

Laser-Facilitated Lysis of Occluded Synthetic Femoropopliteal Bypass Grafts
Abstract
Background. Synthetic polytetrafluoroethylene Infra-inguinal grafts as described in the surgical literature have a 5-year patency of 40% to 50%.1 Most of the patients that receive these grafts present with acute or threatened limb ischemia. Thrombotic occlusion of synthetic femoropopliteal bypass grafts is the most common cause of graft failure. Laser thrombolysis is initiated by a light pulse delivered through the fluid catheter. The temperature of the thrombus increases as it absorbs the light, reaching levels sufficient for vaporization. These vapor bubbles collapse and disrupt the thrombus. Excimer lasers have been shown to vaporize plaque, lyse thrombus, and produce a vapor bubble at the catheter tip. Method. An excimer laser was utilized with direct lytic infusion through the laser catheter to treat patients with occluded synthetic graft occlusions from 1 day old to greater than 3 months old in an attempt to remove thrombus and treat the anastamotic lesions. Conclusion. Laser-mediated thrombolysis resulted in successful resolution of the clot burden in the synthetic femoro-popliteal bypass grafts. Prolonged hospital admission and bleeding complications were less common in this group compared to the traditional catheter-directed thrombolytics group. Large-scale studies are warranted to evaluate the safety, efficacy, and long-term patency rates with this procedure.
VASCULAR DISEASE MANAGEMENT 2013:10(3):E63-E66
Key words: graft intervention, angioplasty, adjunctive pharmacology, femoropopliteal artery
______________________________________________
 Synthetic polytetrafluoroethylene infra-inguinal grafts as described in the surgical literature have a 5-year patency of 40% to 50%.1 Most of the patients that receive these grafts present with acute or threatened limb ischemia. Thrombotic occlusion of synthetic femoropopliteal bypass grafts is the most common cause of graft failure. This most commonly occurs secondary to decreased flow caused by proximal or distal anastomotic stenosis as the synthetic graft is relatively inert. Intra-arterial thrombolytic therapy has been a well described entity since Dotter reported a series of patients with local intra-arterial administration of thrombolytic therapy.2 Thrombolytic therapy is controversial in these situations mostly due to paucity of data and poorly established studies.
Synthetic polytetrafluoroethylene infra-inguinal grafts as described in the surgical literature have a 5-year patency of 40% to 50%.1 Most of the patients that receive these grafts present with acute or threatened limb ischemia. Thrombotic occlusion of synthetic femoropopliteal bypass grafts is the most common cause of graft failure. This most commonly occurs secondary to decreased flow caused by proximal or distal anastomotic stenosis as the synthetic graft is relatively inert. Intra-arterial thrombolytic therapy has been a well described entity since Dotter reported a series of patients with local intra-arterial administration of thrombolytic therapy.2 Thrombolytic therapy is controversial in these situations mostly due to paucity of data and poorly established studies.
 Salvage of these occluded grafts has been well established. Surgical balloon embolectomy has been utilized for decades and is quite effective, particularly in relatively fresh thrombus.3 It requires a surgical procedure and may be complicated by embolization or difficulty crossing anastomotic strictures with the balloon. Prolonged lytic infusions have been effective in graft salvage even with fairly chronic occlusions. Lytic infusion typically requires at least overnight admission to an ICU and there is risk of minor and major bleeding complications as well as embolic complications.4 More recently mechanical thrombectomy devices have been utilized alone or in combination with lytics to achieve more rapid lysis and mitigate bleeding risks.5 Mechanical thrombectomy has been highly effective in fresh thrombus but much less effective in older, more organized thrombus.6 Hemolysis, residual thrombus, and distal embolization are recognized complications of isolated mechanical lysis. When coupled with acute arterial lytics, rapid clot removal can often be achieved but this is associated with more bleeding complications. Laser thrombolysis is initiated by a light pulse delivered through the fluid catheter. The temperature of the thrombus increases as it absorbs the light, reaching levels sufficient for vaporization. These vapor bubbles collapse and disrupt the thrombus. Excimer lasers have been shown to vaporize plaque, lyse thrombus, and produce a vapor bubble at the catheter tip. An excimer laser was used with direct lytic infusion through the laser catheter to treat patients with occluded synthetic graft occlusions from 1 day old to greater than 3 months old in an attempt to remove thrombus and treat the anastomotic lesions.
