



Retrospective Evaluation of the Clinical Effectiveness of an Innovative Catalytic Wound Care Technology
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background. Chronic, nonhealing wounds have significant negative effects on both patients and the health system, including increased morbidity and mortality. Objective. To retrospectively examine the effect of an advanced wound care treatment that delivers catalytic technology to the affected area through polymers that mimic the extracellular matrix. Materials and Methods. The proprietary catalytic treatment matrix (CTM) technology facilitates copper-dependent cellular signaling pathways within the wound healing process. Patients whose wounds were originally treated following standard wound care protocols and then subsequently transitioned to the catalytic technology (as determined by their physician), were recruited from a specialized outpatient wound care clinic in Calgary, Alberta, Canada. Data were collected from charts for 19 patients with a total of 26 chronic wounds (venous leg ulcers and diabetic foot ulcers). Following initiation of the catalytic technology, time to wound closure was tracked via percent area reduction, or for up to 16 weeks if wounds did not close. Results. The average age of the wounds prior to application of the CTM technology was 39 weeks. After transitioning to CTM technology, 81% of wounds closed within 16 weeks. Notably, 77% of the wounds closed within the first 8 weeks (±2 days) of initiating use. Overall, the average time to closure was 43 days (median, 35 days). Conclusion. CTM technology was shown to be an effective tool for improving time to closure of chronic wounds.
Chronic wounds are defined as wounds that do not heal in a predictable or timely manner despite appropriate care.1,2 Current practices for the treatment of chronic wounds are unique to the individual and the wound. Wound management practices focus on resolving the root causes and may take a multipronged approach. As part of treatment, wounds may be dressed with a variety of products. Dressings are chosen based on the unique needs of each wound and are typically focused on moisture management and infection control. Advanced therapies are also available that are implemented to either augment or replace traditional approaches to wound management; however, these are often costly therapies that have limited availability in many jurisdictions.
Despite comprehensive standard of care protocols, chronic wounds continue to present a significant challenge to health systems from both a clinical and economic perspective. In Canada, an estimated $13 billion was spent on managing wounds in 2024, which had increased from previous estimates.3 The persistent burden of chronic wounds creates the need for innovative strategies that go beyond the existing modalities and provide a simple approach to optimize healing at each phase of wound care.
A Calgary-based specialized outpatient wound clinic began using NanoSALV Catalytic Advanced Wound Care Treatment Matrix (NanoTess Inc; hereafter “CTM technology”) as a potential innovative solution to support the treatment and management of chronic wounds. This technology is authorized by Health Canada as a Class II medical device.4 It is indicated for use in a variety of wounds, including chronic wounds, acute wounds, burns, and dermatological conditions.5 The gel delivers proprietary Catalytic Treatment Matrix (CTM) technology to the affected area through polymers that mimic the extracellular matrix. The CTM technology is composed of copper, titanium dioxide, and silica structures. In a wound environment, the CTM technology facilitates the numerous copper-dependent cellular signaling pathways within the wound healing process. Copper is well known to be an essential element that plays a role in all major stages of wound healing (hemostasis, inflammation, proliferation, and remodelling), for example,6
- Vascularization support: Copper modulates the expression of vascular endothelial growth factor.
- Extracellular matrix stabilization: Copper is a necessary cofactor for the enzyme lysyl oxidase, which is essential for the cross-linking of collagen and elastin, strengthening the newly formed tissue.
- Fibroblast function and collagen synthesis: Copper promotes the secretion of collagen (types I, II, and V), elastin, and fibrillin by fibroblasts.
- Reepithelialization: Copper stimulates the migration and proliferation of keratinocytes, helping to close the wound.
- Inflammatory response: Copper acts as a cofactor for superoxide dismutase, an enzyme that protects against free radicals and oxidative stress, which can otherwise damage tissues. It also modulates macrophage activity.
- Antimicrobial protection: Copper provides a broad-spectrum antimicrobial effect across a wide range of pathogens, including gram-positive and gram-negative bacteria, fungi, yeast, viruses, resistant strains, and biofilms, helping to prevent or treat infection, which is often the cause of stalled healing.
