



Patient and Nurse Perceptions of a Bordered Silicone Superabsorbent Polymer Dressing for Pressure Injury Prevention: A Prospective Noncomparative Pilot Study in a Long-Term Acute Care Hospital
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Prophylactic dressings for pressure injury (PI) prevention have been investigated in a range of hospital settings, but there is limited evidence supporting their use in long-term acute care (LTAC) hospitals. Objective. To evaluate patient and nurse perceptions of incorporating a bordered silicone superabsorbent polymer (SAP) dressing into an LTAC PI prevention protocol. Materials and Methods. This pilot study included 50 adult patients at risk for sacral PIs, with intervention and data collection occurring between January 2024 and April 2025. Dressings were applied to the sacrum, with assessments at least daily and dressing changes no less than every 7 days. Patient- and nurse-reported outcomes (primary outcomes) included comfort, satisfaction, and usability indices. Secondary outcomes included PI incidence, adverse events, and dressing utilization. Results. The median follow-up was 15 days, with a median of 6 dressings used per patient. Patients reported minimal discomfort, and approximately 90% rated comfort and satisfaction as good-to-excellent. Nursing staff also reported high usability. No PIs or device-related serious adverse events occurred. Conclusion. The bordered silicone SAP dressing was well-tolerated by patients and nursing staff within an LTAC PI prevention protocol. These findings support its consideration for integration into prevention protocols. Further research is needed to evaluate comparative PI reduction and adverse events.
Patients in long-term acute care (LTAC) hospitals are at high risk of developing pressure injuries (PIs) due to their complex medical needs, prolonged immobility, and high prevalence of incontinence. An assessment across care settings showed that LTAC hospitals had the highest overall prevalence of hospital-acquired PI (HAPI).1 HAPIs are considered preventable “never events” that should not occur if appropriate preventive measures are implemented.2,3
In recognition that impaired mobility is a key contributor to PIs,4 clinical practice guidelines emphasize the need to manually reposition patients at regular intervals and to encourage early patient mobilization.5-8 Although repositioning and mobilization can mitigate sustained pressure, not all patients can tolerate these levels of movement, and guidelines emphasize that PI prevention requires a multifactorial approach involving regular skin assessment, repositioning, moisture management, nutritional support, and use of support surfaces.5-10 The implementation of PI prevention strategies addressing multiple risk factors has led to marked reductions in PI prevalence.11
In recent years, prophylactic dressings have emerged as a potential adjunctive measure to protect skin in high-risk anatomical areas, such as the sacrum or heels. The prophylactic use of dressings has been investigated in patients in acute care settings (eg, emergency department, intensive care unit [ICU], operating room, spinal surgery and neurosurgery-emergency department or ICU), as well as in elderly patient populations.12 These dressings are applied to intact skin over high-risk anatomical sites, such as the sacrum or heels, to reduce mechanical forces including pressure, shear, and friction. By providing a cushioning interface and redistributing loads, they complement standard interventions such as repositioning and moisture management. Evidence from acute and postacute care settings suggests that prophylactic dressings may reduce PI incidence, but effectiveness can vary by patient population, anatomical site, and adherence to broader prevention protocols.13-16
Bordered silicone superabsorbent polymer (SAP) dressings, such as Zetuvit Plus Silicone Border (Hartmann USA, Inc), are candidates for prophylactic dressings for PI prevention due to their mechanical cushioning properties and ability to redistribute pressure more effectively than conventional foam dressings. Their multilayer design, incorporating an SAP core, reduces peak stresses on bony prominences and mitigates tissue deformation under sustained loading, while the silicone interface ensures atraumatic application and removal. Evidence from computational modeling indicates that bordered silicone SAP performs at least as well as, and in some aspects better than, 4 different multilayered silicone foam dressings for PI prevention. Using an anatomically realistic finite element model, Gefen et al17 demonstrated that bordered silicone SAP achieved high protective efficacy, endurance under prolonged loading, and optimal performance after moisture exposure, all critical factors for real-world clinical conditions.
Although prophylactic dressings have been increasingly adopted in acute care hospitals, there is limited evidence regarding their tolerability and effectiveness in LTAC patient populations, where unique patient risk profiles and prolonged exposure to pressure may influence use and outcomes. To address this gap and to evaluate the acceptability of an investigational dressing, this pilot study evaluated the feasibility of incorporating a bordered silicone SAP dressing, applied to the sacral area, in a PI prevention protocol at an LTAC hospital.
Materials and Methods
Study design and setting
This pilot study was an open, noncomparative, prospective clinical investigation to evaluate the acceptability of a PI prevention protocol incorporating a bordered silicone SAP dressing in Spaulding Hospital for Continuing Medical Care, an LTAC hospital in Cambridge, MA (hereafter referred to as Spaulding Cambridge). The details of the protocol are provided as an electronic supplement to this article.
Acceptability measures included nurse ratings of dressing performance and satisfaction, and patient ratings of comfort and satisfaction. The intervention and data collection took place from January 2024 through April 2025. Patients could remain in the prevention protocol until the earliest of end of study period (30 days after last patient screening date), discharge, occurrence of a sacral PI, occurrence of any adverse reaction to the dressing, or withdrawal of consent. This was a descriptive clinical study to assess categorical and qualitative end points, and no statistical hypothesis testing was planned. The study was reviewed and approved by the Mass General Brigham Institutional Review Board.
The study was conducted at Spaulding Cambridge, an LTAC hospital specializing in intensive rehabilitation and complex medical treatment over extended stays. The patient population at this hospital consists of individuals who require ongoing hospital-level care. Many patients are chronically and critically ill, and they cannot be safely managed in other settings, such as acute inpatient rehabilitation, skilled nursing facilities, or home care, due to medical instability or the need for intensive nursing support. Patients admitted to Spaulding Cambridge typically have experienced an ICU stay of 3 days or longer, have spent at least 20 days in an acute care hospital, and require daily physician oversight for their medical needs.
Following admission or significant changes to patients’ health, patients were screened for eligibility by trained nursing staff using predefined inclusion and exclusion criteria, which were verified at the baseline assessment. Participants were eligible for inclusion if they were at risk for developing a PI, as determined by clinical judgment and Braden Scale risk assessments. At Spaulding Cambridge, the standard of care designates patients with a Braden Scale score of less than or equal to 18 as being at risk for PI. Additionally, patients may be classified as at-risk regardless of their Braden Scale score if they present with factors that compromise independent mobility, such as the presence of medical devices (eg, tubes, drains, splints), or if they are receiving medications known to elevate integumentary risk, including chemotherapy and corticosteroids. Additional inclusion criteria included being predominantly bedbound or chairbound, aged 18 years or older, and able to provide consent either personally or through a legal representative. Patients were excluded if they had an existing sacral PI classified as stage 1 through 4, deep tissue injury, or unstageable PI at baseline, or if they had a known or suspected sensitivity to any component of the dressing under evaluation. Informed consent was obtained at the screening visit prior to any study procedures. Participation was voluntary, and withdrawal was permitted at any time.
During the study period, the nursing staff was comprised of 77% nurses with baccalaureate degrees, 19% with associate degrees, and 4% with master’s degrees. Notably, 25% of nurses employed during the study had completed the Wound, Ostomy, and Continence Nurses Society Wound Treatment Associate coursework. All nursing staff were expected to participate in the study when assigned to a study participant during their shift. In-service education regarding the study protocol, dressing application, and data collection was provided to nurses on all shifts, as well as to nurse clinical leads, overnight and weekend nurse supervisors, and nurse educators.