Salvage of these occluded grafts has been well established. Surgical balloon embolectomy has been utilized for decades and is quite effective, particularly in relatively fresh thrombus.3 It requires a surgical procedure and may be complicated by embolization or difficulty crossing anastomotic strictures with the balloon. Prolonged lytic infusions have been effective in graft salvage even with fairly chronic occlusions. Lytic infusion typically requires at least overnight admission to an ICU and there is risk of minor and major bleeding complications as well as embolic complications.4 More recently mechanical thrombectomy devices have been utilized alone or in combination with lytics to achieve more rapid lysis and mitigate bleeding risks.5 Mechanical thrombectomy has been highly effective in fresh thrombus but much less effective in older, more organized thrombus.6 Hemolysis, residual thrombus, and distal embolization are recognized complications of isolated mechanical lysis. When coupled with acute arterial lytics, rapid clot removal can often be achieved but this is associated with more bleeding complications. Laser thrombolysis is initiated by a light pulse delivered through the fluid catheter. The temperature of the thrombus increases as it absorbs the light, reaching levels sufficient for vaporization. These vapor bubbles collapse and disrupt the thrombus. Excimer lasers have been shown to vaporize plaque, lyse thrombus, and produce a vapor bubble at the catheter tip. An excimer laser was used with direct lytic infusion through the laser catheter to treat patients with occluded synthetic graft occlusions from 1 day old to greater than 3 months old in an attempt to remove thrombus and treat the anastomotic lesions.
 Method
Method
78 consecutive patients with thrombotic occlusion of synthetic femoropopliteal synthetic bypass grafts deemed suitable for lytic therapy were treated between 2001 and 2011. Graft occlusions were less than 2 weeks old in 41 patients and greater than 2 weeks old in 37 patients. Four occlusions were at least 3 months old. Patients were treated with an excimer laser coupled with 10 mg of tenecteplase (TNK) directly infused through the laser catheter during the process of photoablation followed by a dwell time of 20 minutes then repeat photoablation. This was performed in an effort to achieve more rapid dissolution of thrombus obviating the need for overnight admission and prolonged lytic infusion with its inherent bleeding risks and cost. The goal was to attempt complete revascularization during the index interventional procedure.
Procedural Technique
The procedure was performed using the following steps:
- Contralateral access with a 7F crossover sheath
- Administration of intravenous heparin to achieve activated clotting time of 250 to 350
- Administration of 200 µg of nitroglycerin
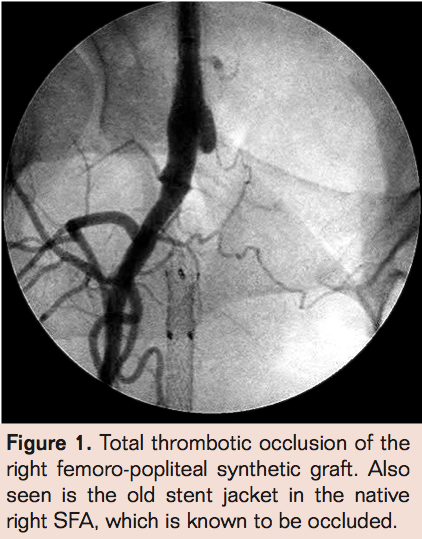
- Angiography utilizing ipsilateral obique projection to visualize graft origin if possible (may not visualize). Evaluate outflow as well (Figure 1).
- Cross occlusion with guidewire of choice (must exchange for .014 guidewire if larger wires used to cross) (Figure 2)
- Laser thrombectomy with a 0.9 mm probe advanced 1 mm/sec with saline flush via the sheath (Figure 3)
- Laser atherectomy utilizing a 2.3 mm probe while administering 10 mg of TNK (mixed with 50 cc of saline) through the lumen of the laser catheter by connecting a Touhy-Borst adapter to the laser catheter (the wire lumen is .024). Laser catheter advanced no more than 1 mm/sec.
- Dwell time of at least 20 minutes
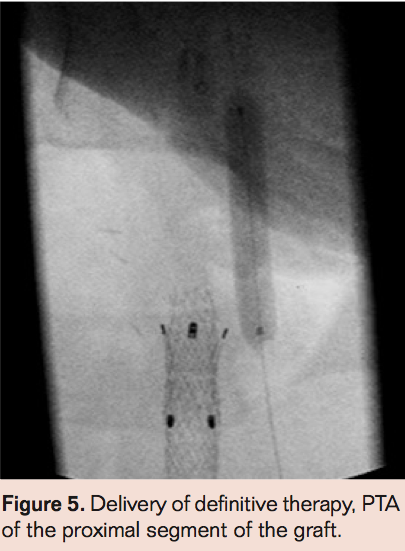
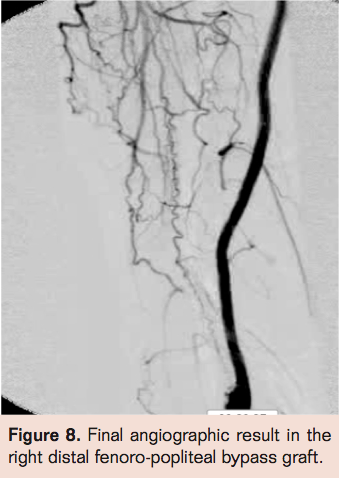
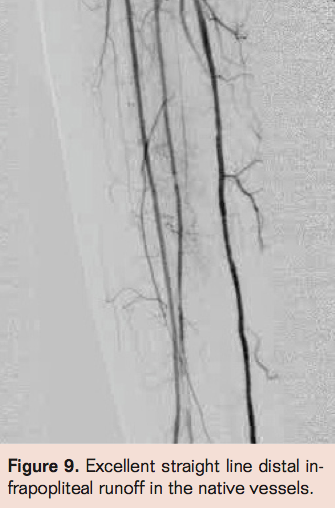
- Laser thrombectomy at 1 mm/sec. with the 2.3 mm probe (Figures 4-9)
- Repeat angiography, and if there is no obvious thrombus proceed to definitive therapy. If there is no flow, then perform angiography via side hole perfusion catheter placed across the occlusion to determine residual thrombus. Patients with residual thrombus are treated with TNK infusion via infusion catheter at 0.5 mg/hr. Repeat angiography at 3 hours to assess patency. If necessary, perform prolonged lytic infusion followed by definitive therapy.