Despite these known benefits of copper in wound healing, silver-based materials remain more widely used for antimicrobial applications in wound dressings.7 To better understand the potential effect of CTM technology, the authors of the current study retrospectively evaluated data collected from an outpatient clinic to determine the impact of the CTM technology on wound progression compared with current state dressings and whether use of the CTM technology results in a faster time to wound closure compared with current state dressings.
Materials and Methods
Data Collection
The project team received a waiver of consent as part of a research protocol that was reviewed and approved by the Conjoint Health Research Ethics Board to access chart and wound imaging data at an outpatient clinic that specializes in foot care and ulcer treatment in Calgary, Alberta, Canada. The CTM technology was integrated as a new treatment to be used as part of daily practice for chronic wounds at the clinic.
All patients either had caregiver support or were able to independently perform dressing changes using the CTM technology at home, at a frequency prescribed by the physician. The frequency of application for the technology varied depending on the standard of care for each wound and ranged from every 24 hours to every 72 hours.
Standard patient appointments occurred weekly. During clinic visits, nursing staff performed the dressing changes following image capture. Plain secondary dressings, not containing antimicrobial properties, were placed over the top of the CTM technology and were used to manage wound exudate. The most common secondary dressing types were soft silicone foam dressings and hydrofiber dressings. All other patient factors remained consistent prior to the integration of the CTM technology, including off-loading, nutrition, diabetes management, and compression, as applicable.
Time to closure tracked through percent area reduction was used as an indicator for wound healing. Time to closure is recognized by the US Food and Drug Administration as a clinically relevant end point in wound healing clinical trials.8–10 This metric offers a standardized, objective way to assess healing progress across wounds of various sizes. It is especially useful in retrospective studies in which limited time-point data are available. Wound closure, defined as a percent area reduction of 100, was clinically confirmed by the physician during the patient’s clinic visit and recorded in their chart.
Wound images were collected during each patient clinic visit using the SilhouetteStar wound imaging camera (Aranz Medical Ltd).11 Because the original wound image tracings were collected by clinic staff and not completed by the research team, all images were reviewed by study team members. Retracings were completed if deemed appropriate. To address possible variability between team members, a random sampling of wound images was selected by the study team for review by the study lead (CH).
 Inclusion Criteria
Inclusion Criteria
Data were collected from charts for patients aged 18 years or older who had received the CTM technology as part of their wound care, as prescribed by the overseeing physician, between September 2, 2022, and February 7, 2023.
Wounds were included if they did not progress with use of standard of care practices. As a minimum requirement, the wounds needed to be present for at least 14 days using standard of care treatment before being transitioned to treatment with the CTM technology per physician discretion. Given the nature of the wounds seen at the clinic, both diabetic foot ulcers and venous leg ulcers were included. For diabetic foot ulcers, patients were required to have a diagnosis of diabetes mellitus type 1 or 2, with ulcer area post-debridement between 1 cm2 and 25 cm2. Venous leg ulcers were included if the ulcer area post-debridement measured between 2 cm2 and 50 cm2. All eligible wounds treated with the CTM technology at the clinic were included in the study.
Infections identified in the historical chart review were treated with antibiotics when clinically indicated.
Statistical Analysis
Descriptive statistical methods were used to summarize the data. These include the number of subjects, mean, and standard deviation for continuous variable data (medians and IQR values are given when the distribution of variable value is nonnormal), and frequencies and percentages for categorical data. Unless otherwise specified, all statistical testing was 2-sided and performed using a significance (alpha) level of .05.
The percent area reduction from baseline was calculated as the percent change in the surface area of the index wound using the formula ([A1−A2]/A1)*100, where A1 is the baseline area and A2 is the area at the specified time point.
All statistical analyses were conducted using SPSS (version 28.0; IBM) and NCSS 12 (NCSS LLC).