Sacral dressings
Bordered silicone SAP dressing is a sterile, self-adhesive, multilayer dressing with a semipermeable polyurethane backing, soft silicone interface, cellulose-based absorbent core with superabsorbent polyacrylate, hydrophilic and hydrophobic nonwovens, and adhesive borders. A sacrum-shaped dressing was used to conform to the sacral area for PI prevention. Dressings were applied to intact skin and could remain in place for up to 7 days per clinical protocol. The study protocol was designed to minimally affect the site’s standard of care, including concurrent PI prevention strategies. Nursing staff were instructed to inspect sacral skin at least daily by lifting the dressing, observing sacral skin as per standard of care, and reapplying the dressing. Dressings were permitted to be changed at any time at the discretion of the nursing staff in consideration of factors such as hygiene, adhesion, and patient comfort.
Study assessments
A description of the contents of the case report form (CRF) is provided in the summary of the study protocol as an electronic supplement to this article. Baseline and recurring CRFs were provided as paper-based assessments to be completed by nursing staff. Following screening and consenting, a baseline assessment was conducted. Risk for PI development was assessed using the Braden Scale, and baseline sacral photographs were obtained. Medical history and comorbidities were abstracted from the medical record into the study CRF. Following the baseline assessment, the investigational dressing was applied to the sacrum. At each dressing change, nursing staff were instructed to complete study assessments of changes in patient comfort, dressing performance, skin integrity, moisture status, and presence of erythema, discoloration, or other early signs of PI.
Dressing acceptability was assessed through patient reports of comfort and satisfaction and nurse reports of dressing performance and clinical satisfaction. After 2 weeks, or at the time of withdrawal or discharge, patients were asked to rate their perceptions of dressing comfort and satisfaction. Nursing staff completed a structured questionnaire assessing ease and speed of application, accuracy of positioning, stay-in-place performance, conformability to body contours, coverage of bony prominence, atraumatic removal, adherence to skin, and overall impression. For patient and nurse assessments of acceptability, respondents were requested to rate each question on a 5-point Likert scale (1=very poor, 2=poor, 3=good, 4=very good, 5=excellent). Ratings of “good,” “very good,” or “excellent” were considered consistent with “acceptable.” The instruments were developed specifically for this pilot study, which serves as a field pretest and represents the baseline administration of these newly developed measures. The measures of satisfaction in the present study was consistent with assessments of dressing satisfaction in the peer-reviewed literature.18-20 Internal consistency was preliminarily assessed using Cronbach alpha. Future research will include comprehensive psychometric testing to ensure the measures accurately assess comfort, satisfaction, and performance. In addition to inquiring about comfort and satisfaction, nursing staff inquired about the experience of any pain or discomfort at each dressing change. If pain or discomfort were reported, additional questions documented the intensity of discomfort using the numerical rating scale (NRS) (score range: 0-10, with 10 indicating the worst pain) and qualitative descriptors in the patient’s own words. The NRS is a commonly used and validated approach to evaluating pain severity.21
