



Comparison of Clinical Characteristics According to Etiological Classification of Pressure Injuries in Pediatric Patients: A Retrospective Cohort Study
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Pressure injuries remain a significant problem in health care, and more studies are needed on their recognition, prevention, and treatment in the pediatric population. Objective. To evaluate pressure injuries in hospitalized pediatric patients according to etiology (medical device–related pressure injury [MDRPI] vs immobility-related pressure injury [IRPI]) and compare demographic, clinical, and treatment characteristics, in order to inform etiology-specific prevention and management strategies. Materials and Methods. This single-center retrospective cohort study included pediatric patients (age at pressure injury identification, 0–211 months) hospitalized between August 2020 and December 2024. Wounds were classified as MDRPI or IRPI. Healing response was categorized as either medical (dressing and local care) or surgical treatment. Results. Of 283 pressure injuries in 149 patients, 225 (128 patients) were IRPI and 58 (37 patients) MDRPI; 16 patients had both. Localization differed significantly (P < .001): IRPIs predominated in occipital and sacral regions, MDRPIs in the ear and neck. IRPIs were larger at baseline (median, 3.0 vs 1.0 cm²; P < .001) and more often unstageable (20.8%) or deep tissue (3.6%) injuries, neither observed in MDRPIs (P = .001). Surgical intervention was required for 35.0% of IRPIs vs. 7.4% of MDRPIs (P < .001); median treatment duration was longer in IRPIs (29 vs 18 days; P = .002). Conclusions. This study shows significant differences between IRPIs and MDRPIs in terms of localization, initial wound size, wound stage, healing response, and treatment duration. The findings suggest a need for etiology-specific treatment strategies for pediatric pressure injuries, as well as the importance of developing risk management protocols specific to each wound type.
Pressure injuries (PIs) are defined as tissue damage in the skin and subcutaneous tissues caused by prolonged pressure, sometimes with the contribution of friction.1 These wounds remain a significant problem in health care delivery, and it is important to recognize them in the pediatric population.2 The reported prevalence of pressure injuries in childhood varies between 1.4% and 8.2%, with a rate of up to 43.1% in critical care areas.3-6 In pediatric patients, physiological differences as well as the limitation of treatment options make the healing process difficult.7,8 Immature skin structure, weak dermoepidermal connections, and increased transepidermal water loss lead to rapid progression of PIs and increased risk of infection.9,10 Therefore, critically ill children are at high risk of developing PIs in the hospital.4-6,11-13 Published data on pediatric PIs are scarce; most existing evidence is derived from adult studies.1,4,11,12,14
PIs may differ according to their etiology. Medical device-related pressure injuries (MDRPIs) are defined as tissue damage caused by direct contact of medical devices with the skin. In contrast, immobility-related pressure injuries (IRPIs) usually occur on bony prominences or in tissue areas in contact with the support surface.15,16
Prevention of MDRPIs may be more complex compared with conventional PIs because the device itself may be an integral part of diagnosis or treatment.17,18 Few studies have examined the treatment and healing process of MDRPIs, even in the adult literature.19,20 Studies on PIs have primarily focused on incidence and prevalence, as well as the determination of preventable risk factors.20-22 However, despite all preventive measures, the incidence of PIs has not decreased for decades.23,24 Thus, a detailed examination of the clinical and treatment process-specific differences between MDRPI and IRPI in pediatric patients is needed.
This study aimed to evaluate PIs in hospitalized pediatric patients according to etiology (MDRPI vs IRPI) and to compare the demographic, clinical, and treatment characteristics of these 2 groups in an effort to contribute to the development of etiology-specific pediatric PI prevention and management strategies.
Materials and Methods
Study design and setting
This retrospective cohort study was conducted at Dr Behçet Uz Pediatric Diseases and Surgery Training and Research Hospital (Izmir, Turkey)and included data on pediatric patients treated between August 2020 and December 2024. The study included pediatric patients hospitalized in various wards, including the neonatal intensive care unit (NICU), pediatric intensive care unit (PICU), surgical intensive care unit, and cardiovascular surgical intensive care unit. The pressure injuries in patients who were diagnosed with pressure injuries and who started treatment in these wards were divided into 2 groups: MDRPI and IRPI.
Electronic medical records, wound photographs, and the pressure injury staging form completed daily by specialist wound care nurses (hospital wound care team) were retrospectively reviewed. In the study institution, specialist wound care nurses are registered nurses assigned to the hospital wound care team. These nurses have dedicated training and routine clinical responsibility for pressure injury assessment, staging according to the European Pressure Ulcer Advisory Panel (EPUAP)/National Pressure Ulcer Advisory Panel (now National Pressure Injury Advisory Panel [NPIAP])/Pan Pacific Pressure Injury Alliance (PPPIA) 2019 guidelines, and documentation. The 6-step staging system updated in the aforementioned guidelines was used to stage pressure injuries as stage 1, stage 2, stage 3, stage 4, unstageable pressure injury (UPI), or deep tissue pressure injury (DTPI).25 As recommended by NPIAP, the term "pressure injuries" is used throughout this article, though cited research might rely on the outdated term "pressure ulcers."
Study population
All pediatric patients who developed pressure injuries within the specified period were included in the study. The pediatric cohort encompassed the full inpatient age spectrum, including neonates. Eligible patients ranged from 0 to 211 months of age at the time of pressure injury identification. Both IRPIs and MDRPIs were included. For MDRPIs, only skin injuries were included; mucosal MDRPIs were excluded because they could not be evaluated using the EPUAP/NPIAP/PPPIA classification.25 Patients who were followed as outpatients or treated at home, and patients who were interned to participating wards for less than 24 hours were not included in the study. Because adequate oxygenation and perfusion of the tissue is necessary for wound healing26 and because no treatment can provide healing of the existing wound in patients whose general condition gradually deteriorates and who die due to progression of the primary disease,26-29 such patients were not included in statistical studies analyzing wound stage, response to treatment, and wound healing time. Similarly, patients whose medical or surgical treatment was ongoing during the specified date range were not included in the statistical studies analyzing wound stage, response to treatment, and wound healing time. Informed consent was obtained from the parents of each patient, and the study was reviewed and approved by the ethics committee of the study hospital.
Data collection
Data on patients’ medical records, pressure injuries, and medical treatment were obtained from the hospital information management system (Probel Software; Probel Software Company) and from the pressure injury staging form. Each patient hospitalized in the study hospital’s intensive care units is followed up with the Braden Q scale by the nurses on duty, and at-risk patients are reported to specialist wound care nurses.
In the current study, the term specialist wound care nurses refers to the designated hospital wound care team, not unit-based nursing champions. Bedside or unit nurses perform routine risk screening (eg, Braden Q scale). However, formal pressure injury staging and the daily staging documentation used for study analyses are performed by the specialist wound care nurses, who record patients’ demographic and clinical data and plan treatment with the pediatric surgeon.