Results
Demographics
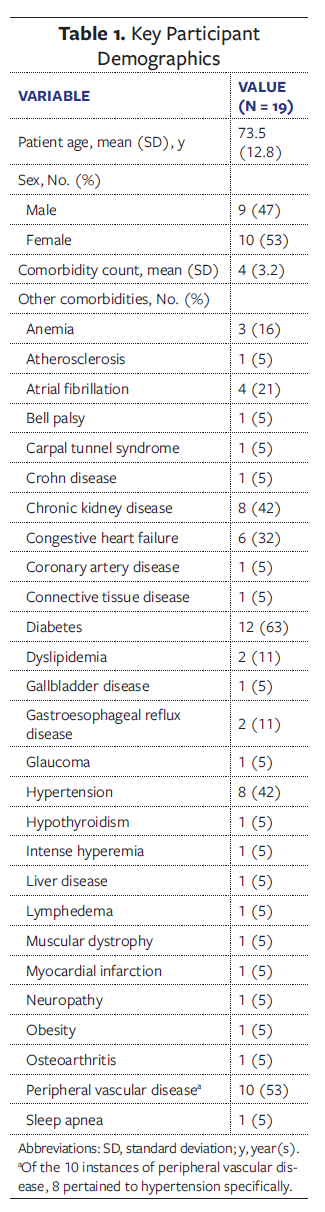
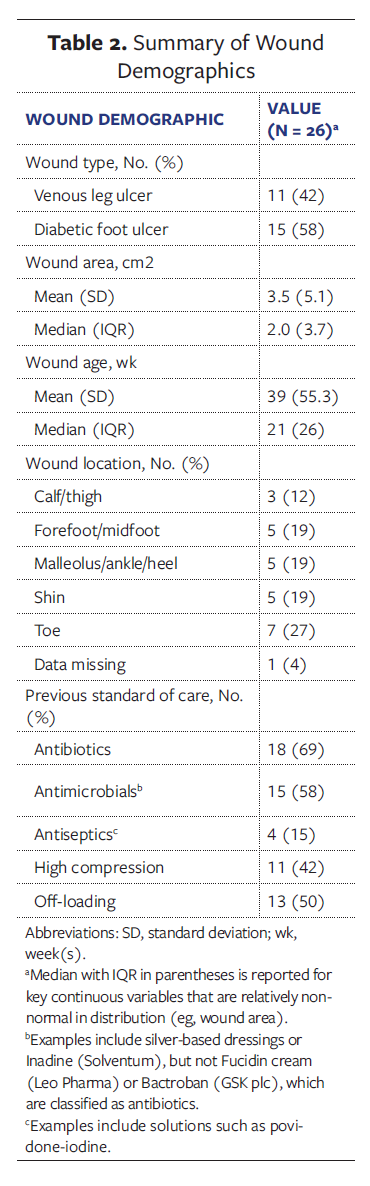 Table 1 provides an overview of the study population. Ten of the 19 patients were female (53%) and 9 were male (47%), and the overall population had an average of 4 comorbidities. The most common comorbidities were diabetes (63%); peripheral vascular disease (53%), with 8 of those 10 instances pertaining to hypertension specifically; and chronic kidney disease (42%). The average time of treatment with the standard of care prior to application of the CTM technology was 39 weeks.
Table 1 provides an overview of the study population. Ten of the 19 patients were female (53%) and 9 were male (47%), and the overall population had an average of 4 comorbidities. The most common comorbidities were diabetes (63%); peripheral vascular disease (53%), with 8 of those 10 instances pertaining to hypertension specifically; and chronic kidney disease (42%). The average time of treatment with the standard of care prior to application of the CTM technology was 39 weeks.
For any patient with more than 1 wound that met inclusion criteria, each wound was classified accordingly and included in the data analysis. Overall, data from 19 patients with 26 chronic wounds were included in the analysis. Table 2 provides an overview of the wounds, including wound age, size, and location, and previous standard of care approaches. All diabetic foot ulcers were Wagner grade 2.