Safety and effectiveness outcomes were evaluated as a secondary objective. For effectiveness, the sacral skin was monitored for the occurrence of PIs, per the standard of care. Adverse events potentially related to the dressing and serious adverse events were recorded in both the medical record and the CRFs. In addition, dressing utilization metrics were evaluated as secondary outcomes. Indices of dressing utilization included total dressings used, total duration of dressing use, and calculated average wear time (ie, duration of enrollment divided by the number of dressings used).
Analysis
This pilot study was intended to provide preliminary evidence of the clinical acceptability of the intervention dressings from patient and nursing perspectives in an LTAC hospital. The clinical acceptability outcomes include quantitative and qualitative indices. No formal statistical analyses were conducted for the purpose of hypothesis testing.
Tabular summaries of baseline patient characteristics were generated to describe the patient population. To protect the identity of participants, covariate strata with fewer than 5 patients have been masked by replacing the true count with “<5.” For categorical values, frequencies and percentages are reported. Continuous values are presented as median (IQR). All analyses were implemented as variable-specific complete case analyses, omitting observations with missing data when estimating descriptive statistics. Analyses of the primary outcomes entailed quantitative and qualitative approaches. Quantitatively, distributions of each of the patient and nursing staff metrics of comfort and acceptability were reported (number and percentage). Qualitative analyses were conducted to evaluate and synthesize free-text responses derived from the exit interviews of the nursing staff, which were conducted by study investigators. Major and minor themes were hierarchically identified from the interview responses through a process of familiarization, coding, and theme identification. After categorizing responses into the major and minor themes, the themes were described by providing frequencies and sample verbatim responses.
Results
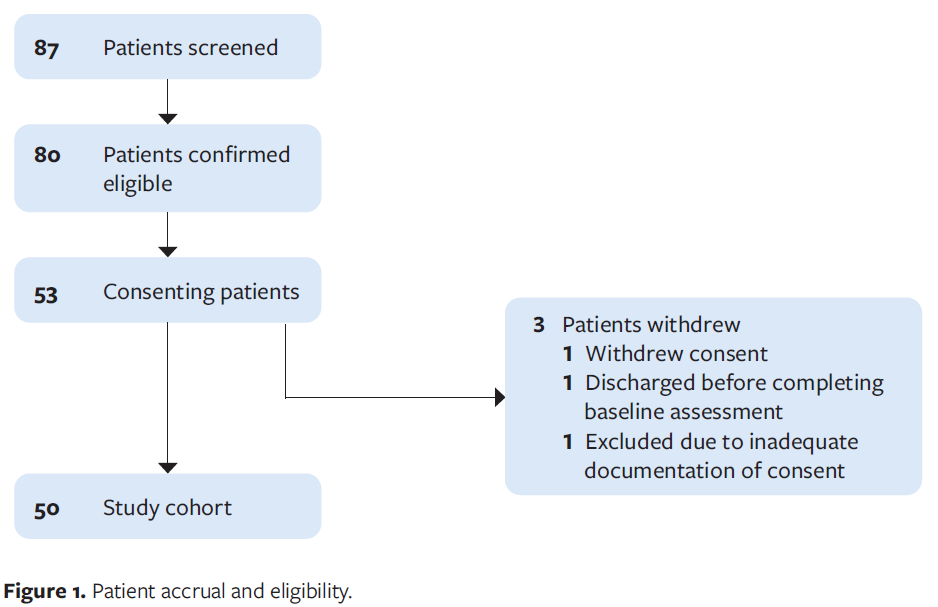
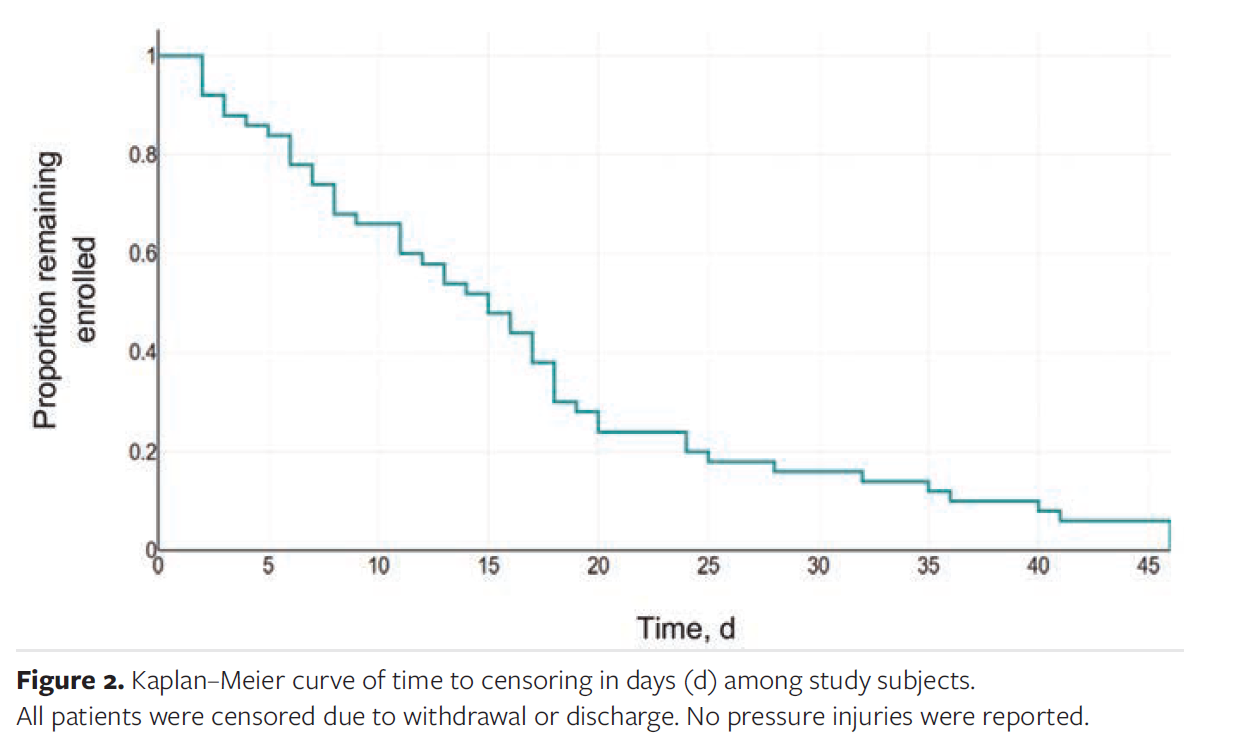
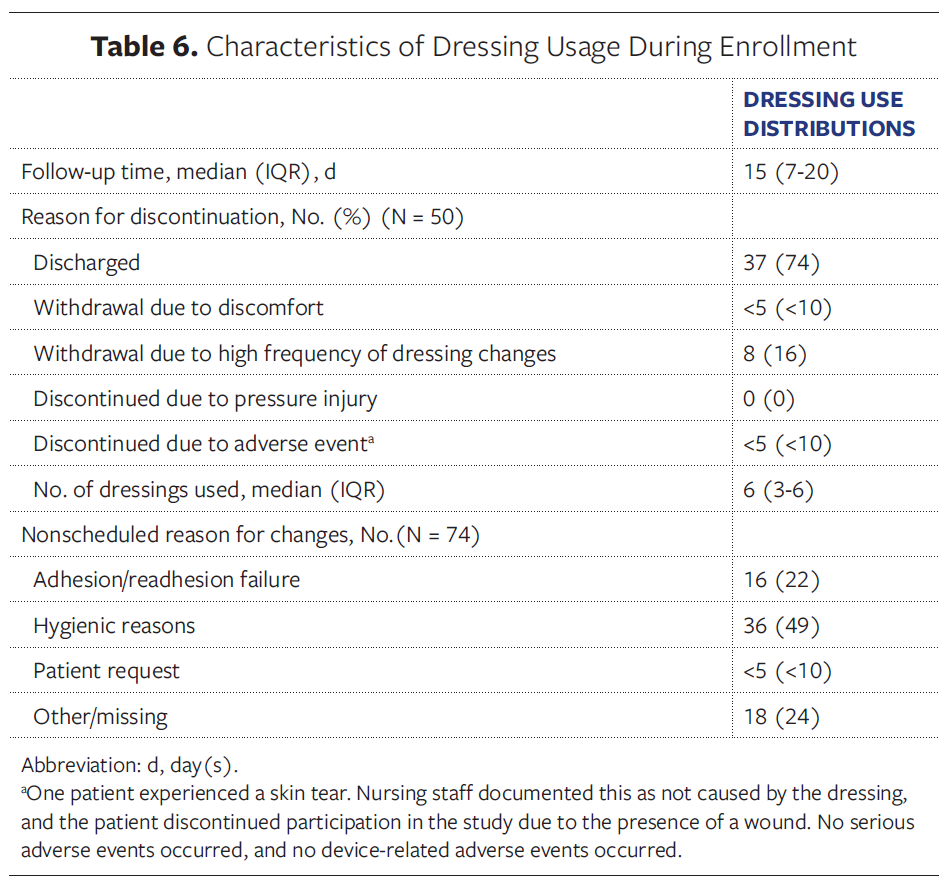
During the accrual period of the pilot clinical investigation, 87 patients were screened for eligibility, 80 patients were confirmed as eligible, and 53 patients consented to participate. Of those who consented, 1 withdrew consent, 1 was discharged prior to completing the baseline assessment, and 1 patient was excluded due to inadequate documentation of consent (Figure 1). The average follow-up time per patient was 17 days (median, 15 days), resulting in 824 patient-days of follow-up in total for this study. Figure 2 illustrates the Kaplan–Meier curve of time to censoring, showing the proportion of participants remaining enrolled over time. Censoring occurred when patients were withdrawn or discharged; no PIs were reported during the study. The most common reasons for discontinuation of the investigational dressing was discharge from hospital (74%) and withdrawal due to high frequency of dressing changes, typically due to incontinence (16%).
Of the 50 patients included in the analysis, the median age was 62 years (IQR, 43 years-68.75 years) and 90% of the subjects were white (Table 1). Consistent with expectation for the target population, consenting patients had a moderate to high risk of PI, with a median Braden Scale score of 15 (IQR, 14-17). A small number of patients had minor PIs at non-sacral sites prior to enrollment; none had a sacral PI at baseline. Common concurrent PI prevention strategies included turning/repositioning (96%), pressure-reducing mattress or specialty support surfaces (94%), diet and nutrition (82%), and pressure-reducing chair or chair cushion (76%). Topical ointments for PI prevention were less commonly observed, although still prevalent (50%). When used, topical ointments were not applied directly to the sacrum. Instead, application was limited to areas exposed to excessive moisture resulting from incontinence, such as the perineum and lower buttocks.