Treatment decisions (conservative vs surgical/procedure-based treatment) were made by the institutional multidisciplinary wound care team, led by specialist wound care nurses in collaboration with a pediatric surgeon, and aligned with the primary intensive care unit or ward team. Escalation to surgical/procedure-based treatment was considered when wound progression, necrotic tissue burden, or lack of improvement despite conservative care was documented on serial wound assessments. Treatment was applied at the determined frequency, and changes in the wound were noted. In the case of signs of infection, a swab was collected and cultures performed. For this study, wound infection status was determined from the electronic medical record based on documented clinical signs of infection and, when performed, wound swab culture results. Wounds without such documentation were categorized as having no documented infection. At the study instutition, the treatment plan is changed in patients who do not improve despite regular treatment or whose wounds worsen. In each patient whose treatment plan is changed, the wound dimensions and stage are recorded on the daily wound assessment form. In patients for whom treatment is progressing favorably, the treatment plan is altered if deemed necessary according to the current stage of the wound.
Demographic data collected in the present study included age and sex. In addition, clinical data such as the ward in which each patient was hospitalized, primary disease, time to wound formation, wound localization, wound dimensions before and after treatment, and presence and stage of infection were obtained by examining the records.
Reducing pressure on the wound and the resulting ischemia by changing the position of the patient or medical equipment every 2 hours to 4 hours during the wound treatment process is a standard part of treatment for all pressure wounds at the study institution.
Patients were also categorized into 2 groups according to wound healing. Healing with dressing and local care was classified as “healing with medical treatment,” and healing after interventions such as surgical debridement, negative pressure wound therapy (NPWT), primary suturing, graft, or flap was classified as “healing with surgical treatment.” For the purpose of this study, “surgical/procedure-based treatment” refers to any wound management that required a procedure beyond routine dressings or local care, including sharp or surgical debridement and/or NPWT, and, when applicable, definitive closure techniques (ie, primary closure, skin grafting, or flap reconstruction).
Statistical analysis
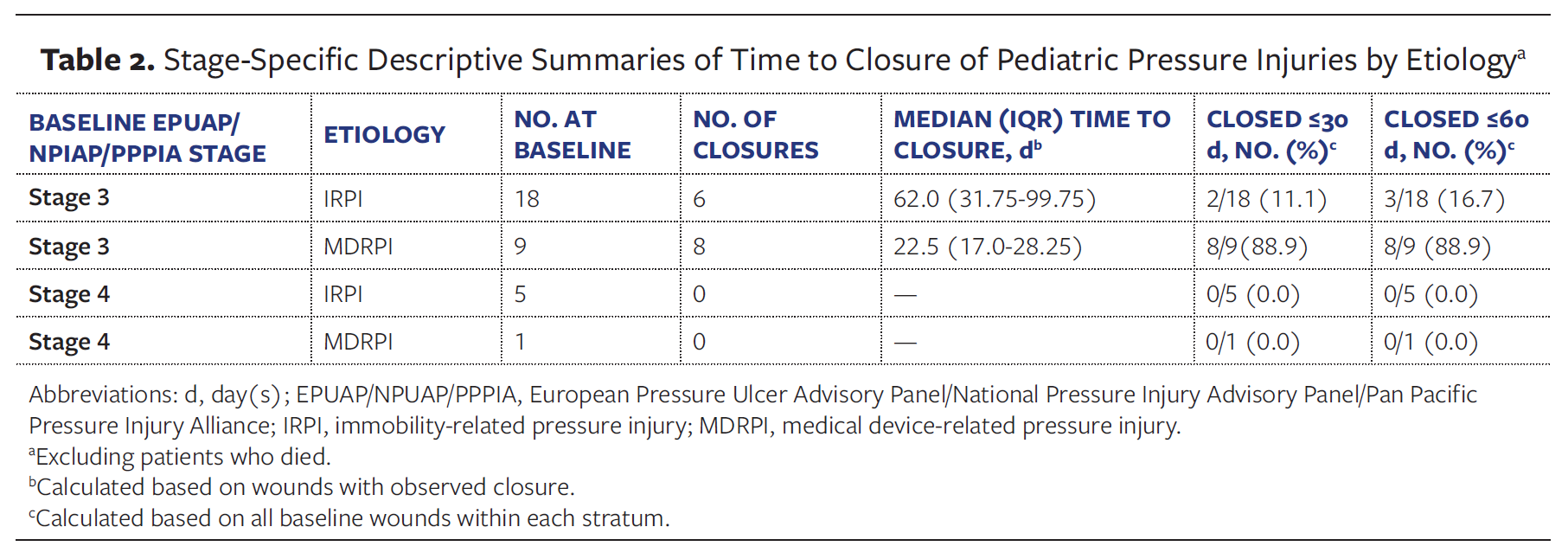
Patients in the MDRPI and IRPI groups were compared in terms of age, sex, primary diagnosis, follow-up service, wound localization, time to wound formation, wound size, wound stage, infection findings, response to treatment, and duration of treatment. The progression of DTPI to stage 3 to 4 and their corresponding times to progression were abstracted from daily wound staging forms. For wounds with baseline stage 3 to 4, median (IQR) times and the proportion of closures within 30 days and 60 days, stratified by etiology, are reported.
Statistical analysis of the collected data was performed using SPSS software version 27.0 (IBM Corporation). For comparisons between groups, an independent sample t test or Mann-Whitney U test was used for continuous variables according to the distribution of the data. The chi-square test or Fisher exact test was used for categorical variables. The level of statistical significance was set at .05.
Results
A total of 283 PIs were identified in 149 pediatric patients hospitalized at a single center between August 2020 and December 2024. Of these wounds, there were 225 in the IRPI group (128 patients) and 58 in the MDRPI group (37 patients). Sixteen patients developed both MDRPI and IRPI.
