Managing Complex Ischial Pressure Injury in a Patient with Congenital Amelia: A Multistage Freestyle Flap Reconstructive Strategy
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Management of complex stage 4 ischial pressure injuries (PIs) is challenging, particularly in patients with congenital anomalies, severe comorbidities, and limited reconstructive options. Ethical and functional considerations may further constrain surgical decision-making. Case Report. The present report discusses a paraplegic patient with congenital amelia who developed a chronic, recurrent stage 4 ischial-perineal PI complicated by osteomyelitis and prior reconstructive failure. A multidisciplinary, staged approach was used, including serial debridement, infection control, nutritional optimization, negative pressure wound therapy, and delayed freestyle flap reconstruction. Intraoperative perfusion was assessed via intraoperative laser angiography using indocyanine green. Definitive reconstruction was achieved using a pelvic torso V-Y advancement flap with adjunctive groin advancement scrotoplasty to address testicular exposure. Ethical considerations, including preservation of the patient’s only viable site for noninvasive blood pressure monitoring, directly influenced reconstructive planning. Durable wound closure was achieved without major complications, and satisfactory healing was noted at 3-month follow-up. Conclusion. This case highlights the importance of individualized, patient-centered, and ethically informed decision-making in the management of complex PIs. Multidisciplinary collaboration and tailored reconstructive strategies can achieve successful outcomes in patients with rare congenital conditions and limited surgical options.
Pressure injuries (PIs) are a common debilitating problem and continue to impose a substantial financial and health care burden.1 PIs are skin and soft tissues injuries that arise because of localized damage from continuous tissue compression.1 Specifically, the combination of shear and friction forces exerted by sustained external pressure affects underlying capillary beds, causing tissue ischemia with subsequent necrosis of skin and underlying subcutaneous tissues.2 PIs frequently occur over bony prominences, most commonly over the ischial and sacral regions.2 Stage 4 PIs are full-thickness skin defects to underlying fascia with extensive tissue loss that may involve muscle, bone, tendon, and/or joints.3
Treatment of PIs varies depending on the presence of concomitant infections, the extent of tissue injury, injury depth, and associated complications. Surgical intervention for stage 4 PIs includes serial debridement of infected devitalized or necrotic tissues to improve the healing potential of the remaining healthy tissue.
Reconstructive options may be considered to cover the defect and obliterate dead space after debridement. Different options for staged versus immediate reconstruction have been described to restore damaged tissue, including primary wound closure, skin grafting, skin or muscle flaps or musculocutaneous flaps, pedicled flaps, and, rarely, microvascular free flaps.3 Complex stage 4 sacral and ischial injuries in patients with paraplegia pose a significant challenge due to high complication and recurrence rates after reconstruction.4
The case reported herein involved multistage reconstruction of a chronic complex stage 4 ischial-perineal injury in a patient with paraplegia. This case was particularly challenging and required significant ethical consideration and discussions because of the patient’s congenital amelia.
Congenital amelia is an extremely rare birth defect characterized by the complete absence of 1 or more extremities resulting from disruption of limb bud development during embryogenesis.5 The estimated incidence is approximately 1.4 per 100,000 births.5 Patients with congenital amelia often experience profound functional limitations, altered biomechanics, and unique challenges related to positioning, mobility, and pressure distribution, which predisposes them to pressure-related injuries.
The present case illustrates the complexity of managing chronic PIs with superimposed osteomyelitis in patients with congenital and neurologic impairments. A multidisciplinary approach including staged debridement, infection control, nutritional optimization, and delayed flap reconstruction allowed for successful wound closure and functional recovery.
Case Report
A 36-year-old male with a complex medical and surgical history presented to Banner University Medical Center-Phoenix with concerns about a worsening right ischial wound with purulent drainage and associated fevers, chills, and malaise. His medical history is significant for congenital amelia, scoliosis status post spinal fusion complicated by paraplegia, neurogenic bladder requiring a chronic suprapubic catheter complicated by recurrent urinary tract infections, and chronic stage 4 ischial-perineal PIs. The patient also reported an extensive surgical history to address previous PIs, including previous biologic grafts, local soft tissue advancement, and rotational flap reconstructions, all of which had failed or had resulted in short-term recurrence.