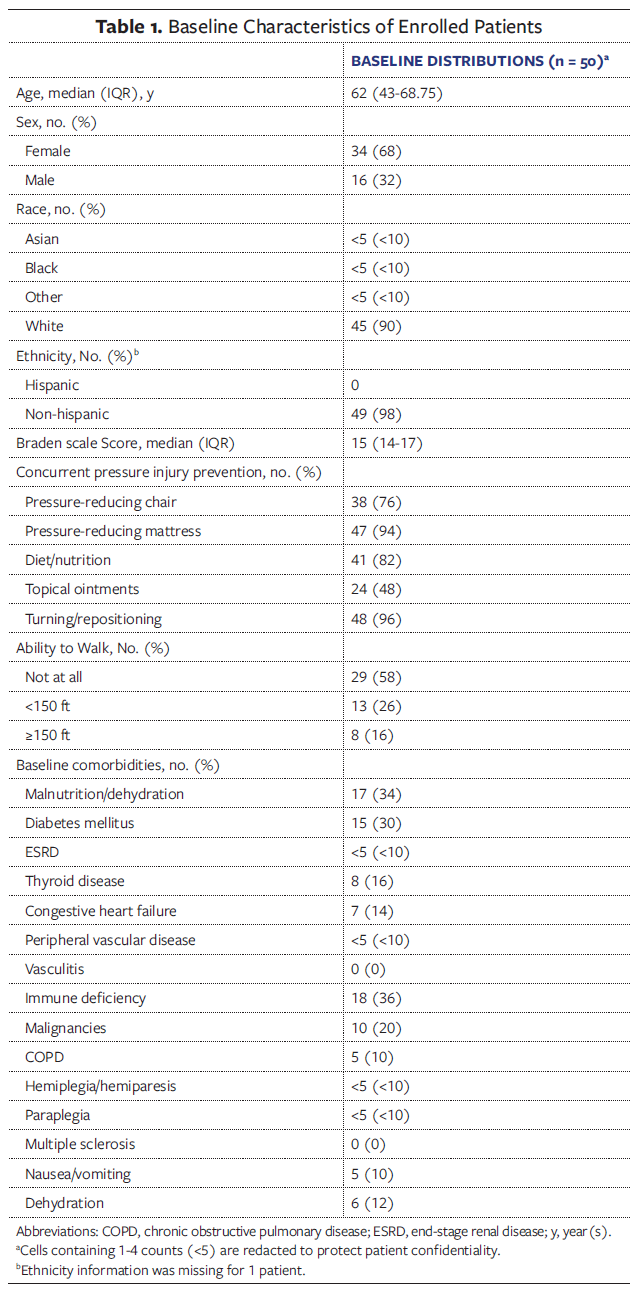
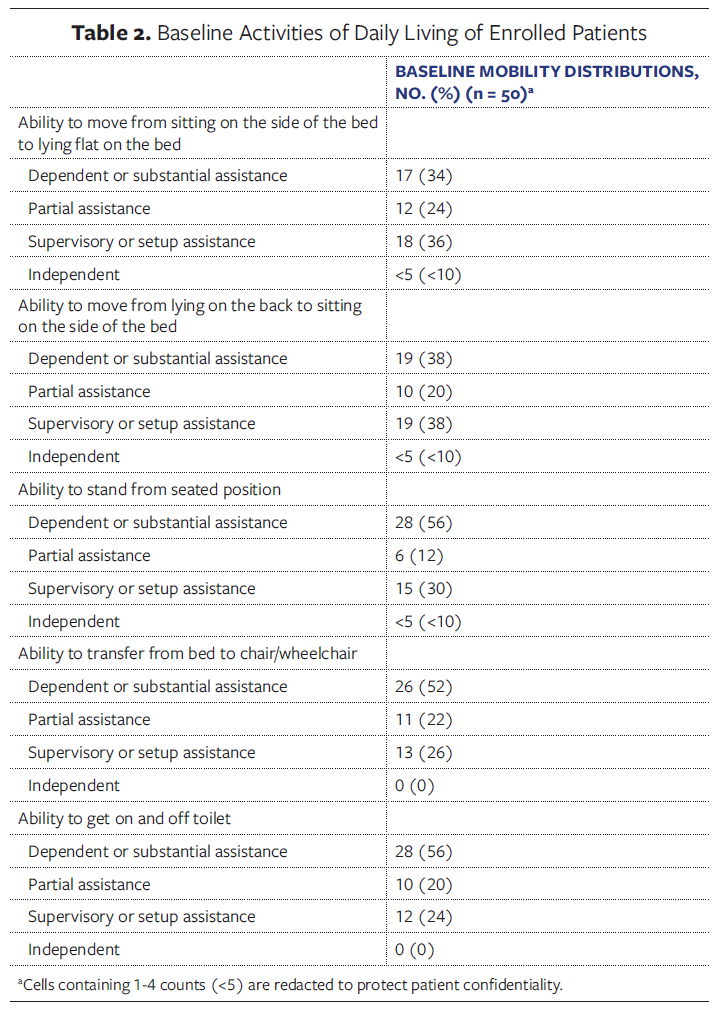
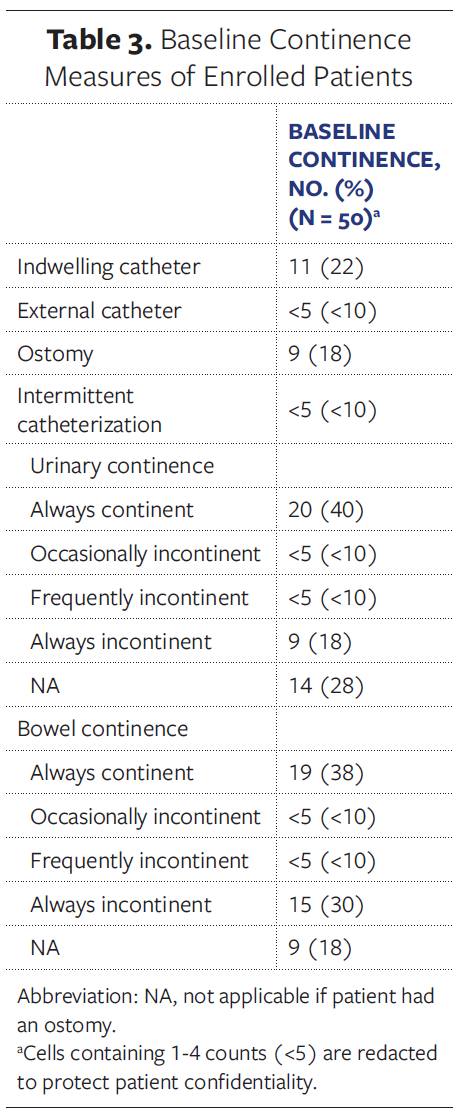
The most common baseline comorbidities included immune deficiency (36%), malnutrition or dehydration (34%), and diabetes (30%). Enrolled patients had limited mobility, with 58% of patients unable to walk. Few patients were independent in any assessed domain of baseline activity (Table 2). Over half of the study subjects were fully dependent or required substantial assistance for activities, including transitioning to standing from a seated position, transitioning to chair or wheelchair from bed, and toileting (Table 2). Distributions of baseline catheterization, ostomy, and incontinence were assessed (Table 3). Of included patients, 22% had an indwelling catheter and 18% had an ostomy. Additionally, 18% were identified as always experiencing urinary incontinence, and 30% were reported as always experiencing bowel incontinence.