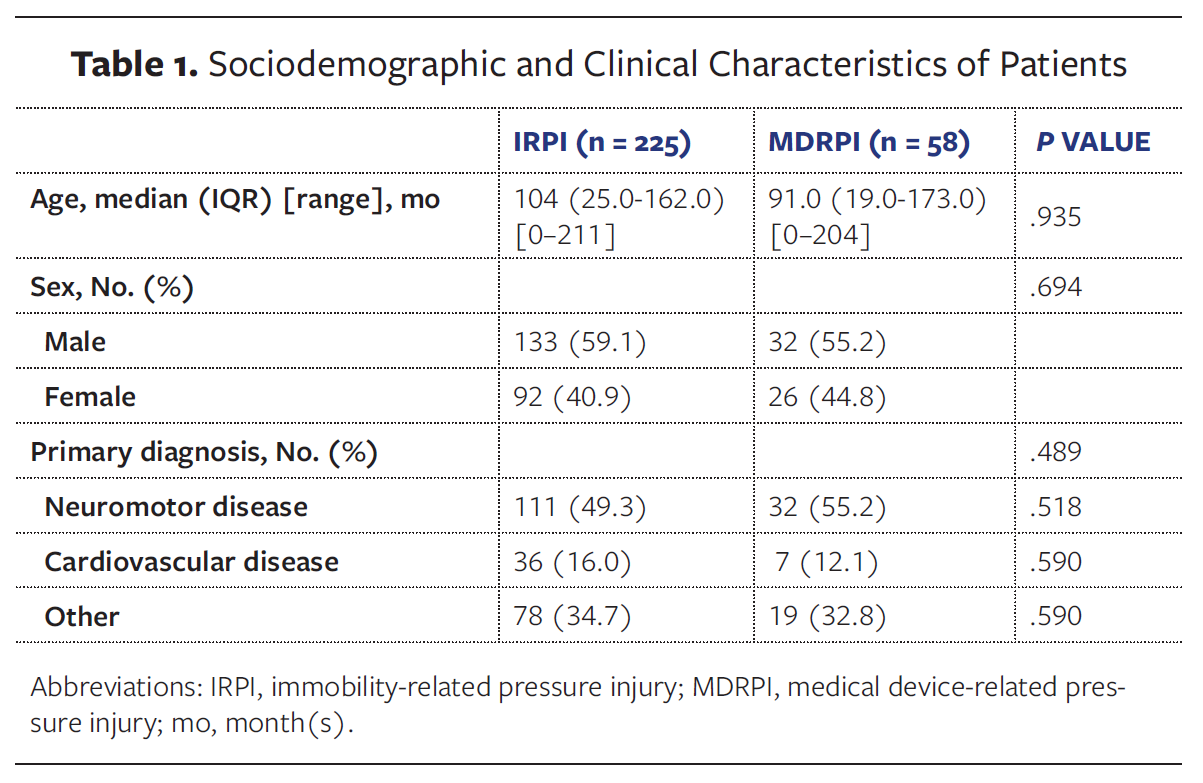
Detailed information on the sociodemographic and clinical characteristics of the patients is presented in Table 1.
Age and sex
The median (IQR) patient age was 104 months (25.0 months-162.0 months) in the IRPI group and 91.0 months (19 months-173 months) in the MDRPI group. The overall age range was 0 months to 211 months (IRPI, 0 months-211 months; MDRPI, 0 months-204 months), with a median (IQR) patient age of 104 months (23 months-166.5 months) and a mean (SD) age of 98.1 (72.0) months. There was no statistically significant difference between the 2 groups in terms of age (P = .935) or sex distribution (P = .694). In the IRPI group, 59.1% of the wounds occurred in male patients and 40.9% occurred in female patients. In the MDRPI group, 55.2% of the MDRPIs occurred in male patients and 44.8% occurred in female patients.
Primary diagnosis
The most common primary diagnosis of pressure injuries in both groups was neuromotor diseases (49.3% in the IRPI group and 55.2% in the MDRPI group). There was no difference in the risk of developing MDRPI or IRPI in children with neuromotor diseases (P = .518). The second most common diagnosis was cardiovascular diseases, and similarly, there was no difference in the risk of developing MDRPI or IRPI (P = .590). In this cohort, the risk of MDRPI vs IRPI did not differ by primary diagnosis (P = .489).
Wound localization
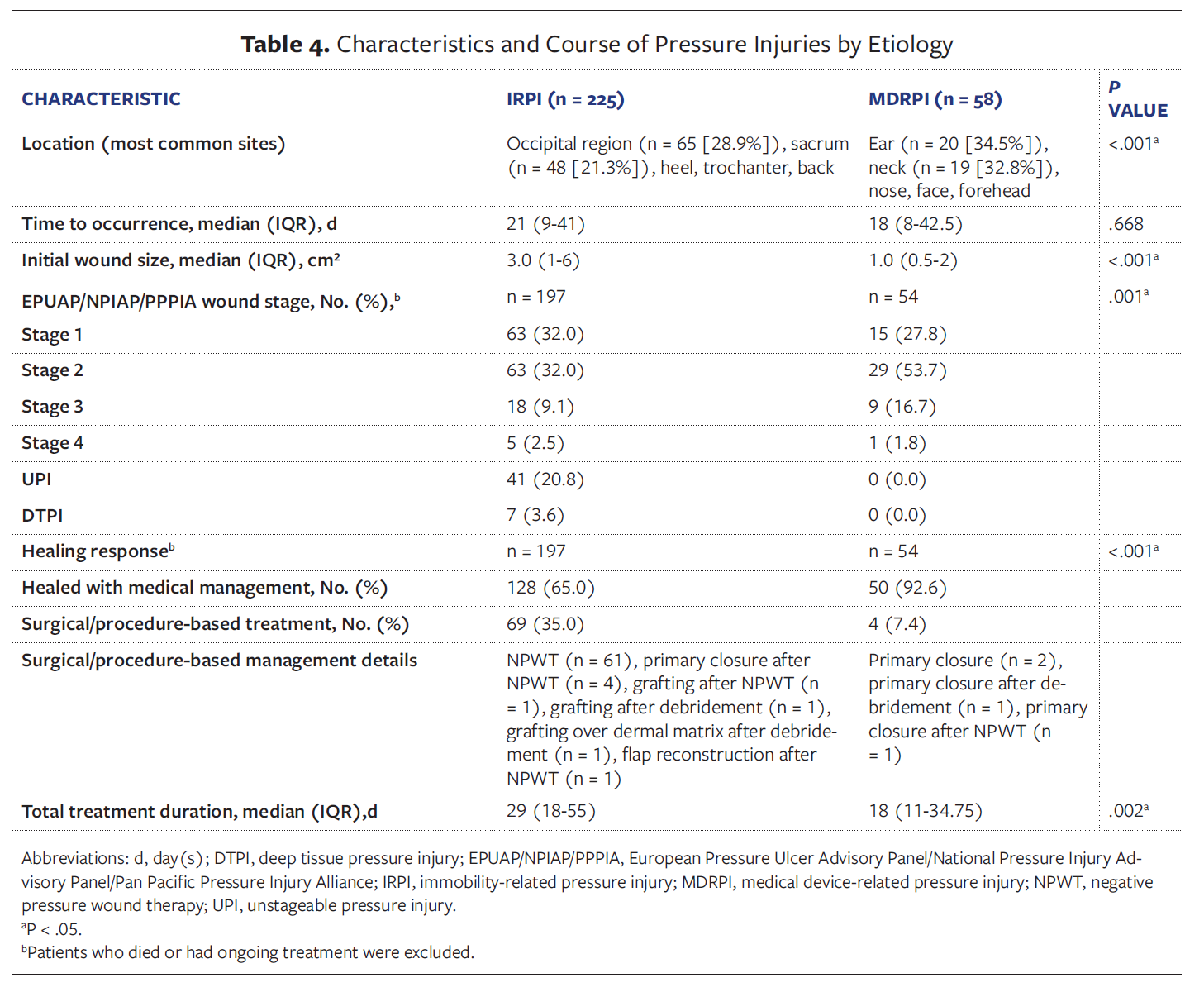
There was a marked and significant difference between the 2 groups in terms of the anatomic region of the wound (P < .001). The most common wound sites in the IRPI group were the occipital region (65 wounds) and the sacrum (48 wounds) (Figure 1), with wounds concentrated in classical compression sites. MDRPI was most commonly seen in the ear (Figure 2) and neck regions, with these sites accounting for approximately 67% of all MDRPIs.


