Challenging Conventions: Transulnar Route for Simultaneous Bilateral SFA Angioplasty
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Sarah Misbah, MD1; Alexis Albert Annan, MD1; Sridevi Pitta, MD, MBA, FACC, FSCAI, RPVI3; Ashley Ferguson, BSN, RN2
1Texas Health Resources, Denton, Texas;
2Texas Health Presbyterian Hospital Denton, Texas
3Professor of Medicine, Department of Internal Medicine
Anne-Brunette School of Medicine, Texas Christian University, Fort Worth, Texas; Interventional Cardiologist, Texas Health Presbyterian Hospital Denton;
Chair, Quality Assurance and Performance Improvement Committee; Medical Director, Cardiology Service Line, Texas Health Presbyterian Hospital Denton;
Core Faculty, Internal Medicine Residency Program Texas Health Resources HEB/Denton
Correspondence: SarahMisbah@TexasHealth.org
Background/Introduction
The transulnar access approach for bilateral angioplasty of superficial femoral arteries (SFA) is relatively uncommon compared to other access methods. Transradial access is more frequently used as an alternative to traditional transfemoral approaches.1 A recent study evaluating transulnar access for peripheral interventions showed a high success rate of 97.14% in 35 procedures.2 One of the limiting anatomic factors when comparing upper and lower extremity access sites is the narrower lumen and the larger distance between the puncture site and target lesion, whereas the main advantage is rarer atherosclerotic involvement.3
The majority of endovascular procedures throughout the body, including those for peripheral arterial disease (PAD), have been performed through a transfemoral approach, given its large diameter and relatively easy trajectory to many target areas. However, a growing body of evidence, particularly from interventional cardiology literature, has demonstrated that transradial access (TRA) is both safe and effective, with lower complication rates.4 However, understandably, many of these patients have severe PAD and may require access crossover mid-procedure to obtain an alternate access.
There have been some cases and observational studies reporting transulnar access for percutaneous coronary intervention (PCI). However, no case has been reported using transulnar access for peripheral interventions; specifically, simultaneous bilateral superficial femoral artery (SFA) interventions. Multiple access techniques have been reported in the literature for SFA angioplasty, such as bilateral radial access for kissing stent procedures in the iliac arteries.4 Transfemoral access remains a common approach for SFA interventions, and in some complex cases, a bilateral transpopliteal approach has been used successfully for treating long SFA occlusions.5
We present the case of a 70-year-old female who presented with left lower extremity (LLE) critical limb ischemia (CLI) and underwent a bilateral SFA intervention via the transulnar route.
Case Presentation
This is a 70-year-old female with a past medical history of premature coronary artery disease, familial hyperlipidemia, and intolerance to statins. She is on PSCK9 inhibitors and inclisiran infusions, underwent on-pump coronary artery bypass graft (CABG) surgery x 3 with occluded saphenous vein grafts not amenable to redo, and prior PCIs, with a recently failed transfemoral access, and has chronic diastolic heart failure. She has Protein C, S, and Factor V Leiden deficiency, a history of deep vein thrombosis and pulmonary embolism, and an inferior vena cava filter in place; she is also on anticoagulation with apixaban. She also has extensive peripheral vascular disease with prior stenting and in-stent stenosis.