Primary outcomes
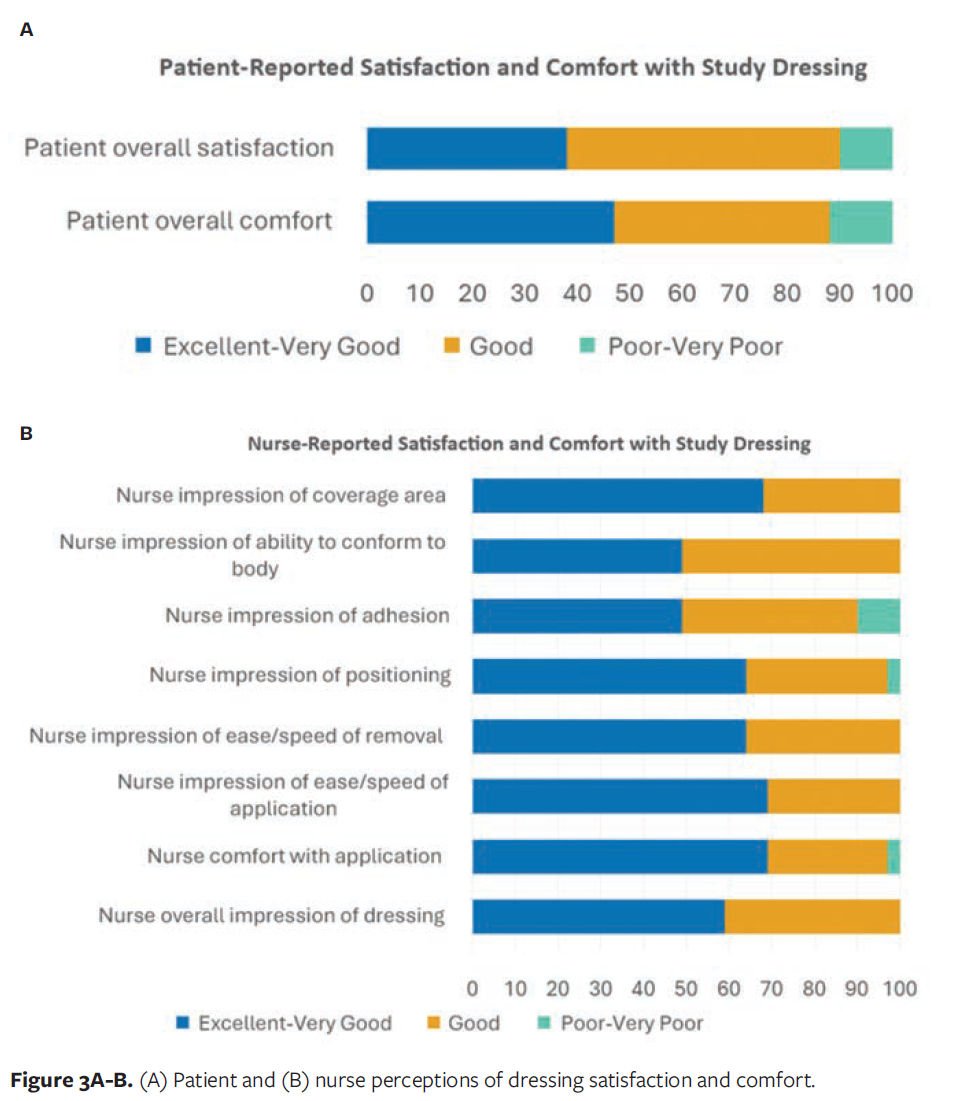
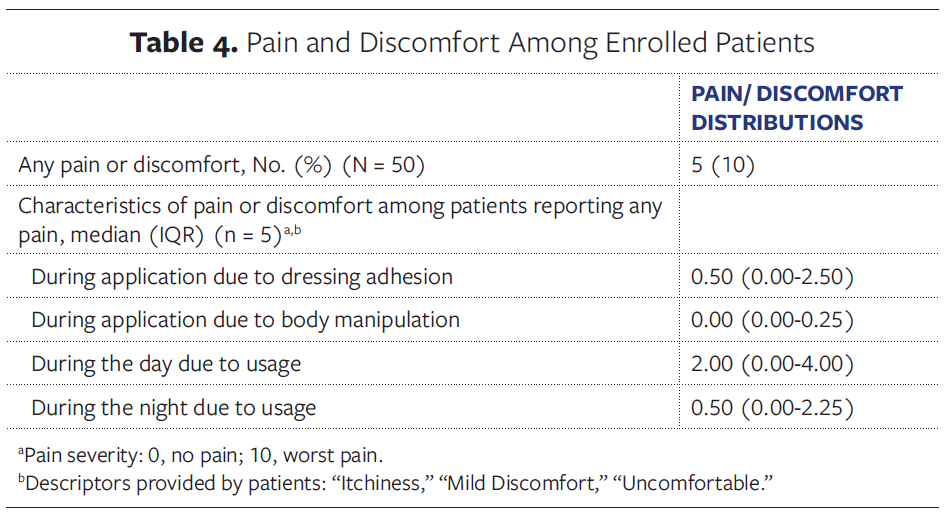
Few patients reported any pain or discomfort on the recurring surveys (10%) (Table 4). The pain score for those reporting any pain or discomfort ranged from 0 to 5 on the NRS, with a median of 0 and an average of less than 1. Due to acute or unplanned discharge occurrences and inclusion of patients who were unable to communicate, exit surveys assessing patient satisfaction were missing for 16 of the 50 study subjects. The majority of patients completing exit surveys reported good-to-excellent perceptions of overall comfort (88%) and satisfaction (91%) (Figure 3A). Nursing staff perceptions were unanimously reported as good-to-excellent for overall impression, ease and speed of application, ease and speed of removal, the dressing’s ability to conform to the patient’s body, and the dressing’s coverage of bony prominence. Other domains of nursing staff perceptions were rated highly (Figure 3B). The lowest rating was for the item on the dressing adhesion, with 89% reporting good-to-excellent perceptions.