Two months prior to his presentation, the patient was diagnosed with methicillin-sensitive Staphylococcus aureus (MSSA) bacteremia. At that time, repeat cultures of blood from his known port-a-cath were negative. Additionally, transthoracic echocardiography was negative for vegetations or other sources of MSSA bacteremia. The patient was advised to undergo removal of the port-a-cath and prolonged intravenous (IV) antibiotic therapy. However, he refused this and was subsequently discharged on oral cefalexin. He was lost to follow-up until his home health wound care team urged him to seek further evaluation given his worsening clinical status, at which point he presented to the facility of the authors of the present report. When discussing precautions to prevent development of PIs, the patient reported use of a custom motorized wheelchair at baseline; however, he was not compliant with routine seat pressure mapping evaluations. Additionally, he admitted to only mild to moderate adherence to off-loading recommendations, turning every 3 hours to 4 hours while in bed instead of the recommended 2 hours. He also denied use of a low air loss mattress at home.
On initial presentation, the patient was afebrile and otherwise hemodynamically stable, with reports of weakness, fatigue, fevers, chills, and anorexia. Laboratory results were significant for symptomatic microcytic anemia (hemoglobin level of 6.9 g/dL) requiring transfusion of 1 unit of packed red blood cells, an elevated C-reactive protein level of 206.8 mg/L, and a low prealbumin level of 10 mg/dL. Urinalysis was significant for pyuria, leukocyte esterase level of 75 mg/dL, and bacteriuria.
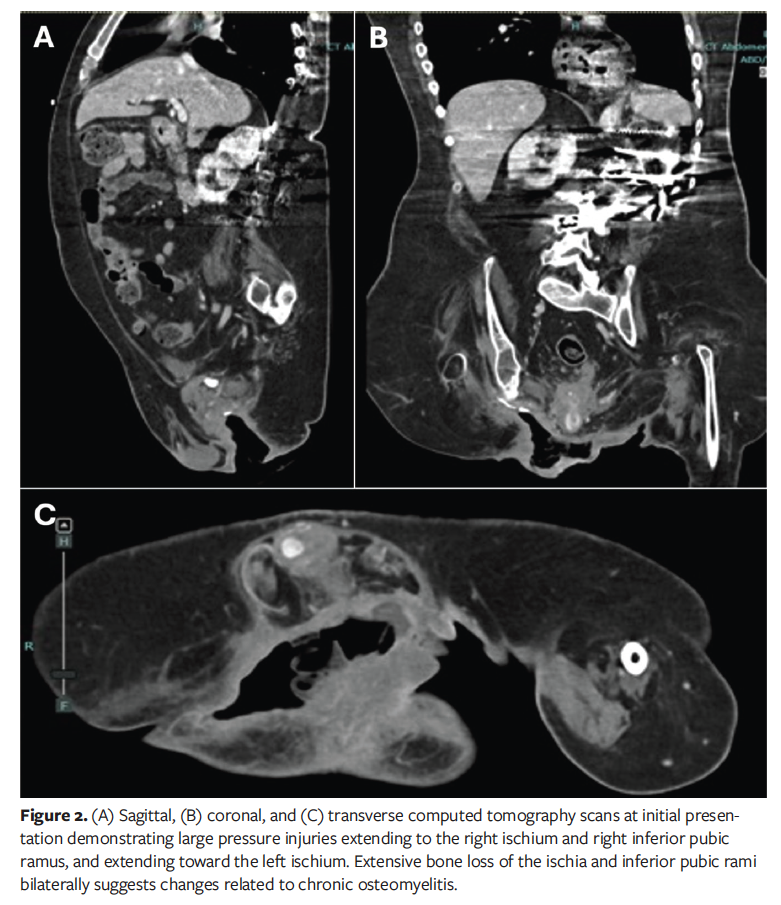
On physical examination, a large stage 4 PI was observed over the right ischium with perineal extension (Figure 1). Initial diagnostic computed tomography (CT) of the abdomen and pelvis was performed to evaluate the extent of the soft tissue defect and underlying bony destruction. This imaging demonstrated a large PI at the right ischium and inferior pubic ramus extending to the left ischium with extensive bony destruction suggestive of acute on chronic osteomyelitis (Figure 2). Subsequent pelvic magnetic resonance imaging confirmed acute on chronic osteomyelitis of the right ischium and inferior pubic ramus. The patient was started on broad-spectrum IV antibiotic therapy with vancomycin and piperacillin/tazobactam.

Given that the patient had active purulent drainage from the extensive tissue injury, systemic symptoms, and poor nutritional status, the decision was made to proceed with initial extensive excisional debridement of the perineal soft tissue, right ischial ostectomy, and negative pressure wound therapy (NPWT). Prior to initial surgical intervention, a long discussion was had with the patient regarding possible diverting colostomy and enteral feeding access to allow for adequate nutrition for healing and prevention of wound bed contamination. Although he was agreeable to surgical debridement, he was adamantly against colostomy and enteral access due to perceived social stigma and negative effect on his robust baseline sexual activity. Initially, the proposed surgical intervention was a filet of limb flap using the patient’s thigh as a donor site. After extensive ethical consideration and discussion with orthopedic surgery and the intensive care unit teams, however, this plan was abandoned because it would sacrifice the patient’s only noninvasive blood pressure monitoring location, which would significantly alter his future care.