Time to wound formation
There was no significant difference between the 2 groups in terms of time to wound formation (P = .668). The median time to wound formation was 21 days in the IRPI group and 18 days in the MDRPI group.
Wound size
Analyses based on the initial wound size in centimeters squared revealed a significant difference between the 2 groups (P < .001). The median initial wound size was 1.0 cm² in the MDRPI group and 3.0 cm² in the IRPI group (Figure 3). This finding suggests that IRPIs were significantly larger than MDRPIs at baseline.

Wound stage
There was a significant difference between the 2 groups in terms of wound stage distribution (P = .001). The majority of wounds in the MDRPI group were early-stage wounds, with stage 2 wounds comprising 53.7% of all MDRPIs. In contrast, there were no late-stage wounds in the MDRPI group, but in the IRPI group the rate of UPI and DTPI was 20.8% and 3.6%, respectively. Among initial DTPIs, 5 of 7 cases progressed to UPI within a median (IQR) of 9 days (9.0 days-17.0 days), and then progressed to stage 3 to 4 wounds within a median of 14 days (13.5 days-17.5 days). The other 2 patients died.
Infection findings
In the IRPI group, 29 of 225 wounds (12.9%) were classified as infected, whereas 196 wounds (87.1%) had no documented infection. In the MDRPI group, 5 of 58 wounds (8.6%) were classified as infected, whereas 53 wounds (91.4%) had no documented infection. Wound swab cultures were obtained only when infection was clinically suspected. There was no significant difference between the IRPI and MDRPI groups in terms of wound infection status (P = .506).
Healing response
Of the original 225 IRPI wounds, 28 were excluded from healing response analysis (24 due to death before a healing outcome could be determined; 4 due to ongoing treatment at the study end date). Of the remaining 197 IRPI wounds, 128 (65.0%) healed with medical treatment and 69 (35.0%) required surgical treatment. Of the original 58 MDRPI wounds, 4 were excluded due to death before a healing outcome could be determined. Of the remaining 54 MDRPI wounds, 50 (92.6%) healed with medical treatment and only 4 (7.4%) required surgical intervention. This result shows that wounds in the MDRPI group healed with medical treatment at a much higher rate; additionally, the rate of surgical intervention was significantly lower compared with the IRPI group (P < .001).
Among wounds in either group categorized as requiring surgical/procedure-
based management, interventions primarily consisted of NPWT (n = 61); definitive closure procedures were performed only in select cases: primary closure (n = 2), primary closure after NPWT (n = 5), primary closure after debridement (n = 1), grafting after NPWT (n = 1), grafting after debridement (n = 1), grafting over dermal matrix after debridement (n = 1), and flap reconstruction after NPWT (n = 1).
Treatment duration
The median (IQR) total treatment duration of wounds in the IRPI group was 29 days (18 days-55 days), while in the MDRPI group it was 18 days (11 days-34.75 days). This finding demonstrates that healing took longer in PIs resulting from immobility compared with those caused by medical devices (P = .002).
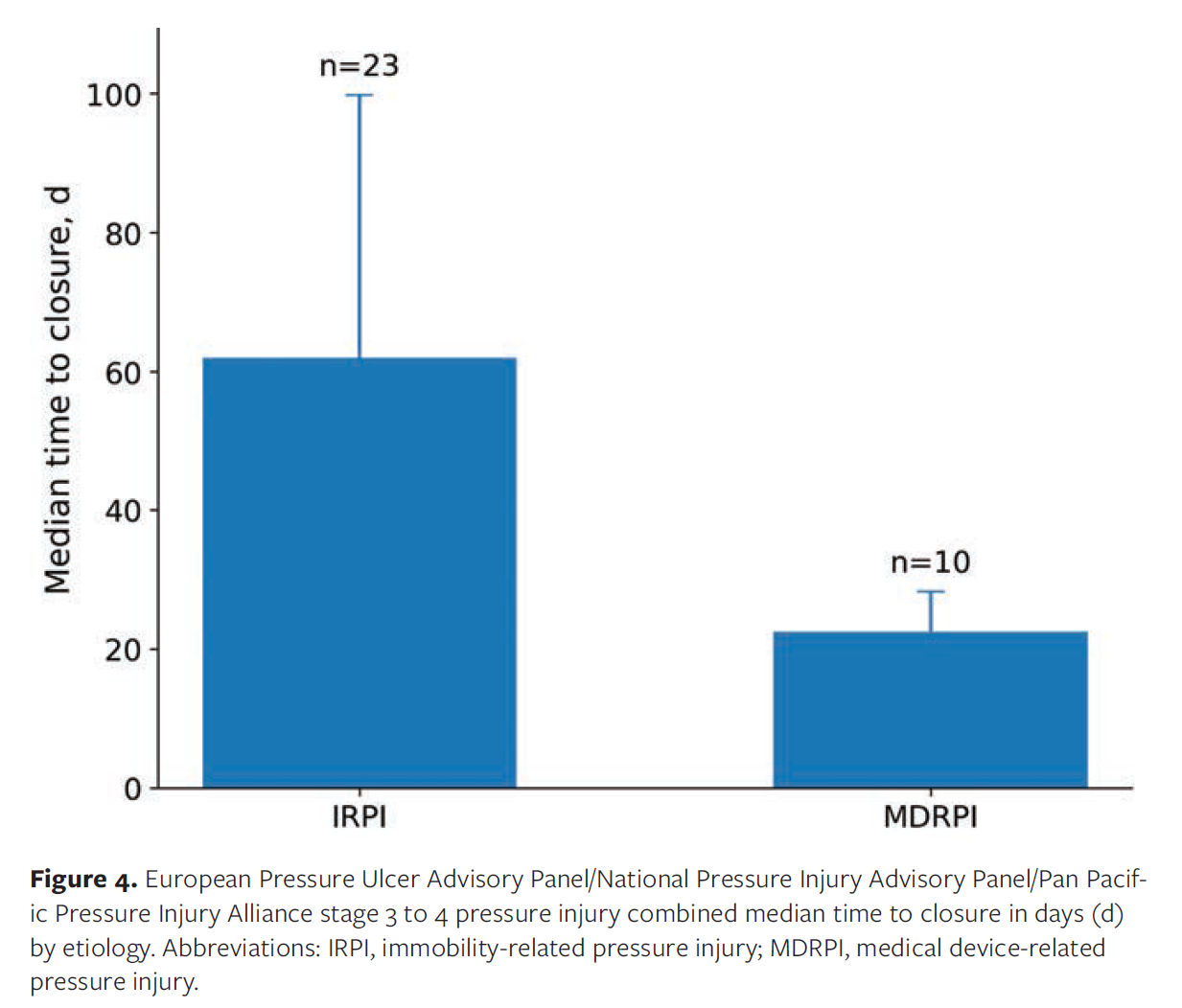
For baseline stage 3 lesions, the median (IQR) time to closure was 62.0 days (31.75 days-99.75 days) in the IRPI group (n = 18) and 22.5 days (17.0 days-28.25 days) in the MDRPI group (n = 9). No closures were observed among baseline stage 4 lesions in either group, with 5 such lesions in the IRPI group and 1 in the MDRPI group (Table 2 and Figure 4).