Outcomes
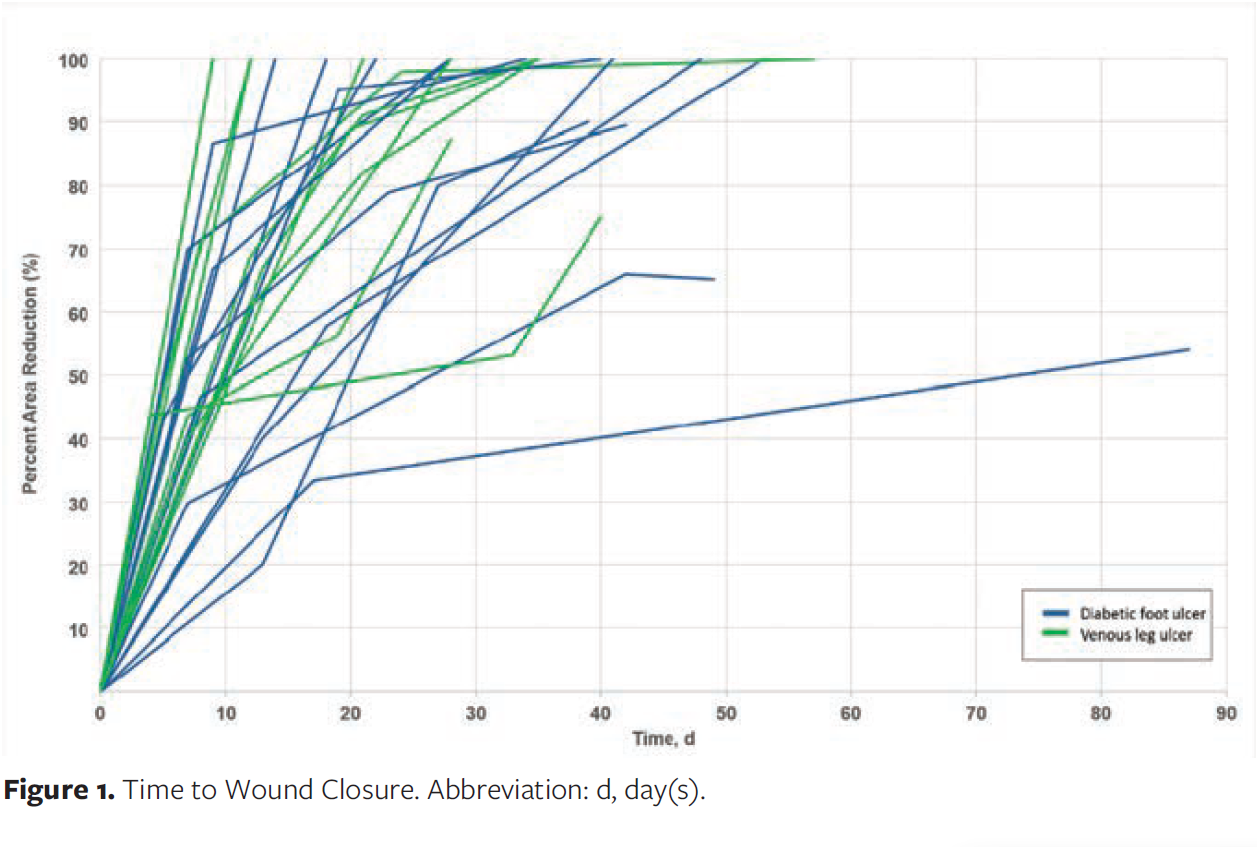
As shown in Figure 1, 81% of the wounds (21 of 26) healed within 16 weeks. Notably, 77% of the wounds (20 of 26) healed within the first 8 weeks (±2 days). At 16 weeks, healing was achieved in 82% of the venous leg ulcers (9 of 11) and in 80% of the diabetic foot ulcers (12 of 15). The average time to heal with the CTM technology was 43 days (95% CI, 30.6-54.9), with a median of 35 days (95% CI, 26.8-43.2). Notably, healing rates were similar for both venous leg ulcers and diabetic foot ulcers, potentially indicating that the CTM technology has a benefit regardless of wound type.
For the 5 wounds that did not heal within 16 weeks, all had decreased in overall area by that time point, with a mean percent area reduction of 74% with CTM technology treatment. These wounds were quite old (between 1 year and 3.2 years), and 1 was notably large (25.8 cm2).
