40 J ×3, and a VF zone at ≥222 bpm with ATP ×1 followed by shocks of 36 J and 40 J ×5. In some instances, these therapies resulted in conversion from AF to normal sinus rhythm. Since the supraventricular (SVT) discriminators were programmed on for at least 3 years, the patient received 55 ATP therapies and 24 shocks. He had not activated remote device monitoring during most of his care.
Transthoracic echocardiography demonstrated normal left ventricular ejection fraction (ejection fraction >55%) with moderate left atrial enlargement. Computed tomography angiography and stress testing were unremarkable. Medication adherence was emphasized, and the patient agreed to resume metoprolol succinate at an increased dose of 100 mg daily. Rivaroxaban was continued, and after extensive counseling, he was referred to Alcoholics Anonymous.
Initial follow-up suggested adherence to sobriety, with participation in Alcoholics Anonymous, as well as adherence to his prescribed medical regimen. Repeat in-office device interrogations demonstrated occasional episodes of paroxysmal AF with rapid ventricular response, without new ICD shocks or ATP therapies.
Despite efforts to address his substance use disorder, the patient subsequently relapsed into binge drinking and became medically nonadherent. He missed multiple cardiology and device follow-up appointments, and attempts to contact him were unsuccessful. After approximately 3 months of complete nonadherence, a remote device interrogation performed during an emergency department visit at an outside hospital revealed 13 episodes of rapid AF, with 3 shocks delivered in rapid succession. The device had reached elective replacement indication, and the outside institution performed ICD generator replacement and assumed ongoing care.
Discussion
Heavy alcohol consumption associated with cardiac arrhythmias is characteristic of holiday heart syndrome. Alcohol can provoke AF as well as VT and VF.5 Sustained alcohol abstinence can significantly reduce arrhythmia burden;6 however, cardiac management in patients with alcohol use disorder is complex and highly dependent on adherence and willingness to implement lifestyle modifications.
Prior to establishing care, the patient demonstrated poor medical adherence and engaged in regular binge drinking. ICD interrogation revealed a high burden of tachyarrhythmias requiring ATP pacing and shocks. Lack of adherence to remote monitoring delayed recognition of escalating arrhythmia burden and recurrent ICD therapies, potentially precluding earlier intervention. Remote monitoring is effective for detecting arrhythmia recurrence and, in patients without alcohol use disorder, often prompts timely electrophysiologic intervention. In patients with alcohol use disorder who engage in binge drinking, particularly those who are nonadherent, the appropriateness of ICD therapy may be questioned.7,8
Cohort studies have demonstrated that recurrent ICD shocks may promote avoidance of behaviors perceived to be associated with shock delivery.9 However, ICD shocks are also known to provoke significant anxiety and anticipatory distress, with evidence from addiction research suggesting that individuals with substance use disorders may continue maladaptive behaviors despite adverse consequences, reflecting altered negative reinforcement learning and impaired sustained avoidance.10 In this case, binge drinking and the associated ICD therapies initially motivated the patient to reengage with EP care; however, he ultimately failed to modify his behavior and experienced recurrent shocks, leading to earlier battery depletion of his device then if he did not experience holiday heart. This presentation contrasts with a prior report of holiday heart syndrome in a patient with an ICD, in which shock delivery served as an effective deterrent to continued alcohol consumption.11 Our case instead illustrates a shock–anxiety–relapse cycle, in which shock-related distress transiently promotes engagement and intent to change, but is followed by relapse rather than sustained behavioral avoidance.
Despite activation of all available discrimination algorithms, this single-chamber ICD failed to consistently distinguish appropriate therapies for VT or VF from inappropriate therapies related to AF or SVT. The absence of an atrial lead precluded atrioventricular discrimination, which may have improved arrhythmia classification and reduced inappropriate therapies. Device selection in complex patients requires careful consideration of ICD type—subcutaneous, single-chamber, or multichamber—as well as programming strategies to optimize discrimination between ventricular and supraventricular arrhythmias, particularly in individuals with factors that may increase arrhythmia burden or limit longitudinal follow-up.
Despite delivery of at least 102 ATP therapies and 34 shocks, the patient’s device functioned for approximately 8 years prior to generator replacement, demonstrating the durability of modern ICD systems and the cumulative impact of recurrent therapies on battery longevity. Recurrent ICD shocks have been associated with adverse cardiac outcomes, including increased rates of heart failure hospitalization and mortality.12 Therefore, patients experiencing recurrent inappropriate ICD shocks warrant prompt evaluation and aggressive intervention to mitigate further harm. This case highlights how a high ICD therapy burden can create downstream management challenges, often requiring subsequent providers to address the consequences of earlier device selection and programming decisions.