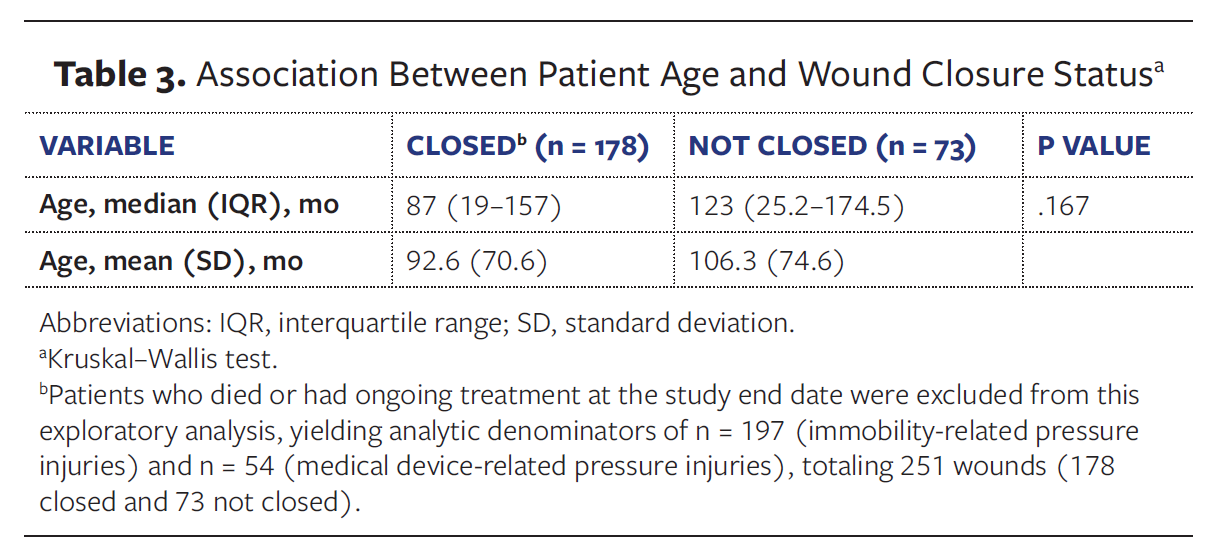
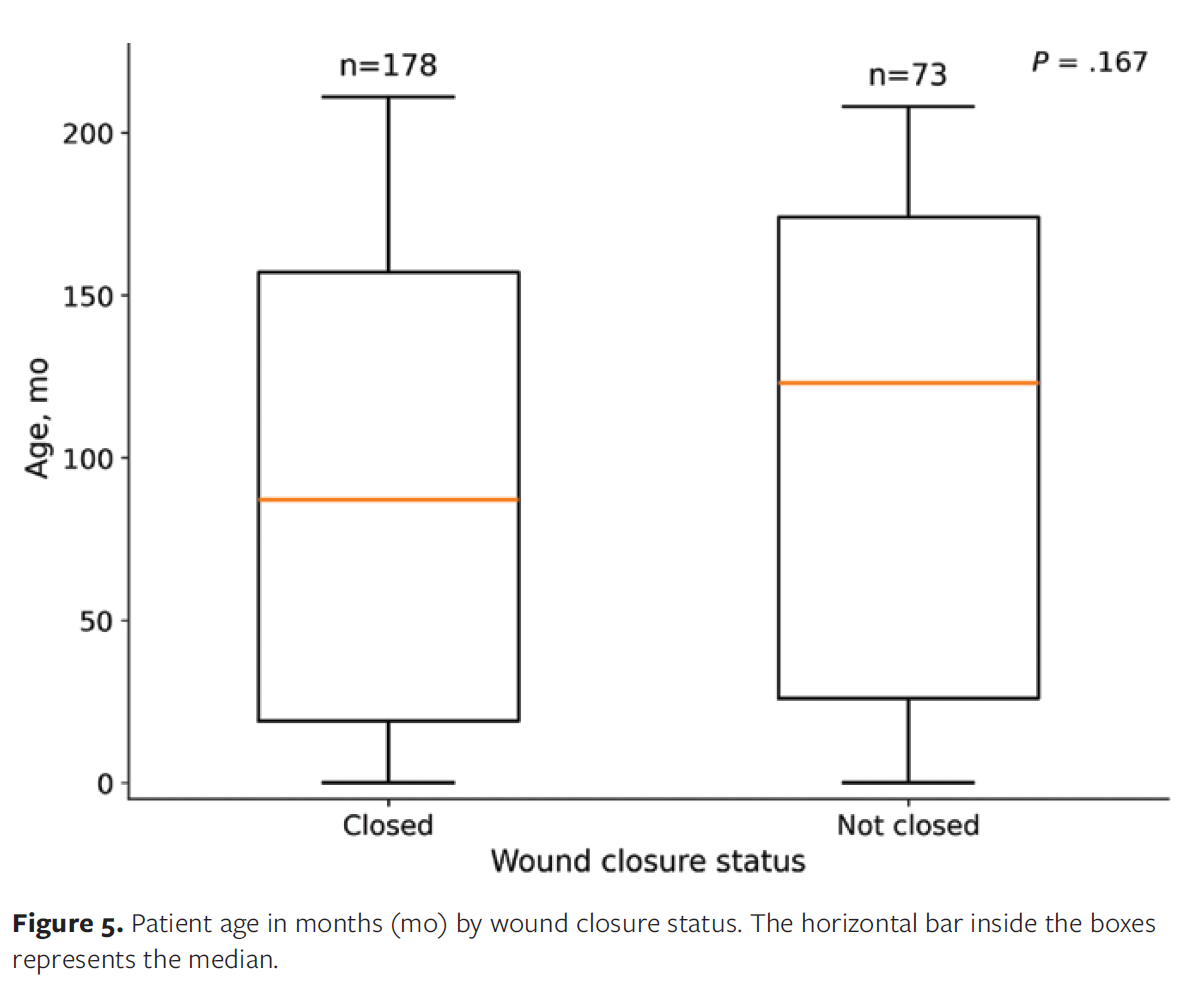
Exploratory analysis excluding deaths and wounds with ongoing management at the study end date showed that patient age was not significantly associated with wound closure status (P = .167; Table 3 and Figure 5).
Discussion
In this retrospective cohort study, PIs in hospitalized pediatric patients were divided into 2 etiologic groups (MDRPI and IRPI) and the patients’ demographic and clinical characteristics compared. The findings reveal that etiology results in significant differences in the clinical presentation and prognosis of pressure injuries in the pediatric population.