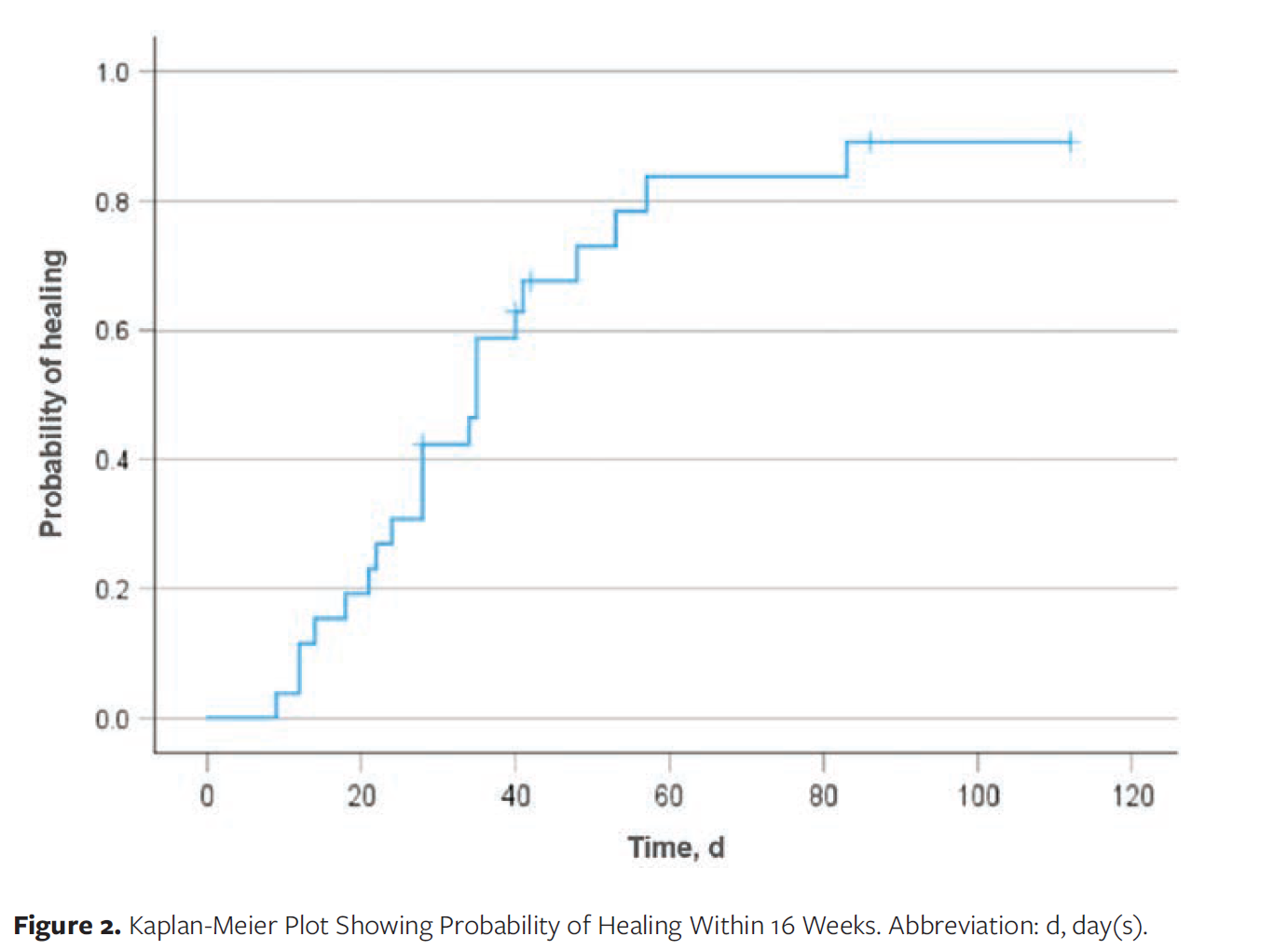
Figure 2 displays a Kaplan-Meier plot, which typically is used to demonstrate time-to-event data when not all subjects continue in a study.12 In the present study, however, the plot is used to demonstrate the probability for a wound to heal to closure while on the CTM technology at various time points up to 16 weeks. Consistent with the findings from Figure 1, at 16 weeks on the CTM technology, the probability of chronic wound healing was approximately 90%.