The patient subsequently underwent extensive perineal debridement, bone biopsy, and NPWT. Intraoperative cultures were negative. The patient remained hospitalized and received NPWT for 3 weeks postoperative prior to undergoing the second stage of soft tissue perineal reconstruction. During this period, he underwent nutritional optimization under the guidance of the nutrition team. He received a regimen of oral nutritional supplements administered 3 times daily, each providing approximately 300 kcal and 20 g of protein to support caloric and protein requirements for wound healing, in conjunction with serial monitoring of clinical and laboratory nutritional parameters.
Additionally, a dedicated CT angiography (CTA) of the pelvis was performed to better delineate the patient’s vascular anatomy and assist with flap planning. This study demonstrated a maldeveloped femoral vascular system but identified adequate perforator supply to support a pelvic torso advancement flap.
Surgical technique
The patient was positioned in the left lateral decubitus position, and standard sterile preparation and time-out were performed. Repeat excisional debridement was performed, including bone biopsy, with specimens sent for histopathologic and microbiologic analysis. Hemostasis was achieved, and the wound was copiously irrigated prior to reconstruction.
Following wound assessment, soft tissue reconstruction was performed using a pelvic torso hatchet-style V-Y advancement flap. The flap was designed with a proximally based pedicle to optimize vascularity from an undeveloped femoral vascular system. The flap was elevated in the subcutaneous plane with preservation of perforators and underlying poorly developed musculature. The flap was advanced to achieve tension-free coverage of the defect, and intraoperative perfusion was confirmed using SPY Portable Handheld Imager (SPY-PHI; Stryker), hereafter referred to as intraoperative laser angiography using indocyanine green. The donor site was closed primarily.
Because of extension of the tissue injury into the scrotum with exposure of the bilateral testes, additional reconstruction was required. A rotational advancement adipocutaneous flap from the right anterior groin was used to perform a complicated scrotoplasty, providing durable coverage of the exposed testes. Flap perfusion was again confirmed with intraoperative laser angiography using indocyanine green prior to flap inset. Complete closure of the ischial and perineal wounds was achieved.
Postoperative course
Given the patient’s complex medical and social history, his postoperative course was complicated by a prolonged hospital admission. Intraoperative cultures from the second excisional debridement were significant for Candida parapsilosis, Pseudomonas aeruginosa, and Klebsiella oxytoca, requiring prolonged IV antibiotic and antifungal treatment for approximately 3 weeks. Due to the patient’s inability to maintain adequate oral intake postoperatively, he required enteral feeding access via a percutaneous endoscopic gastrostomy/percutaneous endoscopic jejunostomy (PEG/PEJ) tube to allow optimal wound healing and prevent failure of the soft tissue reconstruction. Enteral feeding resulted in restoration of the patient’s prealbumin level to 20 mg/dL at discharge.
Additionally, due to the fragility of his perineal reconstruction and history of previous graft/flap failure, the patient was restricted to strict bed rest for 5 weeks. During that time, he was only able to position himself flat or left lateral decubitus with frequent off-loading every 1 hour to 2 hours. The patient was eventually deemed medically appropriate for discharge to a long-term acute care facility with the PEG/PEJ tube and bed rest restrictions in place.
At a follow-up visit 3 months postoperatively, the patient had no additional postoperative complications and was healing well despite some minor excoriation of the perineum (Figures 3 and 4). Given his strict adherence to the previous restrictions, the patient was deemed appropriate to advance to a structured sitting protocol with a customized seat cushion. Sitting duration was progressively increased up to a maximum of 2 hours, with subsequent mandatory pressure off-loading and monitoring of the surgical site for erythema, drainage, and skin compromise.

At 5 months postoperative, the patient returned for evaluation and reported spending the majority of his time in a seated position; he also reported difficulty adhering to recommended off-loading precautions. Physical examination revealed development of a new perineal wound adjacent to the prior reconstruction site. Given the absence of flap compromise, management with aggressive local wound care was planned, including NPWT and close follow-up with the wound care clinic. The patient and his family were advised to adhere to strict off-loading precautions, and he was scheduled for close outpatient follow-up while a plan for future management was made. However, the patient was subsequently lost to follow-up.