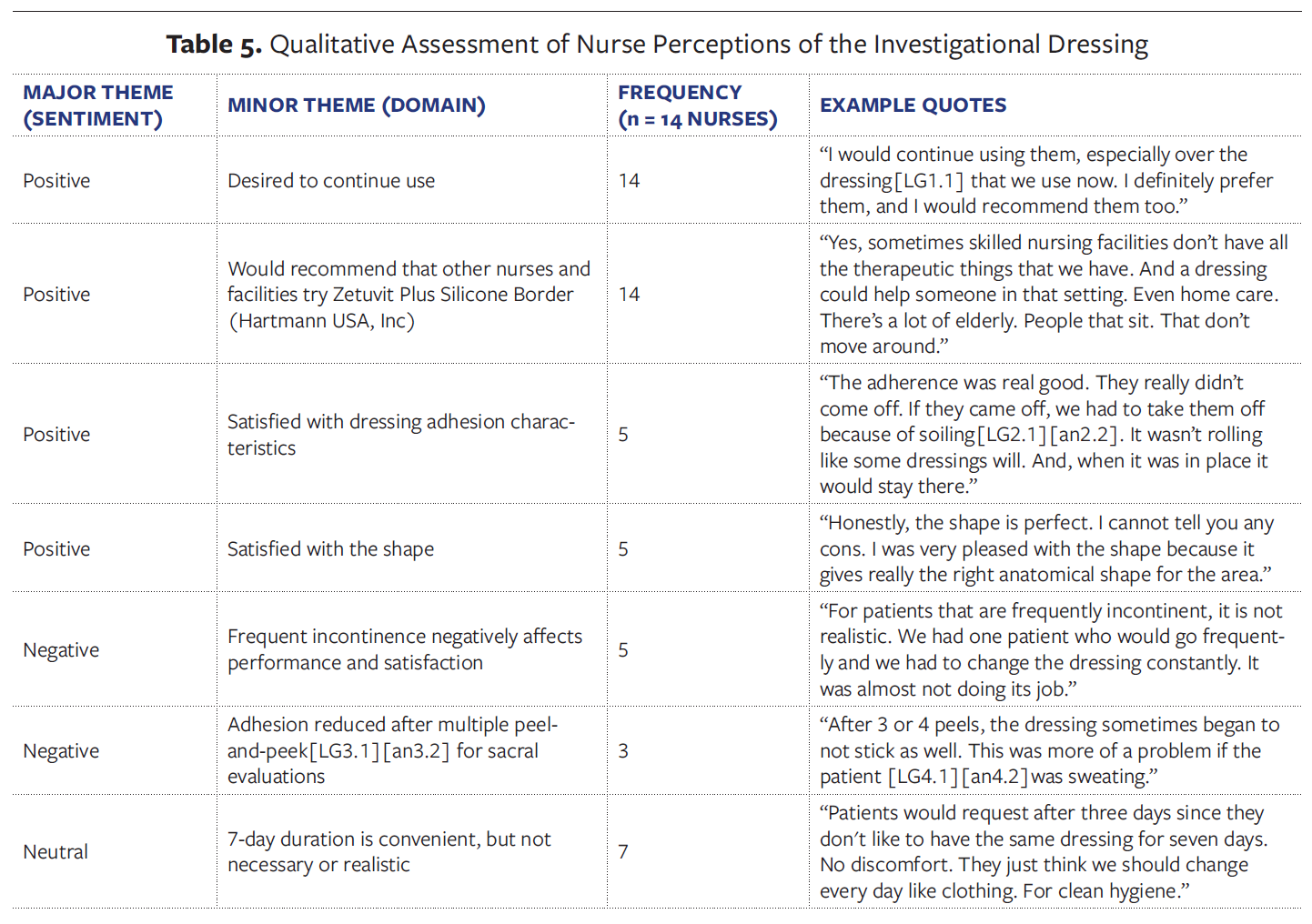
Of the nurses involved in the dressing applications, 22 were invited to participate in an interview assessing nurse perspectives of the dressings. Fourteen nurses were interviewed to gain further insights into nursing perceptions of the dressings (Table 5). Of these, 100% reported that they would continue using the investigational dressing and that they would recommend the dressing to other colleagues and facilities. Pertaining to their inclination to recommend the dressing for PI prevention, 1 nurse shared that the dressings could have broader use and may be impactful in facilities that do not have the complete set of PI prevention tools available at Spaulding Cambridge (eg, specialty support surfaces) or potentially in home care settings where patients are primarily in a seated position.
Five of the 14 nurses highlighted their satisfaction with adhesion, stating that the dressing adhered well and stayed in place until soiled. Similarly, 5 nurses had positive perceptions of the dressing’s shape, sharing that it was the correct anatomical shape. Incontinence was the most frequently noted limitation of the dressing protocol, with 5 nurses reporting that frequent incontinence limited the potential utility of the dressings. These nurses shared that frequent incontinence would be an impediment to the practicality of any dressing or topical agent intended to be applied for an extended period of time. Three of the 14 nurses noted that the removal and reapplication of dressings to inspect the sacral skin reduced adhesion over time. Lastly, 7 nurses reported that the recommended 7-day duration for a dressing was not preferable for their clinical practice and recommended a real-world duration of up to 3 days. The rationale for this recommendation included consistency with current dressings, avoidance of errors from missed skin evaluations, and patient perceptions of hygiene.
Secondary outcomes
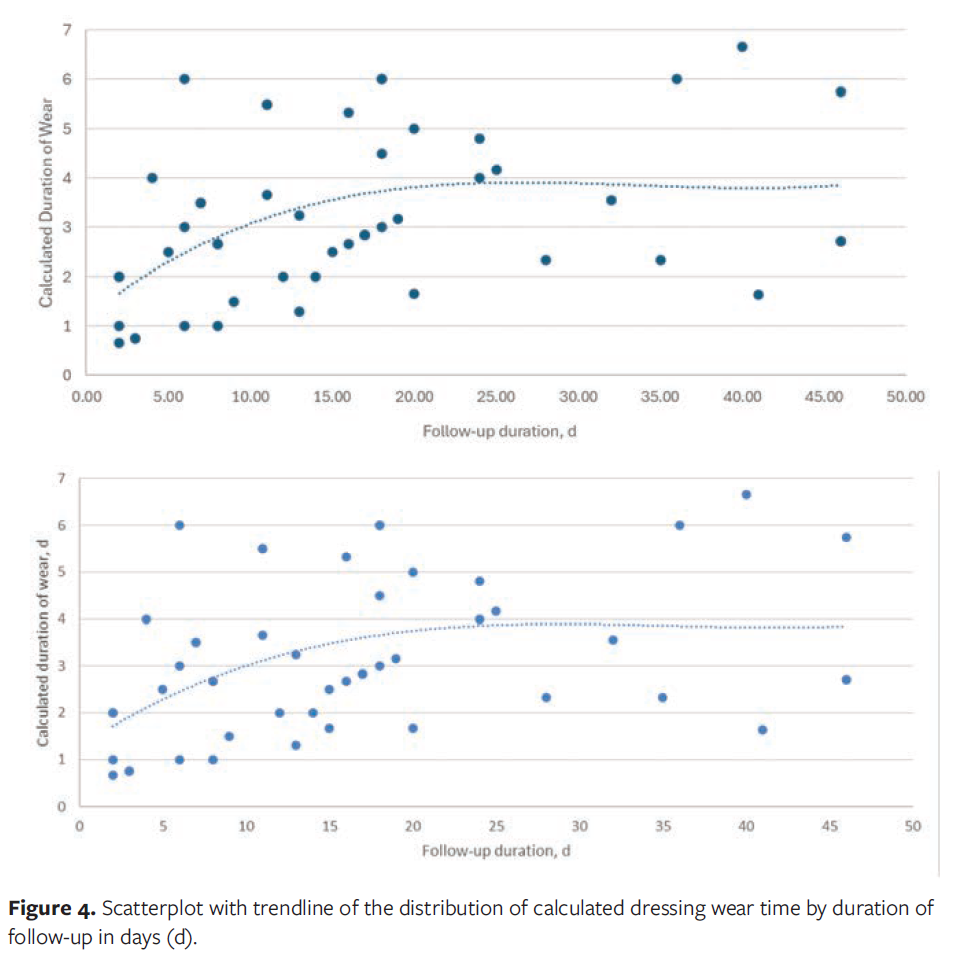
No PIs occurred during the study. No serious adverse events occurred, and no device-related adverse events occurred. One patient withdrew from the study following the occurrence of an adverse event documented as a skin tear in the sacral region, which was unrelated to the dressing. The median number of dressing changes documented for each patient was 6 (IQR, 3-6) (Table 6). The wear time per dressing ranged from less than 1 day to 7 days, with an average wear time of 2.5 days among all subjects and 3.5 days among subjects with a study enrollment of at least 7 days (calculated as duration of use divided by the reported number of dressings used). A scatterplot of calculated wear time by duration of follow-up is presented in Figure 4, showing that wear time per dressing was shorter among patients with the shortest duration of study enrollment and that it stabilized to between 3.5 days and 4 days per dressing among subjects with at least 2 weeks of study enrollment.