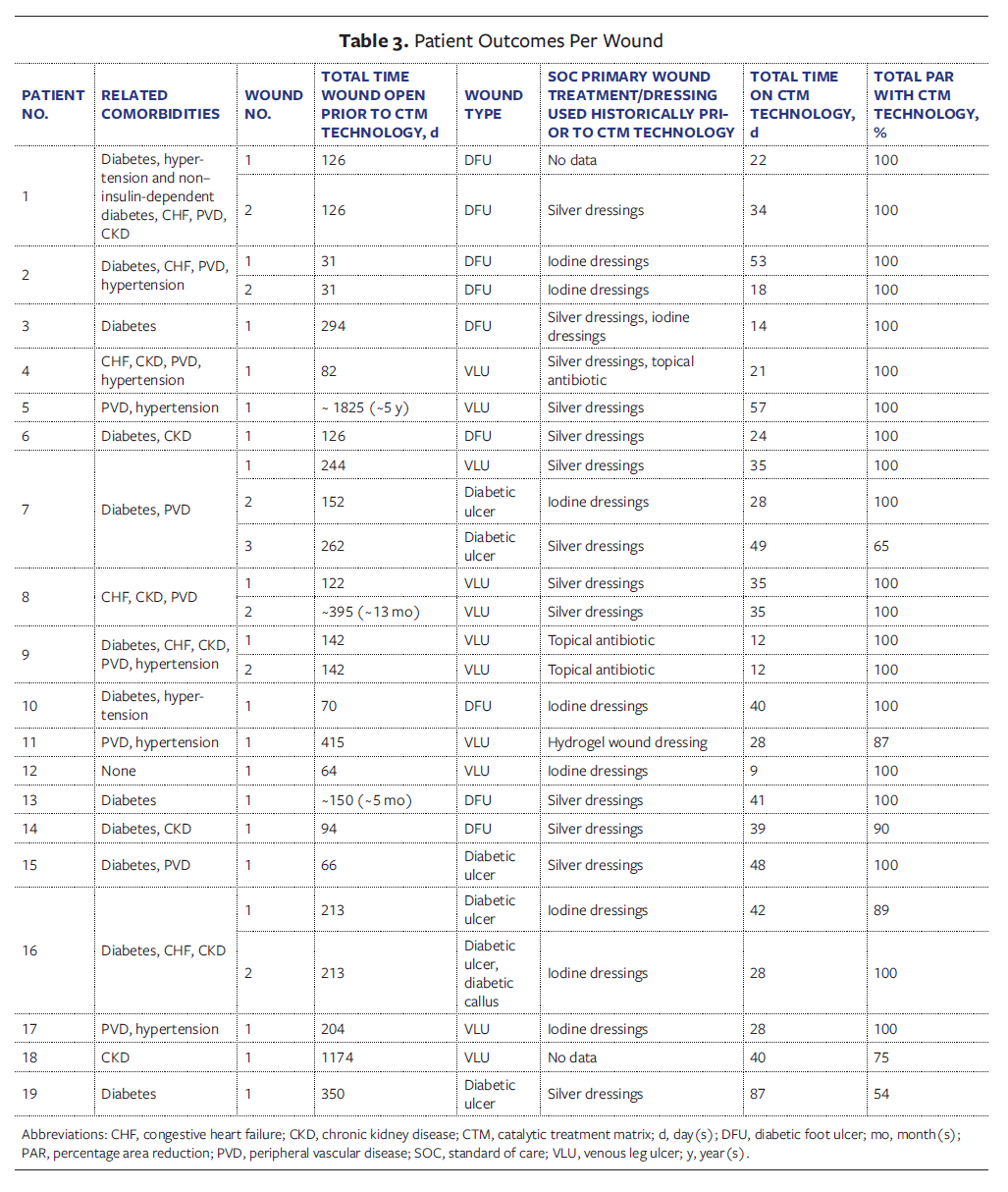
A detailed account of patient outcomes per wound is shown in Table 3.
Discussion
This retrospective study demonstrates promising clinical outcomes for the CTM technology in treating chronic wounds, with an 81% healing rate within 16 weeks and a median time to closure of 35 days. From an exploratory perspective, these results compare favorably with typical standard of care healing rates of 40% to 50% over the same time frame,13 suggesting clinical benefit of the CTM technology in real-world practice settings. However, it is important to note that in the present study no direct statistical comparison with standard care or a control group was performed.