Discussion
The current case underscores the intricate challenges associated with managing chronic PIs complicated by osteomyelitis in a patient with complex congenital and acquired comorbidities. The patient’s congenital amelia, paraplegia following surgical correction of scoliosis, and chronic urinary catheterization created a clinical context highly susceptible to pressure-related soft tissue compromise and infection. In particular, immobility, impaired sensation, and lack of adequate pressure off-loading mechanisms in the setting of recent illness, surgery, and hospitalization contributed to the development and progression of the ischial pressure injury, which ultimately extended to involve underlying osseous and perineal soft tissue structures. Additional considerations for the patient’s active sexual lifestyle also complicated matters because surgical fecal diversion and durable medical equipment was deemed unacceptable by the patient.
The pathophysiology of pressure-induced tissue injury in patients with neurologic impairment is well described in the literature.6 The ischial region is especially vulnerable due to its prominence and the sustained pressure exerted during seated positioning. In the current report, the absence of a pressure-relieving mattress and lack of updated postoperative pressure mapping likely accelerated tissue breakdown. Lack of bilateral lower extremities also greatly limited the patient’s balance and options for pressure off-loading while in the seated position. Once the subcutaneous and deep perineal and ischial tissue was compromised, a chronic wound environment ensued, allowing for bacterial colonization and subsequent osteomyelitis in the face of repeated contamination from feces. Initial diagnostic CT of the abdomen and pelvis played a pivotal role in guiding preoperative planning by identifying soft tissue tracts and osseous involvement. Additionally, preoperative CTA showed the patient’s unique vascular anatomy, which allowed for creation of a freestyle flap based on the maldeveloped femoral vessels.
Malnutrition represented a significant barrier to wound healing and surgical reconstruction in the current case. The patient demonstrated significant malnutrition on presentation, evidenced by a prealbumin level of 10 mg/dL, severe anemia requiring transfusion, and clinical signs of cachexia. Although prealbumin level has historically been used as a nutritional marker, it is an acute phase reactant and may be influenced by systemic inflammation. Thus, nutritional status was assessed in conjunction with clinical parameters, inflammatory markers, and multidisciplinary dietitian-led evaluation. Nutritional optimization is essential in patients undergoing complex reconstruction, because poor nutritional status is strongly associated with increased postoperative complications and impaired flap survival.6 In the current case, early intervention and optimization by the nutrition team allowed for stabilization and improved candidacy for definitive surgical repair. However, it should be noted that preoperative high protein enteral nutrition and supplementation were advised but ultimately not pursued due to patient preference. The early initiation of enteral feeding postoperative likely played a significant role in the patient’s recovery due to its association with improved wound healing, reduced infection rates, shorter hospital stays, and modulation of the immune response.7 In the current case, optimization with enteral nutrition was essential to ensure adequate perfusion and viability of the reconstructive flaps.
The patient’s history of congenital amelia posed a unique challenge to surgical reconstruction, primarily due to the limited availability of donor sites for flap harvest. In the setting of an extensive tissue defect and prior failed reconstruction, options for flap-based coverage were markedly constrained. A V-Y advancement flap from the pelvic torso was used to achieve durable coverage of the ischial and perineal defects. Intraoperative laser angiography using indocyanine green played a critical role in evaluating flap perfusion and confirming adequate vascularity. The magnitude of tissue loss also required adjunctive procedures, including scrotoplasty with a groin advancement flap, to address testicular exposure and restore both anatomic form and functional integrity.
Beyond the technical complexity of reconstruction, this case highlights the ethical and multidisciplinary considerations inherent in caring for patients with rare congenital anomalies and severe functional limitations. The patient’s congenital amelia resulting in a solitary rudimentary lower extremity imposed unique perioperative constraints, including preservation of that limb for essential physiologic monitoring and positioning in the critical care setting. These considerations directly influenced reconstructive decision-making, necessitating sacrifice of a potential filet of leg flap in favor of alternative coverage strategies that prioritized overall patient safety. Additionally, the patient’s baseline robust sexual activity and expressed desire to preserve sexual function underscored the importance of avoiding a diverting ostomy and restoring durable scrotal coverage, not only as an anatomic goal but as a determinant of quality of life. Thus, successful reconstruction required careful balance between wound eradication, functional preservation, and respect for patient autonomy.
This case emphasizes that optimal management of complex PIs extends beyond defect closure alone and requires thoughtful ethical deliberation, shared decision-making with the patient, and close coordination among the multidisciplinary team to align surgical goals with the patient’s physiologic needs and personal values. Furthermore, long-term success in pressure injury reconstruction requires continued adherence to pressure off-loading strategies, routine seat pressure mapping, and use of specialized support surfaces.