Age, sex, and primary diagnosis
In general, pressure injuries are more common in children older than 5 years of age and least common in neonates.30 Neonates are more susceptible to MDRPIs due to their unique physiologic characteristics, such as immature skin structure, weak dermoepidermal connections, and increased transepidermal fluid loss; additionally, babies born preterm are at increased risk of pressure injury.31 In the present study, although the median age was lower in the MDRPI group than in the IRPI group, this difference was not significant (P = .935). Stellar et al32 reported that two-thirds of MDRPIs in their cohort occurred in children younger than 8 years, although that study did not include a direct comparison between MDRPIs and IRPIs. The results of the current study show that when all pediatric age groups are considered, age is not a determining factor for the occurrence of MDRPI or IRPI, regardless of etiology. Similarly, neither is sex a determining factor in the development of MDRPI or IRPI (P = .694).
In the current study, the most common primary diagnoses in both groups were neuromotor disease, followed by cardiovascular disease. Children with chronic hypoxemia may be particularly vulnerable to PIs because inadequate tissue perfusion and oxygenation impair skin and subcutaneous tolerance to sustained pressure.27 We found no significant difference between MDRPIs and IRPIs in the proportion of patients with cardiovascular disease (P = .590), suggesting that circulatory compromise and hypoxia contribute similarly to both etiologic types of PI rather than preferentially promoting one over the other. To our knowledge, no published studies have directly compared MDRPI and IRPI rates among pediatric cardiology patients, and further work is needed to clarify whether specific subgroups of cardiovascular disease carry different risk profiles for each PI etiology.
Wound localization
The occipital region is a typical location for pressure injuries, especially in infants and young children, because the head is larger than the trunk.33 Adult studies have shown that the auricle and the wings of the nose are sites with a high prevalence of MDRPI,34 and care support equipment such as ventilation masks, enteral feeding tubes, nasogastric tubes, and intravenous catheters are the prominent etiologic factors.5,6,32,35 In the present study, wounds in the IRPI group were frequently located on bony prominences, such as the occipital region, sacrum, and heel. In contrast, the wounds in the MDRPI group were concentrated in areas with device contact, such as the ear, neck, nose, and face (P < .001). These localization differences demonstrate the specific effects of etiologic factors on the mechanism of wound formation and thus, the areas where preventive strategies should be targeted.36 This emphasizes the need to develop special protocols to protect skin integrity in the application of medical devices in pediatric patients.
Time to occurrence
Although some literature exists on the time to PI formation in the pediatric population, detailed studies directly comparing the time to formation according to IRPI and MDRPI etiologies are limited. Some prior pediatric studies have reported that PIs in intensive care settings can develop relatively early during admission, particularly when pressure-relief and skin-care interventions are not prioritized in the first days of care.²⁷,³⁷ However, because of increased awareness of this issue and the incorporation of preventive measures, more recent studies indicate a longer duration to PI occurrence.³⁸
In the current study, the median time to MDRPI was 18 days and to IRPI was 21 days (P = .668). This finding of the current study suggests that PIs occur at relatively similar times in pediatric patients regardless of etiology and that the physiological factors involved in wound formation (eg, circulatory failure, tissue tolerance, general condition of the patient) lead to tissue damage at a similar rate in both wound types.
In the current study, MDRPIs were generally smaller at baseline and were more frequently staged as early lesions, which, together with routine checks of areas of device-skin contact, likely facilitated earlier recognition and timely device adjustments. This finding aligns with the shorter time to resolution for MDRPI compared with IRPI.
Wound size
Comparative analyses of the size of pressure injuries are rare. In an adult study including mucous ulcers, MDRPIs were reported to be small (≤2 cm2).38 In the current research, IRPIs were significantly larger than MDRPIs (Table 4). This finding suggests a direct association between wound etiology and wound size. The observed differences in wound size may be related to the mechanisms of wound formation. IRPIs usually develop as a result of prolonged pressure over a larger area. Sustained and distributed pressure on bony prominences can lead to ischemia and damage over a larger area of tissue. In contrast, MDRPIs are usually caused by localized and concentrated pressure or friction from medical devices. The pressure exerted by these devices is generally concentrated in a smaller, specific area, which may result in initially smaller wound sizes. This finding highlights the importance of etiology-specific approaches for the prevention and management of pressure injuries in the pediatric population. Prevention of larger and potentially more severe IRPIs requires comprehensive positioning and pressure distribution strategies.39 In contrast, in the case of MDRPIs, proper device selection, placement, and regular monitoring may play a critical role in limiting the development and size of wounds.12
Wound stage
Stage 1 and stage 2 pressure injuries are most commonly seen in children.12,35 In the present study, analysis of wound stage distributions showed that the majority of MDRPIs were early-stage injuries (especially stage 2), whereas advanced stage wounds such as UPIs and DTPIs only occured in IRPIs (P = .001). That MDRPIs usually remain or are detected at superficial stages may be explained by the fact that they are easily recognizable due to the direct contact of the devices with the skin. Thus, the chance of early intervention is high.16 Because the pressure applied by medical devices is usually localized, tissue damage may initially remain more limited and superficial. In contrast, the high incidence of later-stage IRPIs may be due to the potential for deeper tissue damage because of the nature of these injuries. This suggests a need for more aggressive and comprehensive treatment approaches in the management of IRPIs.
Infection
Infection is a significant complication that increases morbidity in pediatric pressure injuries. Infection or colonization of pressure injuries with microorganisms frequently occurs and, if left untreated, may lead to cellulitis, osteomyelitis, and sepsis.40 Although a prospective study in a small MDRPI group (which included mucosal PIs) reported no infection,38 that is an adult study. The pediatric literature is limited. In the present study, the infection rate was 12.9% in the IRPI group and 8.6% in the MDRPI group. This difference was not significant (P = .506). The findings of the current study indicate that the risk of infection in PIs is similar regardless of etiology. This suggests that all PIs should be followed up at a similar level in an effort to prevent infection, and necessary prophylactic or therapeutic measures should be taken. The results of the current study suggest that the patient’s general condition, underlying diseases, and wound care practices may be more determinant than wound etiology in the development of infection.
Healing response
The stage and severity of the wound usually determine the treatment approach for pressure injuries in pediatric patients. In the literature, it has been reported that most pressure injuries in children can heal spontaneously. However, severe wounds such as stage 3 or 4 or those that do not respond to conservative treatment may require surgical intervention.3 Similarly, it has been emphasised that superficial pressure injuries (stages 1 and 2) are usually treated conservatively. However, more advanced injuries (eg, stages 3 and 4) may require more aggressive surgical approaches, such as debridement and flap closure.41 The present study shows a high rate of healing of MDRPIs with medical treatment and that surgical treatment is rarely needed (P < .001). These findings are consistent with the findings regarding wound stage. While conservative approaches are usually sufficient for early-stage MDRPIs, surgical interventions may be more frequently required for IRPIs, which may be more profound and more complex. The fact that MDRPIs are often seen in the early stages (especially stage 2) may explain why a large proportion of these wounds respond well to medical treatment and are less likely to require surgery. Interventions such as early removal of medical devices or proper positioning can positively affect the prognosis of such wounds. In contrast, the higher incidence of IRPIs in more advanced stages may be the main reason these wounds are more likely to require surgical intervention.