The healing rates regardless of wound type across both venous leg ulcers (82% healing rate) and diabetic foot ulcers (80% healing rate) in the present study are particularly noteworthy, because these represent distinct pathophysiological processes with traditionally different healing trajectories.14,15 These results in combination with the copper mechanism of action of the CTM technology suggest that this treatment may address the fundamental biochemical mechanisms underlying stalled wound healing that go beyond specific wound types.
The patient population studied in the current report reflects the complexity of real-world chronic wound management, with participants presenting multiple comorbidities, including diabetes, peripheral vascular disease, and chronic kidney disease. Despite these challenging baseline characteristics that typically impede wound healing,16 in the present study the observed outcomes remained strong, suggesting that the CTM technology’s effectiveness may extend to the medically complex patients commonly encountered in clinical practice.
Notably, even among the 5 wounds that did not achieve complete closure within 16 weeks, the high percent area reduction demonstrates meaningful clinical progress. Given that these wounds were notably chronic (1 year to 3.2 years’ duration) and in 1 case the wound was exceptionally large (25.8 cm²), the CTM technology represents a promising opportunity for the management of wounds that have not responded to current state approaches.
Limitations
As a retrospective study, this study relied on existing data, which can be incomplete or inaccurate due to missing records or inconsistent recording methods.17 This limitation was mitigated as much as possible through cross-checking wound tracings and obtaining data from valid sources (ie, patient charts). Overall, the quality and availability of data can limit the generalizability of the findings. To help address the limitations of the retrospective data used in the current study, a prospective study has also been conducted.18
Conclusion
Preliminary findings indicate that when compared with current state advanced dressings used in combination with standard of care practices (eg, nutrition, compression, off-loading), the CTM technology facilitated healing, leading to full wound closure in cases in which healing had previously stalled. These results highlight the CTM technology as a promising innovation for addressing chronic wound care challenges, including in complex populations.
Author and Public Information
Authors: Anna Bradford, MBT1; Jill de Grood, MA, PMP1; Kathryn Ambler, MSc2; Negar Dehghan Noudeh, MBT1; Patty Wickson, eMBA, CHE2; and Chester Ho, MD3,4
Affiliations: 1W21C, O’Brien Institute for Public Health, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada; 2Innovation and Business Intelligence, Alberta Health Services, Calgary, AB, Canada; 3Department of Medicine, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, AB, Canada; 4Glenrose Rehabilitation Hospital, Alberta Health Services, Edmonton, AB, Canada
Acknowledgments: The authors would like to thank Wrechelle Ocampo for support with study conceptualization, Mackenzie Murawsky for support with data collection, Marissa Carter, PhD, MA, for support with trial design and statistical analysis, John Nesbitt, MD, and the team at the outpatient clinic, and the Innovation and Business Intelligence team members at Alberta Health Services for their support with funding acquisition. A special thanks to all the health care providers who supported the study and patients who took part in this study.
Author Contributions: The final manuscript has been seen and approved by all authors, and all authors accept full responsibility for the design and conduct of the study, had access to the data, and controlled the decision to publish.
Disclosure: The authors disclose no financial or other conflicts of interest.
Funding: This project was funded by CAN Health West, with in-kind contributions from W21C (study leadership and project management), Alberta Health Services (study leadership and project management), and NanoTess (in-service training for appropriate device use, provision of cameras, and consultation with external wound care expert).
Ethics Statement: The study was conducted following the research protocol that was reviewed and approved by the Conjoint Health Research Ethics Board on November 13, 2022 (reference number REB22-1394). All procedures were completed in compliance with the ethics approval, and the study followed the ethical standards regarding participant privacy and confidentiality.