Consistent with the well-documented recurrence rates of PIs in patients with neurologic impairment,6 the patient in the current report later developed a new perineal wound several months after reconstruction in the setting of prolonged seated positioning and difficulty adhering to off-loading recommendations. This highlights the critical role of long-term pressure management and patient adherence in maintaining reconstructive success.
Limitations
This report describes a single patient experience and thus, lacks generalizability. The reconstructive strategy described was highly individualized and influenced by unique anatomic, functional, and ethical considerations related to congenital amelia, which may not be directly applicable to other patients with PIs. Additionally, long-term outcomes beyond the short-term follow-up period are not yet available, and recurrence remains a known risk in patients with chronic PIs. Despite these limitations, this case provides valuable insight into multidisciplinary decision-making and reconstructive planning for complex wounds in patients with rare congenital conditions and severely limited reconstructive options.
Conclusion
This case exemplifies the complexity of reconstructive options and management in a patient with congenital limb anomalies and paraplegia complicated by chronic PIs and osteomyelitis. Successful treatment required a comprehensive, multidisciplinary approach that integrated surgical debridement, prolonged broad-spectrum IV antibiotic and antifungal coverage, nutritional optimization, and the use of vascularized soft tissue flap reconstruction for durable wound coverage. The combination of these strategies led to an effective surgical outcome and meaningful improvement in the patient’s quality of life. However, continued vigilance in postoperative care and long-term off-loading strategies are essential to prevent recurrence and preserve the integrity of reconstruction.
Author and Public Information
Authors: Jacob C. Koster, ScB1; Taylor Kreul, BS1; David Rincon, BS1; Agustin Herber, DO1,2; and Jimmy Chim, MD1,3
Affiliations: 1The University of Arizona College of Medicine-Phoenix, Phoenix, AZ, USA; 2Department of Surgery, Banner–University Medical Center Phoenix, Phoenix, AZ, USA; 3Division of Plastic and Reconstructive Surgery, Banner–University Medical Center Phoenix, Phoenix, AZ, USA
Disclaimer: The views expressed in this article are those of the authors and do not necessarily represent the official views or policies of their affiliated institutions.
Ethics Statement: Informed patient consent was obtained prior to the writing and submission of this manuscript and is on file at the University of Arizona College of Medicine-Phoenix.
Disclosure: J.C. is a consultant to MTF Biologics. No financial support, equipment, drugs, or other proprietary materials from MTF Biologics or any other commercial entity were provided for this work. The other authors disclose no financial or other conflicts of interest.
Corresponding Author: Jimmy Chim, MD; Banner–University Medical Center Phoenix, 1111 East McDowell Rd, Phoenix, AZ 85006; jimmy.chim@bannerhealth.com
Manuscript Accepted: April 21, 2026
References
1. Mervis JS, Phillips TJ. Pressure ulcers: pathophysiology, epidemiology, risk factors, and presentation. J Am Acad Dermatol. 2019;81(4):881-890. doi:10.1016/j.jaad.2018.12.069
2. Mervis JS, Phillips TJ. Pressure ulcers: prevention and management. J Am Acad Dermatol. 2019;81(4):893-902. doi:10.1016/j.jaad.2018.12.068
3. Fähndrich C, Gemperli A, Baumberger M, et al. Treatment approaches of stage III and IV pressure injury in people with spinal cord injury: a scoping review. J Spinal Cord Med. 2023;46(5):705-715. doi:10.1080/10790268.2022.2108645
4. Krakowczyk D, Opyrchał J, Koszutski T, Dowgierd K, Krakowczyk Ł. Reconstructive options for pressure ulcers in pediatric patients. Children (Basel). 2024;11(6):691. doi:10.3390/children11060691
5. Bermejo-Sánchez E, Cuevas L, Amar E, et al. Amelia: a multi-center descriptive epidemiologic study in a large dataset from the International Clearinghouse for Birth Defects Surveillance and Research, and overview of the literature. Am J Med Genet C Semin Med Genet. 2011;157(4):288-304. doi:10.1002/ajmg.c.30319
6. Alito A, Portaro S, Leonardi G, et al. Pressure ulcers—a longstanding problem: a 7-year neurorehabilitation unit experience of management, care, and clinical outcomes. Diagnostics (Basel). 2023;13(20):3213. doi:10.3390/diagnostics13203213
7. Gramlich L, Guenter P. Enteral nutrition in hospitalized adults. N Engl J Med. 2025;392(15):1518-1530. doi:10.1056/NEJMra2406954