Discussion
The goal of this investigation was to demonstrate the feasibility of implementing a PI prevention protocol incorporating bordered silicone SAP dressings in an LTAC hospital, through assessments of nurse and patient perspectives. Although this was conducted as a pilot investigation, the findings suggest that the investigational dressing may be a safe intervention, with high ratings of patient-reported comfort and satisfaction and nurse-reported usability and satisfaction.
Few patients reported any pain or discomfort associated with the dressings. Among those reporting discomfort, the average severity of reported pain was less than 1 on the NRS. All assessed nursing staff reported a positive overall impression and a willingness to recommend the use of the dressings for PI prevention. Although the absence of PIs in this pilot study is encouraging, these findings should be interpreted with caution. The study was intentionally designed as a phase 1 feasibility and tolerability assessment. It was not designed to establish comparative effectiveness. Consequently, the small sample size, short follow-up period, and lack of a control group limit the generalizability of the results. These preliminary observations are hypothesis-generating and will inform the design of ongoing and planned comparative studies aimed at providing robust evidence on prophylactic effectiveness.
Achieving a high level of patient-reported comfort and satisfaction is noteworthy. Five of 50 patients in the present study (10%) reported any pain or discomfort, which was similar to or better than comparable assessments of foam-based dressings used in PI prevention.22 In a comparative study, discomfort during dressing removal was significantly higher with hydrocolloid dressings than with hydrocellular foam dressings.23 In that study, approximately 13% of patients receiving a foam dressing reported pain or discomfort. While discomfort is a recognized side effect during removal or with certain adhesive types, studies suggest that the benefits of PI prevention outweigh these drawbacks. Of note, among the 10% of patients reporting any pain or discomfort in the present analysis, the severity of discomfort was low, and there were high ratings of comfort and satisfaction. While formal evaluation of device safety and effectiveness requires statistical evaluation against a comparator, the lack of any observed PIs in greater than 800 combined patient-days of follow-up is encouraging. There is limited data on expected PI rates in LTAC settings. Based on data from a 10-year survey ending in 2015, the prevalence of any HAPI may be approximately 5% in LTAC hospitals.1 A study focusing on ICU settings reported PI rates of 3.40 to 6.98 per 1000 patient days in a medical intensive care unit.24 Future work is needed to evaluate the effectiveness of the investigational dressing for PI reduction.
In clinical practice, nursing staff reported patient incontinence as a significant factor affecting their experience with the dressing. Although it was demonstrated that the product may remain in place for up to 7 days (with at least daily skin inspection), this was not achieved in patients with incontinence due to soiling, bathing, or clinical decision-making. Nursing staff reported that their perceptions of more frequent dressing changes would pertain to any dressing or topical PI reduction intervention administered to patients with frequent incontinence. All nursing staff were satisfied with the dressing’s ability to cover the sacral bony prominence. Relatedly, the nursing staff perceive the anatomical shape of the dressing to be advantageous for coverage and positioning.
Limitations
This pilot study served as an initial feasibility assessment and did not include comparative analyses. To build on these findings, 3 studies have been initiated: an indirect treatment comparison using population-adjusted indirect treatment comparison, a retrospective matched cohort study vs. patients managed with PI prevention protocols without dressings, and a randomized controlled trial comparing bordered silicone SAP dressings with foam dressings. Spaulding Cambridge, a highly resourced Magnet‑accredited LTAC hospital, enabled engagement with well‑trained nursing staff; however, nursing and patient experiences at this site may not reflect those at other LTAC hospitals. Satisfaction was assessed using study‑specific, non‑validated questionnaires (Cronbach alpha: 0.97 for patient questions and 0.92 for nursing questions). Although high internal consistency suggests related constructs, nurses and patients may have under‑ or overestimated their satisfaction during an ongoing study, which may introduce response bias.
The study relied on assessments administered by nursing staff at baseline, at each dressing change, and on the patient’s exit from the study. All patients had complete baseline assessments. For assessments at dressing changes, nursing staff were asked to complete recurring patient forms each time a dressing was removed and replaced. Often, nursing staff were unable to submit a recurring assessment at each dressing change, resulting in 106 submissions out of 247 dressing change opportunities. The site principal investigator (J.G.) reported that missingness resulted from clinical burden experienced by all nursing staff. The recurring assessments were relied upon for measures of patient pain or discomfort and dressing issues (ie, changes earlier than anticipated or dressing failures). For these measures, the study authors expect that nursing staff were more likely to submit forms when patients reported discomfort or when the dressing did not perform as expected. This may result in an overestimate of the magnitude of pain and discomfort. Similarly, the present study may overestimate the occurrence of dressing changes that were earlier than anticipated. In addition to a potential sampling bias resulting from missing data, it is important to note that some nursing staff interpreted anything less than 7 days to be earlier than anticipated. Of the 74 reports of early dressing changes, 25 occurred 3 days or more from the previous dressing change. Exit surveys were available for 34 of the 50 patients, with the primary reason for missingness being acute and unplanned discharge. Exit surveys were available for all patients who withdrew from the study prior to discharge. Given that the study authors have complete assessments for patients opting to withdraw, the authors expect that the analyses underestimate patient satisfaction. Complete data were available for occurrence of PIs and adverse events.
Studies within LTAC hospitals are difficult to implement due to facility closures as a result of reduced hospital-level reimbursement rates25 and staffing shortages, which affected study site recruitment efforts. Although the selected site for the present study was an LTAC hospital, factors related to patient complexity and nurse turnover were barriers to patient recruitment. In addition, during the study conduct, the authors’ hospital redesignated some LTAC beds as rehabilitation beds, thus reducing the number of available beds designated as LTAC.
Conclusions
The attributes and evidence for bordered silicone SAP dressings suggest promise for acceptable integration into existing PI prevention protocols. This pilot study demonstrates that bordered silicone SAP dressings can be applied in the medically complex patient population encountered in the LTAC setting, with high patient and nurse satisfaction. Future analysis will evaluate whether a comparative reduction in PI can be achieved.
Author and Public Information
Authors: Jennifer Godfrey, MSN, RN, CWCN, COCN, CCCN1; Chrystalbelle Rogers, MSN, RN, CWCN, CENP2; Syed Naqvi, PhD3; Emily Goddu, MSN, FNP-BC, CWCN, COCN1; and Anthony P. Nunes, PhD3
Affiliations: 1Spaulding Hospital for Continuing Medical Care, Cambridge, MA; 2Hartmann Group, Rock Hill, SC; 3UMass Chan Medical School, Worcester, MA
Corresponding Author: Chrystalbelle Rogers, MSN, RN, CWCN, CENP; Hartmann USA, Inc, 481 Lakeshore Pkwy, Rock Hill, SC 29730; chrystalbelle.rogers@hartmann.info
Acknowledgments: We acknowledge the contributions of the nursing staff of Spaulding Rehabilitation Hospital for their facilitation of study implementation, with specific acknowledgment of the nurse investigators, including Erika Dilbarian, RN, CWON, Nicole Pantos, RN, CWON, Olivia Domack, RN, CWOCN, and Savannah Fair, RN. We are grateful for the contributions of Erin Buchness, MHL, RN, CWCN, CHWS, who assisted in the coordination of training and distribution of dressings.
Disclosures: C.R. is an employee of Hartmann USA, Inc, the manufacturer of investigational dressing. A.P.N. and S.N. were employed by UMass Chan Medical School, a recipient of research funds from Hartmann Group in support of this study. J.G. and E.G. are employed by Spaulding Hospital for Continuing Medical Care, a recipient of research funds from Hartmann Group in support of this study.