Correspondence: Anna Bradford, MBT; W21C GD01, CWPH Building, 3280 Hospital Dr NW, Calgary, AB T2N 4Z6, Canada; anna.bradford1@ucalgary.ca
Manuscript Accepted: May 7, 2026
References
- Falanga V, Isseroff RR, Soulika AM, et al. Chronic wounds. Nat Rev Dis Primers. 2022;8(1):50. doi:10.1038/s41572-022-00377-3
- Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv Wound Care (New Rochelle). 2015;4(9):560-582. doi:10.1089/wound.2015.0635
- Queen D, Botros M. The true cost of wounds for Canadians: annual update. Wound Care Canada. 2025;23(2):37-42. doi:10.56885/032346qumxzp
- Health Canada. Medical device license: NanoSALV Catalytic Advanced Wound Care Treatment Matrix. Government of Canada. Accessed June 16, 2026. https://health-products.canada.ca/mdall-limh/information?deviceId=1053891&deviceName=NANOSALV+CATALYTIC+ADVANCED+WOUND+CARE+TREATMENT+MATRIX&licenceId=108236&type=active&lang=&lang=eng.
- NanoTess. How to Use. Accessed June 16, 2026. https://www.nanotess.com/pages/how-to-use
- Zhang Z, Xue H, Xiong Y, et al. Copper incorporated biomaterial-based technologies for multifunctional wound repair. Theranostics. 2024;14(2):547-570. doi:10.7150/thno.87193
- Pereira-Silva P, Borges J, Sampaio P. Recent advances in metal-based antimicrobial coatings. Adv Colloid Interface Sci. 2025;344:103590. doi:10.1016/j.cis.2025.103590
- Driver VR, Gould LJ, Dotson P, et al. Identification and content validation of wound therapy clinical endpoints relevant to clinical practice and patient values for FDA approval. Part 1. Survey of the wound care community. Wound Repair Regen. 2017;25(3):454-465. doi:10.1111/wrr.12533
- Driver VR, Gould LJ, Dotson P, Allen LL, Carter MJ, Bolton LL. Evidence supporting wound care end points relevant to clinical practice and patients’ lives. Part 2. Literature survey. Wound Repair Regen. 2019;27(1):80-89. doi:10.1111/wrr.12676
- US Food and Drug Administration. Chronic cutaneous ulcer and burn wounds - developing products for treatment. June 2006. Accessed August 26, 2025. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/chronic-cutaneous-ulcer-and-burn-wounds-developing-products-treatment
- Aranz Medical. How SilhouetteStar Works-Silhouette v3.13. 2012. https://www.aranzmedical.com/wp-content/uploads/How-SilhouetteStar-Works.pdf
- Rich JT, Neely JG, Paniello RC, Voelker CCJ, Nussenbaum B, Wang EW. A practical guide to understanding Kaplan-Meier curves. Otolaryngol Head Neck Surg. 2010;143(3):331-336. doi:10.1016/j.otohns.2010.05.007
- Walters J, Cazzell S, Pham H, Vayser D, Reyzelman A. Healing rates in a multicenter assessment of a sterile, room temperature, acellular dermal matrix versus conventional care wound management and an active comparator in the treatment of full-thickness diabetic foot ulcers. Eplasty. 2016;16:e10.
- Robles-Tenorio A, Ocampo-Candiani J. Venous leg ulcer. [Updated 2022 Sep 18]. In: StatPearls [Internet]. StatPearls Publishing; 2026. Available from: https://www.ncbi.nlm.nih.gov/books/NBK567802/
- Raja JM, Maturana MA, Kayali S, Khouzam A, Efeovbokhan N. Diabetic foot ulcer: a comprehensive review of pathophysiology and management modalities. World J Clin Cases. 2023;11(8):1684-1693. doi:10.12998/wjcc.v11.i8.1684
- Beyene RT, Derryberry SL Jr, Barbul A. The effect of comorbidities on wound healing. Surg Clin North Am. 2020;100(4):695-705. doi:10.1016/j.suc.2020.05.002
- Talari K, Goyal M. Retrospective studies - utility and caveats. J R Coll Physicians Edinb. 2020;50(4):398-402. doi:10.4997/jrcpe.2020.409
- Bradford A, de Grood J, Ambler K, Dehghan Noudeh N, Wickson P, Ho C. Prospective evaluation of the clinical effectiveness of an innovative catalytic wound care technology. Wounds. Forthcoming.