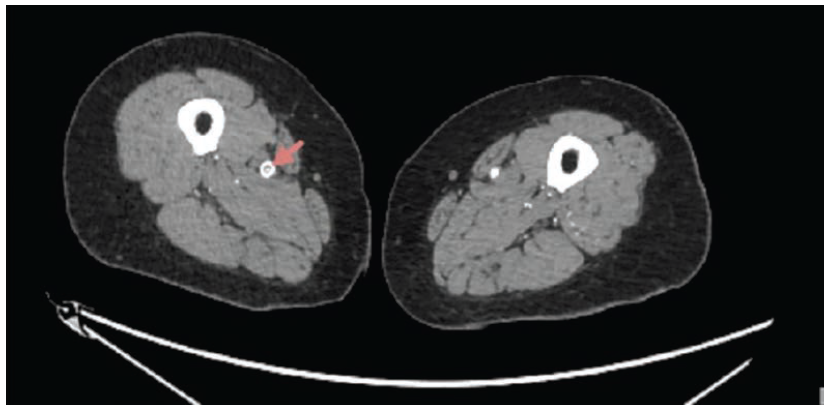
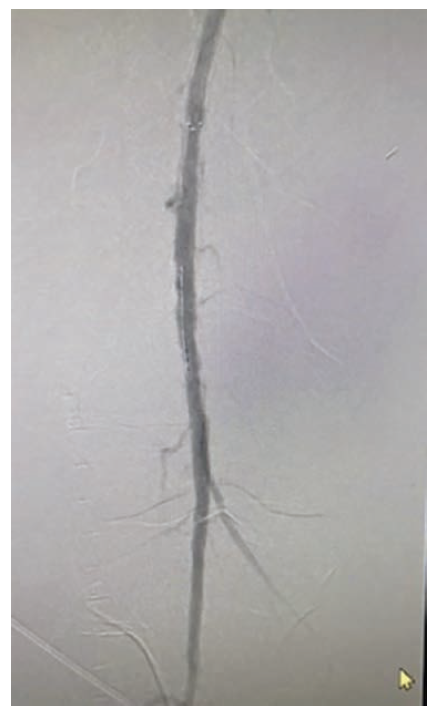
The patient presented with ongoing bilateral lower extremity pain, progressively worsening over the last few weeks. Over the last few days, she noticed changes in temperature and color on her left leg and foot. She denied chest pain or shortness of breath. The physical exam was pertinent for nonpalpable pulses in the bilateral lower extremities, as well as delayed capillary refill. While in the emergency department (ED), her troponin was negative, and beyond the basic labs, she underwent a venous Doppler of the bilateral lower extremities, which was negative, and a subsequent arterial duplex ultrasound of the left lower extremity, which revealed a mid- SFA critical stenosis with monophasic flow below the stenosis. A computed tomography angiography aorta runoff revealed a stent in the right SFA with moderate to severe in-stent stenosis, near complete occlusion over a 2.2 cm segment in the proximal left SFA, and severe peripheral vascular disease bilaterally. She was given aspirin and intravenous fluids in the ED, and her apixaban was held.
Interventional Cardiology was consulted with a resulting plan for peripheral angioplasty the following morning. Given her severe peripheral vascular disease and the fact that the patient was well known to the operator and cath lab due to frequent procedures and outpatient follow-up, it had already been decided that a groin access would not be feasible in this patient, as a difficult groin access was likely. Thus, it was agreed to proceed with the right radial access. She was prepped for radial access; however, the right radial artery, when scanned, revealed low flow and mildly occlusive PAD. Subsequently, access was switched to the right ulnar artery, appearing fully patent on ultrasound and pulsatile. The patient was deemed to have an adequate collateral blood supply to her hand.
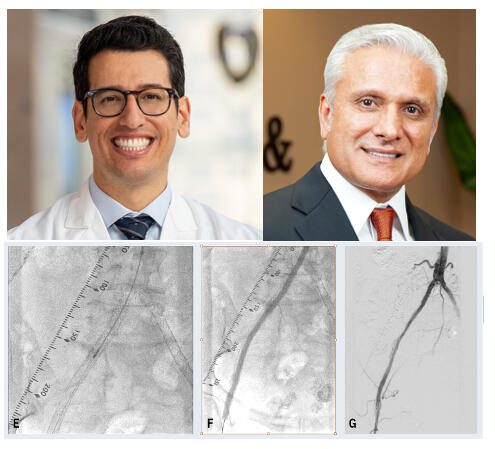
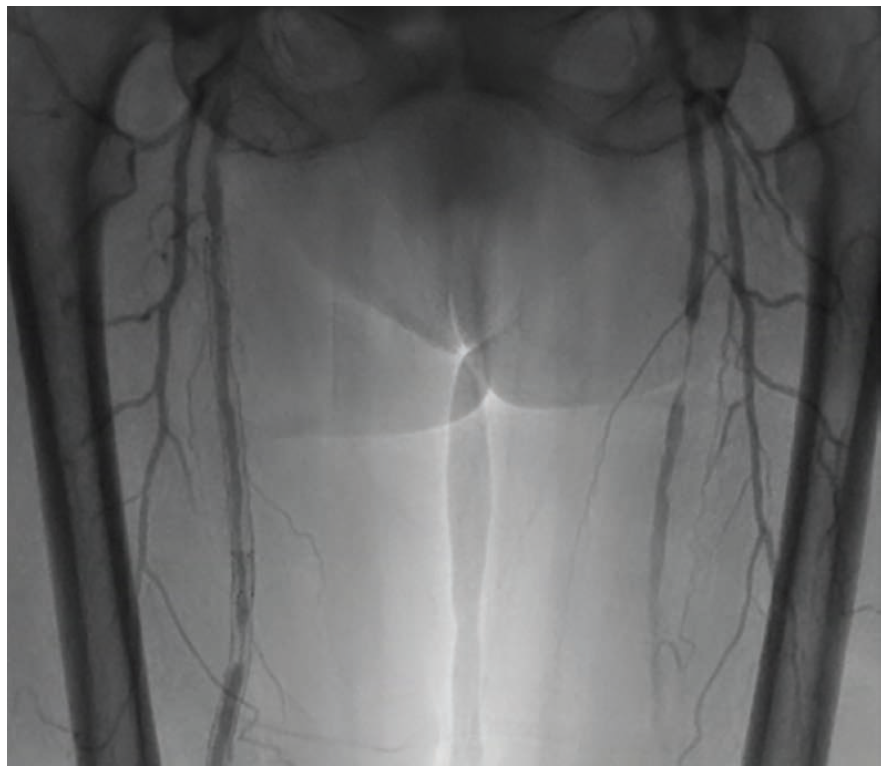