 Findings
Findings
Complete angiographic resolution of thrombus and definitive therapy was achieved in 51 of 78 patients (65.3%) during the index angiographic procedure in the angiographic suite. In 12 of 78 patients (15.3%) flow was established in the index procedure but there was residual thrombus necessitating continued lytic infusion. Of those 12 who had residual thrombus, 11 had complete resolution of thrombus following 3 hours of lytic therapy allowing definitive therapy in the same day. No flow was established during the index procedure for 15 of 78 patients (19.2%). Of these patients angiography via the side hole perfusion catheter showed substantial resolution of thrombus but enough residual thrombus to obstruct antegrade flow in 14 of 15. There was no evidence of thrombus resolution in 1 of 15 patients for whom no flow was established in the index procedure. Of those 15 patients,3 (20%) had complete resolution of thrombus at 3 hours post angiography while 12 of 15 patients (80%) required prolonged lytic infusion. Graft patency was established in 78 of 78 patients but bleeding complications were much less common in the group with successful index procedure than those requiring overnight infusion (2% vs 47% with major bleeding necessitating transfusion of 2 units of PRBC’s in 2 patients who had overnight lytics).
 Conclusion
Conclusion
Laser-mediated thrombolysis is a major modification of the traditional doctrine. In this study, laser-facilitated lysis allowed definitive therapy of occluded synthetic femoropopliteal grafts during the index procedure with no need for critical care admission during the index procedure in 65.4% of patients; 15.4% of patients had definitive therapy at the second angiogram performed 3 hours following initiation of lytic infusion following the index procedure; and 19.2% of patients required prolonged lytic infusion before definitive therapy. Bleeding complications were less common in those patients with successful index procedure than those requiring prolonged infusion. Successful revascularization was achieved in all of these patients. More studies are warranted to evaluate the safety and efficacy of this technique. Future studies should evaluate different doses of lytic agents, more prolonged dwell times, use of distal protection devices, and varying techniques.

References
- Michaels JA. Choice of material for above-knee femoropopliteal bypass graft. Br J Surg. 1989;76(1):7-14.
- Dotter CT, Rosch J, Seaman AJ, Dennis D, Massey WH. Streptokinase treatment of thromboembolic disease. Radiology. 1972;102(2):283-290.
- Aburahma AF, HopkinsES, Wulu JT Jr, Cook CC. Lysis/balloon angioplasty versus thrombectomy/open patch angioplasty of failed femoropopliteal polytetrafluoroethylene bypass grafts. J Vasc Surg. 2002;35(2):307-315.
- Swischuk JL, Fox PF, Young K, et al. Transcatheter intraarterial infusion of rt-PA for acute lower limb ischemia: results and complications. J Vasc Interv Radiol. 2001;12(4):423-430.
- Shammas NW, Dippel EJ, Shammas G, Gayton L, Coiner D, Jerin M. Dethrombosis of lower extremity arteries using the power-pulse spray technique in patients with recent onset thrombotic occlusions: results of the DETHROMBOSIS registry. J Endovasc Ther. 2008;15(5):570-579.
- Kalinowski M, Waqner HJ. Adjunctive techniques in percutaneous mechanical thrombectomy. Tech Vasc Interv Radiol. 2003;6(1):6-13.
__________________________________

 Editor’s Note: Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr.Walker reports stock ownership, speaker honoraria, board membership, and teaching courses for Spectranetics. Dr. Patlola reports that he is a consultant to Spectranetics. No other disclosures were reported in relation to this manuscript.
Editor’s Note: Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr.Walker reports stock ownership, speaker honoraria, board membership, and teaching courses for Spectranetics. Dr. Patlola reports that he is a consultant to Spectranetics. No other disclosures were reported in relation to this manuscript.
Manuscript received May 3, 2012, final version accepted June 5, 2012.
Address for correspondence: Raghotham R. Patlola, MD, FACC, Division of Cardiology, Cardiovascular Institute of the South, 2730 Ambassador Caffery Parkway, Lafayette, LA, 70506, USA. Email address: rpatlola@aol.com