It is important to note that our team’s interaction with the patient was limited. Although attempts were made to follow the patient remotely, remote monitoring was never fully activated, and regular in-person follow-up did not occur despite repeated outreach efforts. Several shock-reduction strategies—including optimization of discriminator settings, extension of detection intervals, elimination of intermediate VT zones, intensification of rate-control therapies, addition of antiarrhythmic medications, or consideration of an atrioventricular junction ablation—may have reduced inappropriate therapies. However, persistent nonadherence with medications and follow-up precluded implementation of these interventions. While such strategies are effective in appropriately selected patients, their success remains contingent on sustained patient engagement.
Summary
This case highlights the substantial impact of alcohol abuse on arrhythmia burden and ICD therapy delivery. Recurrent ICD shocks alone may be insufficient to promote sustained behavioral change in patients with alcohol use disorder. Effective cardiac management requires not only optimized device programming and remote monitoring, but also coordinated behavioral health support and close longitudinal follow-up to reduce recurrent arrhythmias and inappropriate ICD therapies.
Disclosures: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest, and have no disclosures to report.
References
- Piano MR. Alcohol’s effects on the cardiovascular system. Alcohol Res. 2017;38(2):219-241. doi:10.35946/arcr.v38.2.06
- Ettinger PO, Wu CF, De La Cruz C, et al. Arrhythmias and the “holiday heart”: alcohol-associated cardiac rhythm disorders. Am Heart J. 1978;95(5):555-662. doi:10.1016/0002-8703(78)90296-x
- Voskoboinik A, Prabhu S, Ling LH, Kalman JM, Kistler PM. Alcohol and atrial fibrillation: a sobering review. J Am Coll Cardiol. 2016;68(23):2567-2576. doi:10.1016/j.jacc.2016.08.074
- Krishnamoorthy S, Lip GY, Lane DA. Alcohol and illicit drug use as precipitants of atrial fibrillation in young adults: a case series and literature review. Am J Med. 2009;122(9):851-856.e3. doi:10.1016/j.amjmed.2009.02.012
- George A, Figueredo VM. Alcohol and arrhythmias: a comprehensive review. J Cardiovasc Med (Hagerstown). 2010;11(4):221-228. doi:10.2459/JCM.0b013e328334b42d
- Voskoboinik A, Kalman JM, De Silva A. Alcohol abstinence in drinkers with atrial fibrillation. N Engl J Med. 2020;382(1):20-28. doi:10.1056/NEJMoa1817591
- Ferrick AM, Raj SR, Deneke T, et al. 2023 HRS/EHRA/APHRS/LAHRS Expert Consensus Statement on practical management of the remote device clinic. Heart Rhythm. 2023;20(9):e92-e144. doi:10.1016/j.hrthm.2023.03.1525
- Slotwiner DJ, Varma N, Akar JG, et al. HRS Expert Consensus Statement on remote interrogation and monitoring for cardiovascular implantable electronic devices. Heart Rhythm. 2015;12(7):e69-e100. doi:10.1016/j.hrthm.2015.05.008
- Gupta K, Kaminska M, Gupta S, et al. The psychological impact of implantable cardioverter defibrillators: a narrative review. Am J Cardiol. 2025 Jul 12:255:82-88. doi:10.1016/j.amjcard.2025.07.007
- Thompson LL, Claus ED, Mikulich-Gilbertson SK, et al. Negative reinforcement learning is affected in substance dependence. Drug Alcohol Depend. 2012;123(1-3):84-90. doi:10.1016/j.drugalcdep.2011.10.017
- Russ KC, Mower M, Veltri EP. Life-threatening ventricular tachyarrhythmias associated with holiday heart syndrome: treatment with the automatic implantable cardioverter defibrillator. J Electrophysiol. 1989;3(4):309-312. doi:10.1111/j.1540-8167.1989.tb01567.x
- MacIntyre CJ, Sapp JL, Abdelwahab A, et al. The effect of shock burden on heart failure and mortality. CJC Open. 2019;1(4):161-167. doi:10.1016/j.cjco.2019.04.003