We proceeded with the same steps as for radial access. Local anesthetic was administered and arterial puncture achieved by palpation of the site of maximum pulse prominence and then by using ultrasound guidance. The needle was inserted at a 45- to 60-degree angle along the vessel axis, moving lateral to medial, thereby avoiding the ulnar nerve. A 6 French (Fr) Glidesheath Slender (Terumo) was placed using the modified Seldinger technique and a .035-inch x 180 mm Roadrunner guidewire (Cook Medical) was advanced. Intra-arterial vasodilators nitroglycerin, verapamil, and heparin were administered. We then inserted the catheter over the guidewire and removed the wire. The sheath was exchanged for a 6 Fr 119 cm Radial to Peripheral (R2P) guide sheath (Terumo), and a Runthrough wire (Terumo) was threaded. The sheath was maneuvered into the aorta, then the internal and external iliac arteries. First targeted was the left SFA, which required some protracted wiring; however, we were eventually able to push through without having to change or escalate to a different wire. Because this procedure was performed via right ulnar access, device length was an important consideration in addition to profile compatibility. The Shockwave E8 intravascular lithotripsy (IVL) balloon was chosen in part because its 150 cm shaft length and 6 Fr compatibility allowed delivery to the target lesion from an upper-extremity approach. A 6 Fr 5.0 mm x 80 mm Shockwave E8 IVL balloon was inserted over the wire. We performed IVL using multiple pulses, moving from proximal to distal. After two pulses, our balloon ruptured, requiring insertion of a second balloon, and multiple pulses were delivered successfully. The balloon was subsequently removed intact. A subsequent peripheral angiogram of the left SFA revealed adequate flow. A 200 cm, 6 Fr, 6.0 mm x 100 mm Misago self-expanding stent (Terumo) was deployed. Post dilatation was performed with a 6.0 mm x 100 mm Crosstella balloon (Terumo), expanded to a maximum pressure of 8 atmospheres for 30 seconds. The balloon was subsequently removed intact. The wire was exchanged and navigated into the right SFA.
Intravascular ultrasound (IVUS)-guided IVL was performed. A 6 Fr 5.0 mm x 80 mm Shockwave E8 IVL balloon was inserted over the wire and multiple pulses were delivered. The balloon was removed intact and the wire was exchanged. A 4 Fr 150 cm Glidecath was inserted. The sheath was exchanged for a 6 Fr .021-inch x 10 cm GlideSheath Slender. A peripheral angiogram revealed good flow. The sheath was removed and a TR Band (Terumo) was placed for hemostasis with inflation to 11 mL.