Recovery time
The findings of the current study suggest that IRPIs take longer to heal compared with MDRPIs. As noted previously, the fact that MDRPIs are usually detected at earlier stages and have a smaller initial size may contribute to the shorter resolution time of these wounds. Indeed, it is recognized that more superficial wounds have the potential to heal faster than more advanced wounds. Conversely, prolonged treatment times with IRPIs may be due to the often advanced stage of these injuries (UPI, DTPI) and the increased need for surgical intervention.3 The findings of the current study emphasize that determining treatment plans and risk management strategies based on wound etiology may result in more effective and faster wound healing in pediatric patients. In this exploratory analysis, patient age alone was not significantly associated with wound closure, suggesting that wound-related factors (eg, baseline stage/severity, etiology, size, infection, management) may be more informative determinants of closure than chronologic age in hospitalized pediatric patients.
Limitations
The single-center, retrospective design of this study may limit the generalizability of the findings. Although pressure injury staging in the study hospital is performed by specialist wound care nurses using standardized criteria and is supported by serial clinical documentation, some degree of misclassification cannot be entirely ruled out due to the retrospective design. Neonatal cases constituted a small proportion of the cohort; therefore, neonatal-specific etiologic patterns (particularly device-related injuries in patients receiving respiratory support) may not be fully captured, and findings should be interpreted with caution for NICU populations. In addition, as a common limitation of retrospective studies, some clinical details may have been incompletely documented in the original medical records at the time of patient care, and such missing information cannot be retrieved retrospectively. Due to the retrospective nature of the study, the effects of specific interventions or wound care protocols on wound healing times could not be evaluated in detail.
Conclusion
This retrospective cohort study found significant clinical differences based on the etiology of pressure injuries in pediatric patients. The study contributes to the limited published data on pediatric PIs. It fills a significant gap, especially in the comparison of etiology-based characteristics, treatment responses, and healing times. The significant differences between IRPIs and MDRPIs in terms of localization, initial wound size, wound stage, healing response, and treatment duration suggest the need to adopt etiology-specific treatment strategies for pediatric PIs and the importance of developing risk management protocols specific to each wound type In particular, MDRPIs are detected at an earlier stage and generally heal more rapidly, suggesting that early diagnosis and appropriate device management of these wounds is critical. This approach provides the basis for strategies to increase and standardize preventive measures, especially in PICUs, where medical device use is an everyday occurrence.
This in-depth analysis based on the etiological classification of pressure injuries in pediatric patients provides a scientific basis for the development of more personalized and effective interventions in clinical practice. Future prospective, multicenter studies are needed to confirm these findings and to examine the long-term outcomes of these wound types in pediatric populations in different age groups and with different underlying diseases.
Author and Public Information
Authors: Mehmet Can, MD1; İlknur Mert, MSN, RN2; Özkan Okur, MD1; Arzu Şencan, MD1; Hasan Ağın, MD3; Sinem Akbay Ak, MD4; Nilgün Harputluoğlu, MD5; and Hurşit Apa, MD6
Affiliations: 1Pediatric Surgery Department, Dr Behçet Uz Pediatric Diseases and Surgery Training and Research Hospital, Izmir, Turkey; 2Pediatric Wound Care, Dr Behçet Uz Pediatric Diseases and Surgery Training and Research Hospital, Izmir, Turkey; 3Pediatric Intensive Care Unit, Dr Behçet Uz Pediatric Diseases and Surgery Training and Research Hospital, Izmir, Turkey; 4Department of Neonatology, Dr Behçet Uz Pediatric Diseases and Surgery Training and Research Hospital, Izmir, Turkey; 5Pediatric Palliative Care Unit, Dr Behçet Uz Pediatric Diseases and Surgery Training and Research Hospital, Izmir, Turkey; 6Pediatric Emergency Department, Dr Behçet Uz Pediatric Diseases and Surgery Training and Research Hospital, Izmir, Turkey
Disclosures: The authors disclose no financial or other conflicts of interest.
Ethics Statement: Informed consent was obtained from the parents of each patient, and this study was reviewed and approved by the ethics committee of the Dr Behçet Uz Pediatric Diseases and Surgery Training and Research Hospital.
Corresponding Author: Mehmet Can; MD; Pediatric Surgery Department, Dr Behçet Uz Pediatric Diseases and Surgery Training and Research Hospital, Ismet Kaptan Mah., Sezer Dogan Sok. No:11, 35210 Konak, İzmir, Turkey; mcan72@live.com
Manuscript Accepted: April 7, 2026
References
- Sarsak HI. Review of pressure ulcers management in pediatrics: assessment, prevention, and intervention. J Pediatr Neonatal Care. 2018;8(5):245-248. doi:10.15406/jpnc.2018.08.00350
- Delmore B, VanGilder C, Koloms K, Ayello EA. Pressure injuries in the pediatric population: analysis of the 2008–2018 international pressure ulcer prevalence survey data. Adv Skin Wound Care. 2020;33(6):301-306. doi:10.1097/01.ASW.0000661812.22329.f9
- Pignatti M, D’Arpa S, Roche N, et al. Surgical treatment of pressure injuries in children: a multicentre experience. Wound Repair Regen. 2021;29(6):961-972. doi:10.1111/wrr.12964
- Luo WJ, Zhou XZ, Lei JY, Xu Y, Huang RH. Predictive risk scales for development of pressure ulcers in pediatric patients admitted to general ward and intensive care unit. World J Clin Cases. 2021;9(35):10956-10968. doi:10.12998/wjcc.v9.i35.10956
- Marufu TC, Setchell B, Cutler E, et al. Pressure injury and risk in the inpatient paediatric and neonatal populations: a single centre point-prevalence study. J Tissue Viability. 2021;30(2):231-236. doi:10.1016/j.jtv.2021.02.004
- Semerci R, Umaç EH, Yılmaz D, Karadağ A. Analysis of the prevalence and risk factors of pressure injuries in the hospitalized pediatric population: a retrospective study. J Tissue Viability. 2023;32(3):333-338. doi:10.1016/j.jtv.2023.04.004
- Baldwin KM. Incidence and prevalence of pressure ulcers in children. Adv Skin Wound Care. 2002;15(3):121-124. doi:10.1097/00129334-200205000-00007
- Delmore B, Deppisch M, Sylvia C, Luna-Anderson C, Nie AM. Pressure injuries in the pediatric population: a national pressure ulcer advisory panel white paper. Adv Skin Wound Care. 2019;32(9):394-408. doi:10.1097/01.ASW.0000577124.58253.66
- Garncarczyk AA, Adamczyk K, Lubczyńska A, Wcisło-Dziadecka D, Antończak P, Jakubowska M. Structure of children’s skin and rules for its care–what’s new? Children’s skin structure. Pol J Paediatr. 2021;96(4):258-262. doi:10.5114/polp.2021.112400
- Klein C, Marie-Christine P. Challenges in the management of infected wounds in children. J Wound Care. 2021;30(6):427-428. doi:10.12968/jowc.2021.30.6.427
- Boylan C. Paediatric pressure injuries: considerations for this patient cohort. Wound Pract Res. 2020;28(2):84-89.