Author Contributions: All authors contributed to the design and planning of the study and to the review and revision of the manuscript. J.G. acted as the study site principal investigator and was responsible for overseeing data collection and on-site study operation. A.N. was responsible for data analysis and drafting of the manuscript.
Ethical Approval: This study was reviewed and approved by the Mass General Brigham Institutional Review Board. All patients included in this study consented directly, or via legal proxy if needed, and capacity to consent was verified.
Funding: This study was sponsored by Hartmann Group, the manufacturer of the investigational device.
Manuscript Accepted: March 4, 2026
Recommended Citation
Godfrey J, Rogers C, Naqvi S, Goggu E, Nunes AP. Patient and nurse perceptions of a bordered silicone superabsorbent polymer dressing for pressure injury prevention: a prospective noncomparative pilot study in a long-term acute care hospital. Wounds. 2026;38(5):127-136. doi:10.25270/wnds/25124
References
- VanGilder C, Lachenbruch C, Algrim-Boyle C, Meyer S. The International Pressure Ulcer PrevalenceTM Survey: 2006-2015: a 10-year pressure injury prevalence and demographic trend analysis by care setting. J Wound Ostomy Continence Nurs. 2017;44(1):20-28. doi:10.1097/WON.0000000000000292
- Rondinelli J, Zuniga S, Kipnis P, Kawar LN, Liu V, Escobar GJ. Hospital-Acquired Pressure Injury: Risk-Adjusted Comparisons in an Integrated Healthcare Delivery System. Nurs Res. 2018;67(1):16-25. doi:10.1097/NNR.0000000000000258
- Pittman J, Beeson T, Dillon J, Yang Z, Cuddigan J. Hospital-acquired pressure injuries in critical and progressive care: avoidable versus unavoidable. Am J Crit Care. 2019;28(5):338-350. doi:10.4037/ajcc2019264
- Gefen A, Brienza DM, Cuddigan J, Haesler E, Kottner J. Our contemporary understanding of the aetiology of pressure ulcers/pressure injuries. Int Wound J. 2022;19(3):692-704. doi:10.1111/iwj.13667
- Wound, Ostomy and Continence Nurses Society-Wound Guidelines Task Force. WOCN 2016 guideline for prevention and management of pressure injuries (ulcers): an executive summary. J Wound Ostomy Continence Nurs. 2017;44(3):241-246. doi:10.1097/WON.0000000000000321
- Kottner J, Cuddigan J, Carville K, et al. Prevention and treatment of pressure ulcers/injuries: the protocol for the second update of the international Clinical Practice Guideline 2019. J Tissue Viability. 2019;28(2):51-58. doi:10.1016/j.jtv.2019.01.001
- Qaseem A, Mir TP, Starkey M, Denberg TD; Clinical Guidelines Committee of the American College of Physicians. Risk assessment and prevention of pressure ulcers: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2015;162(5):359-369. doi:10.7326/M14-1567
- Post-Acute and Long-Term Care Medical Association (PALTmed). Pressure Ulcers and Other Wounds in the Post-Acute and Long-Term Care Setting Clinical Practice Guideline. PALTmed; 2017.
- Serafin A, Graziadio S, Velickovic V, et al. A systematic review of clinical practice guidelines and other best practice recommendations for pressure injury risk assessment in the United States. Wound Repair Regen. 2025;33(2):e70016. doi:10.1111/wrr.70016
- 2025 NPIAP Prevention and Treatment of Pressure Ulcers/Injuries - Guideline Summary - Guideline Central. Accessed October 23, 2025. https://www.guidelinecentral.com/guideline/23835.
- Kandula UR. Impact of multifaceted interventions on pressure injury prevention: a systematic review. BMC Nurs. 2025;24(1):11. doi:10.1186/s12912-024-02558-9
- Patton D, Moore ZE, Boland F, et al. Dressings and topical agents for preventing pressure ulcers. Cochrane Database Syst Rev. 2024;12(12):CD009362. doi:10.1002/14651858.CD009362.pub4
- Ramundo J, Pike C, Pittman J. Do prophylactic foam dressings reduce heel pressure injuries? J Wound Ostomy Continence Nurs. 2018;45(1):75-82. doi:10.1097/WON.0000000000000400
- Sugrue C, Avsar P, Moore Z, et al. The effect of prophylactic silicone dressings on the incidence of pressure injuries on patients in the acute care setting: a systematic review and meta-analysis. J Wound Ostomy Continence Nurs. 2023;50(2):115-123. doi:10.1097/WON.0000000000000953
- Fu T, Wu X, Yu B. Efficacy of silicone foam dressings in preventing pressure injuries in the sacral and heel areas of patients: a meta-analysis. Front Med (Lausanne). 2025;12:1644290. doi:10.3389/fmed.2025.1644290
- Tayyib N, Coyer F. Effectiveness of pressure ulcer prevention strategies for adult patients in intensive care units: a systematic review. Worldviews Evid Based Nurs. 2016;13(6):432-444. doi:10.1111/wvn.12177
- Gefen A, Krämer M, Brehm M, Burckardt S. The biomechanical efficacy of a dressing with a soft cellulose fluff core in prophylactic use. Int Wound J. 2020;17(6):1968-1985. doi:10.1111/iwj.13489
- Beele H, Van Overschelde P, Olivecrona C, Smet S. A prospective randomized controlled clinical investigation comparing two post-operative wound dressings used after elective hip and knee replacement: Mepilex® Border Post-Op versus Aquacel® surgical. Int J Orthop Trauma Nurs. 2020;38:100772. doi:10.1016/j.ijotn.2020.100772
- Pickles S, McAllister E, McCullagh G, Nieroba TJ. Quality improvement evaluation of postoperative wound dressings in orthopaedic patients. Int J Orthop Trauma Nurs. 2022;45:100922. doi:10.1016/j.ijotn.2022.100922
- Anusitviwat C, Yuenyongviwat V. Comparing silicone-coated self-adhesive absorbent polyurethane films with transparent absorbent films for bilateral hip dressing: a prospective randomized controlled trial. J Orthop Surg Res. 2025;20(1):129. doi:10.1186/s13018-024-05448-7
- Thong ISK, Jensen MP, Miró J, Tan G. The validity of pain intensity measures: what do the NRS, VAS, VRS, and FPS-R measure? Scand J Pain. 2018;18(1):99-107. doi:10.1515/sjpain-2018-0012
- White R. A multinational survey of the assessment of pain when removing dressings. Wounds UK. 2008;4(1):14-22.
- da Silva Augusto F, Blanes L, Ping PZX, Saito CMM, Masako Ferreira L. Hydrocellular foam versus hydrocolloid plate in the prevention of pressure injuries. Wounds. 2019;31(8):193-199.
- Byrne J, Nichols P, Sroczynski M, et al. Prophylactic sacral dressing for pressure ulcer prevention in high-risk patients. Am J Crit Care. 2016;25(3):228-234. doi:10.4037/ajcc2016979
- Law AC, Bosch NA, Song Y, et al. Patient outcomes after long-term acute care hospital closures. JAMA Netw Open. 2023;6(11):e2344377. doi:10.1001/jamanetworkopen.2023.44377