The patient tolerated the procedure well, with no further complications. She reported improvement of her symptoms with no further rest pain in the bilateral lower extremities.
Discussion
This case demonstrates the feasibility of using a transulnar approach for bilateral SFA angioplasty. The patient presented with a significant in-stent stenosis in the right SFA and a short occlusion in the left SFA, both of which were successfully treated via percutaneous transluminal angioplasty (PTA) and stent placement through the ulnar artery.
The choice of the transulnar approach in this case was influenced by the need to address bilateral SFA lesions. While bilateral transradial access is an option, the transulnar approach provided a single access point to potentially treat both lesions simultaneously, which can be advantageous in reducing the risk of access-site complications associated with multiple punctures.
Peripheral vascular interventions for infrainguinal disease are traditionally conducted via the common femoral artery (CFA) and its branches, either antegrade on the ipsilateral limb or retrograde via the contralateral limb. Transfemoral access is the traditionally used approach for peripheral vascular intervention because the puncture is nearly effortless, provides good backup support for the intervention, and allows the use of large femoral sheaths (6-8 Fr).4 However, femoral artery access has several limitations, including limited pushability for infrapopliteal lesions and challenging access in total complete occlusions of the CFA. Previously repaired femoral disease, either from prior surgery or stenting, also poses challenging access. It can be compromised by scar tissue, or if the lesion itself involves the CFA, a crossover to the contralateral access becomes mandatory, which is not always possible in cases of calcified, tortuous, or angled iliac arteries. The primary disadvantage of the femoral technique is the high incidence of bleeding complications and prolonged immobilization resulting from the limited applicability of the closure devices.4
Therefore, the use of safe and effective alternative access sites for PVI is crucial in the management of PAD and for limb salvage. The most commonly used alternative access sites are the radial, popliteal, and pedal approaches. Other options include brachial and axillary access sites.
Ulnar artery (UA) access studies have not been previously published for peripheral vascular intervention; however, numerous publications describe its use in coronary intervention. In the SWITCH registry,6 Agostoni et al reported switching directly to the ipsilateral ulnar artery in cases of failed radial sheath insertion. In the randomized PCVI-CUBA trial,7 consecutive unselected patients were randomized to the ulnar or radial approach before performing the Allen test and palpating the forearm pulses. Successful access was achieved in 93.1% of patients in the ulnar group and 95.5% of patients in the radial group (P=.82), and the arterial diameters did not differ significantly, as determined by ultrasound.
The disadvantages of UA access over radial access are that UA access is a more difficult puncture due to limited palpability, as well as the seemingly more difficult compression; however, the latter factor does not translate into a higher complication rate, according to the literature.8
The main concern with switching to ipsilateral or contralateral UA access is the question of hand ischemia. There are certain prerequisites when choosing the UA, such as pre-procedure Allen testing or Barbeau waveform analyses. The Allen test is performed as follows: both radial and ulnar arteries are occluded at the wrist, and the patient is asked to make a tight fist until the palmar surface of the hand branches. Pressure is subsequently released from each of the vessels, ie, the radial artery and UA in turn, and their patency and that of the superficial palmar arch is confirmed by the return of color to the hand/palm.9 However, care must be taken when interpreting results. Shah et al note that the Allen test can often be misleading and thus be an inaccurate measure of contralateral blood supply.10
Another measure of establishing palmoplantar patency is by doing the Barbeau and reverse Barbeau waveform analyses. The reverse Barbeau test involves placing a pulse oximeter on the patient’s 5th digit followed by baseline pulse waveform analysis. The UA is then compressed for 2 minutes and a pulse waveform post-compression response is graded according to the Barbeau classification. Normally, operators will attempt a transulnar approach in patients with Barbeau D waveform and after re-evaluation with a reverse Barbeau waveform analysis.9
Ulnar Access Limitations. While our case highlights the potential benefits of the transulnar approach, it is important to acknowledge its limitations. Ulnar access, just like radial access, is associated with complications such as nerve injury leading to paresthesia and hematoma formation causing subsequent nerve injury. The learning curve for ulnar artery access may be steeper compared to more traditional approaches. Failure of puncture is a more common cause of crossover in the ulnar group, while radial artery spasm is more likely to hinder radial access. Furthermore, unlike the radial artery, the ulnar artery has no adjacent bony structure to provide compressive support, making TR Band placement more challenging. Literature and operator experience show that higher pressure or prolonged hemostasis of the ulnar artery may be necessary to prevent post-procedure access site complications such as hematoma.