- Ramos GW, Monteiro DR, Rodrigues PO, Wegner W, Breigeiron MK. Pressure ulcers in pediatric patients: causal factors and therapeutic management. Cogitare Enfermagem. 2023;28:e86780. doi:10.1590/ce.v28i0.90401
- Dessi F, Valeille J, Beloni P, Toniolo J. Assessment tools for the risk of pressure injury in children: a systematic review. Int J Nurs Stud Adv. 2025;9:100410. doi:10.1016/j.ijnsa.2025.100410
- Puspitasari JD, Nurhaeni N, Waluyanti FT. Testing of Braden QD Scale for predicting pressure ulcer risk in the pediatric intensive care unit. Pediatr Rep. 2020;12(Suppl 1):8694. doi:10.4081/pr.2020.8694
- Freundlich K. Pressure injuries in medically complex children: a review. Children (Basel). 2017;4(4):25. doi:10.3390/children4040025
- Pittman J, Gillespie C. Medical device-related pressure injuries. Crit Care Nurs Clin North Am. 2020;32(4):533-542. doi:10.1016/j.cnc.2020.08.004
- Mehta C, Ali M, Mehta Y, George JV, Singh MK. MDRPU-an uncommonly recognized common problem in ICU: a point prevalence study. J Tissue Viability. 2019;28(1):35-39. doi:10.1016/j.jtv.2018.12.002
- Najjar YW, Saleh MY, Hassan ZM. Medical device related pressure ulcers in Jordan: prevalence study among critically ill patients. Health Sci Rep. 2022;5(3):e620. doi:10.1002/hsr2.620
- Brophy S, Moore Z, Patton D, O’Connor T, Avsar P. What is the incidence of medical device-related pressure injuries in adults within the acute hospital setting? A systematic review. J Tissue Viability. 2021;30(4):489-498. doi:10.1016/j.jtv.2021.03.002
- Saleh MYN, Ibrahim EIM. Prevalence, severity, and characteristics of medical device related pressure injuries in adult intensive care patients: a prospective observational study. Int Wound J. 2023;20(1):109-119. doi:10.1111/iwj.13845
- Black JM, Cuddigan JE, Walko MA, Didier LA, Lander MJ, Kelpe MR. Medical device related pressure ulcers in hospitalized patients. Int Wound J. 2010;7(5):358-365. doi:10.1111/j.1742-481X.2010.00699.x
- Kim JY, Lee YJ; Korean Association of Wound Ostomy Continence Nurses. Medical device-related pressure ulcer (MDRPU) in acute care hospitals and its perceived importance and prevention performance by clinical nurses. Int Wound J. 2019;16(Suppl 1):51-61. doi:10.1111/iwj.13023
- McAuliffe PB, Winter EE, Talwar AA, Desai AA, Broach RB, Fischer JP. Pressure ulcer trends in the United States: a cross-sectional assessment from 2008-2019. Am Surg. 2023;89(12):5609-5618. doi:10.1177/00031348231158691
- Zhang S, Wei G, Han L, Zhong W, Lu Z, Niu Z. Global, regional and national burden of decubitus ulcers in 204 countries and territories from 1990 to 2021: a systematic analysis based on the global burden of disease study 2021. Front Public Health. 2025;13:1494229. doi:10.3389/fpubh.2025.1494229
- European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. The International Guideline. Haesler E, ed. EPUAP/NPIAP/PPPIA; 2019.
- Gould LJ, Alderden J, Aslam R, et al. WHS guidelines for the treatment of pressure ulcers: 2023 update. Wound Repair Regen. 2024;32(1):6-33. doi:10.1111/wrr.13130
- Curley MAQ, Quigley SM, Lin M. Pressure ulcers in pediatric intensive care: incidence and associated factors. Pediatr Crit Care Med. 2003;4(3):284-290. doi:10.1097/01.PCC.0000075559.55920.36
- Neuhaus K, Meuli M, Koenigs I, Schiestl C. Management of “difficult” wounds. Eur J Pediatr Surg. 2013;23(5):365-374. doi:10.1055/s-0033-1354588
- Schlüer AB, Schols JMGA, Halfens RJG. Pressure ulcer treatment in pediatric patients. Adv Skin Wound Care. 2013;26(11):504-510. doi:10.1097/01.ASW.0000433103.55891.af
- Razmus I, Bergquist-Beringer S. Pressure injury prevalence and the rate of hospital-acquired pressure injury among pediatric patients in acute care. J Wound Ostomy Continence Nurs. 2017;44(2):110-117. doi:10.1097/WON.0000000000000306
- Visscher M, Taylor T. Pressure ulcers in the hospitalized neonate: rates and risk factors. Sci Rep. 2014;4:7429. doi:10.1038/srep07429
- Stellar JJ, Hasbani NR, Kulik LA, et al. Medical device–related pressure injuries in infants and children. J Wound Ostomy Continence Nurs. 2020;47(5):459-469. doi:10.1097/WON.0000000000000683
- Manning MJ, Gauvreau K, Curley MAQ. Factors associated with occipital pressure ulcers in hospitalized infants and children. Am J Crit Care. 2015;24(4):342-348. doi:10.4037/ajcc2015349
- Galetto SGS, Nascimento ERP, Hermida PMV, Busanello J, Malfussi LBH, Lazzari DD. Medical device-related pressure injuries in critical patients: prevalence and associated factors. Rev Esc Enferm USP. 2021;55:e20200397. doi:10.1590/1980-220X-REEUSP-2020-0397
- Smith HA, Moore Z, Tan MH. Cohort study to determine the risk of pressure ulcers and developing a care bundle within a paediatric intensive care unit setting. Intensive Crit Care Nurs. 2019;53:68-72. doi:10.1016/j.iccn.2019.04.008
- Gou L, Zhang Z, A Y. Risk factors for medical device-related pressure injury in ICU patients: a systematic review and meta-analysis. PLoS One. 2023;18(6):e0287326. doi:10.1371/journal.pone.0287326
- Baharestani MM, Ratliff CR. Pressure ulcers in neonates and children: an NPUAP white paper. Adv Skin Wound Care. 2007;20(4):208-220. doi:10.1097/01.ASW.0000266646.43159.99
- Coyer FM, Stotts NA, Blackman VS. A prospective window into medical device-related pressure ulcers in intensive care. Int Wound J. 2014;11(6):656-664. doi:10.1111/iwj.12026
- Andayani RP, Wahyuni F, Ausrianti R, Reni I, Edo CWD, Amir H. Effectiveness of virgin coconut oil and regular repositioning in preventing pressure ulcers in children. Med J Malaysia. 2023;78(4):511-514.
- Okamoto S, Ogai K, Mukai K, Sugama J. Association of skin microbiome with the onset and recurrence of pressure injury in bedridden elderly people. Microorganisms. 2021;9(8):1603. doi:10.3390/microorganisms9081603
- Ciprandi G, Oranges T, Schluer AB. Pressure ulcers in pediatric patients. In: Romanelli M, Clark M, Gefen A, Ciprandi G, eds. Science and Practice of Pressure Ulcer Management. Springer; 2018. doi:10.1007/978-1-4471-7413-4_10