Despite the more recent use of transradial access, it was underutilized due to technical and anatomic limitations in the past, with the larger diameter and short delivery shafts of the first-generation catheters. However, recent technology such as newer stents are now 6 Fr sheath compatible, with longer shafts ranging from 120-135 cm, and there has been development of hydrophilic, more flexible, kink-resistant long sheath and sheath guides.11
Given this information, it is important to consider device limitations when considering alternative accesses. Data is available regarding device limitations in alternative accesses for coronary procedures and may mimic inadequacies in peripheral interventions.
Prior studies found that mainly less complex lesions limited to above the knee are successfully accessed via transradial/transulnar access. However, Sher et al showed that with appropriate device selection, more complex and farther lesions were successfully accessed and treated.4 This signifies that it is important to consider device compatibility, and lesion location and length, as well as appropriate patient selection.
Due to less conventional use of the transulnar access, there are few to no UA-specific devices present in the market, and thus, without proper device selection, this is a limitation. For example, although PTA balloons and bare metal stents are available in the appropriate length for most infrainguinal lesions, there are currently no drug-coated balloon/drug-eluting stent options that are long enough to be compatible with 6 Fr sheaths. This is especially important given that DCB angioplasty is superior to PTA specifically for femoropopliteal restenosis or in-stent stenosis. In our patient, we managed two lesions with a single access: an in-stent stenosis and a de novo lesion. We were able to treat both with multiple pulses of IVL and did not need to put in a DCB. If a DCB had been required, there isn’t a long enough sheath available for deployment.4
Despite the concern, Fernández et al12 reported that the use of the ipsilateral UA when the radial artery is inaccessible due to tortuosity, spasms, perforation, etc., is acceptable. This decreases the need for cross-over to the contralateral radial access or femoral access. No significant evidence is present in the literature to support increased rates of hand ischemia when the homolateral UA is accessed after a failed radial access. This is likely due to variations in collateral blood supply to the hand.
It is important to note that as compared to transradial access for PAD, the transulnar approach has been less extensively studied. A meta-analysis comparing transradial and transulnar access showed a high success rate of 97.14% in 35 procedures using transulnar access for peripheral interventions.13 An Egyptian study showed radial and ulnar access for PCI have comparable outcomes when performed by experienced radial operators.8
Furthermore, it is important to note that different operators may have different experiences. Hahalis et al found the transulnar strategy inferior to the transradial strategy due to a high rate of crossover in the transulnar access arm.14 However, Gokhroo et al found transulnar access non-inferior to transradial access when performed by operators who normally used radial access but had experience of performing at least 50 ulnar artery cannulations.15
This further underscores the importance of having trained operators for a favorable outcome and a less steep learning curve. Reported technical failure for transradial procedures is between 1% and 7%, mainly related to the learning curve.1
Ulnar artery access is a safe and practical alternative, when safely performed by operators experienced in radial access. It is especially useful when the radial and/or femoral artery cannot be used due to prior procedural access, occlusion, or anatomical variations. Furthermore, the ulnar artery is wider, runs a straighter course, and is easily palpable, and is less prone to vasospasm as compared to the radial artery due to a lesser number of alpha receptors. The radial artery, on the other hand, has many limitations such as weak radial pulse, prior instrumentation and hence fibrosis leading to occlusion, radial artery spasms, and considerations for preservation of the radial artery for surgical grafts or fistulas.
Conclusion
This case demonstrates that, with appropriate patient selection, operator experience, and contemporary endovascular tools, the transulnar approach can be a safe and effective method for treating complex SFA lesions. Further studies are warranted to evaluate the long-term outcomes and cost-effectiveness of this approach compared to other access strategies for peripheral vascular intervention. Specifically, research should focus on identifying the ideal patient population and anatomical characteristics that favor the transulnar approach, as well as developing specialized devices and techniques to further improve its safety and efficacy. This case contributes to the growing body of evidence supporting the use of alternative access sites for peripheral vascular intervention and underscores the importance of individualized treatment strategies tailored to patient-specific factors.
References
1. Kedev S, Zafirovska B, Dharma S, Petkoska D. Safety and feasibility of transulnar catheterization when ipsilateral radial access is not available. Catheter Cardiovasc Interv. 2014; 83(1): E51-E60. doi:10.1002/ccd.25123
2. Gómez-Pena S, Trejo C, Pérez-García C, et al. Transulnar approach as an alternative access site for neuroendovascular procedures. The Neuroradiology Journal. 2024; 38(4): 488-495. doi:10.1177/19714009241303120
3. Ruzsa Z, Tóth K, Nemes B, et al. Transradial and transulnar access for iliac artery interventions using sheathless guiding systems: A feasibility study. Catheter Cardiovasc Interv. 2016; 88(6): 923-931. doi:10.1002/ccd.26592
4. Sher A, Posham R, Vouyouka A, et al. Safety and feasibility of transradial infrainguinal peripheral arterial disease interventions. J Vasc Surg. 2020; 72(4): 1237-1246.e1. doi:10.1016/j.jvs.2020.02.016
5. Yilmaz S, Sindel T, Lüleci E. Bilateral transpopliteal approach for treatment of complex SFA and iliac occlusions. Eur Radiol. 2002; 12(4): 911-914. doi:10.1007/s003300101043
6. Agostoni P, Zuffi A, Faurie B, et al. Same wrist intervention via the cubital (ulnar) artery in case of radial puncture failure for percutaneous cardiac catheterization or intervention: the multicenter SWITCH registry. Int J Cardiol. 2013 Oct 25; 169(1): 52-6. doi:10.1016/j.ijcard.2013.08.080
7. Aptecar E, Pernes JM, Chabane-Chaouch M, et al. Transulnar versus transradial artery approach for coronary angioplasty: the PCVI-CUBA study. Catheter Cardiovasc Interv. 2006; 67(5): 711-720. doi:10.1002/ccd.20679
8. Shafiq M, Mahmoud HB, Fanous ML. Percutaneous trans-ulnar versus trans-radial arterial approach for coronary angiography and angioplasty, a preliminary experience at an Egyptian cardiology center. Egypt Heart J. 2020; 72(1): 60. doi:10.1186/s43044-020-00089-7
9. Taylor BA, Alzahrani F, Levi E, et al. Absence of ulnar artery inflow detected by Allen’s test prior to radial forearm free flap. Plast Reconstr Surg Glob Open. 2017; 5(4): e1299. doi:10.1097/GOX.0000000000001299
10. Shah AH, Pancholy S, Shah S, et al. Allen’s test: does it have any significance in current practice?. J Invasive Cardiol. 2015; 27(5): E70-E73.
11. Ruzsa Z, Tóth K, Nemes B, et al. Transradial and transulnar access for iliac artery interventions using sheathless guiding systems: A feasibility study. Catheter Cardiovasc Interv. 2016; 88(6): 923-931. doi:10.1002/ccd.26592
12. Fernández R, Zaky F, Ekmejian A, et al. Safety and efficacy of ulnar artery approach for percutaneous cardiac catheterization: systematic review and meta-analysis. Catheter Cardiovasc Interv. 2018; 91(7): 1273-1280. doi:10.1002/ccd.27479
13. Abdullah Al-Shamari MF, Zreigh SMM, Mosa AA, et al. Transulnarversus transradial artery access in patients undergoing cardiac procedures: a systematic review and meta-analysis. Ann Med Surg (Lond). 2026 Jan 21; 88(2): 1806-1814. doi:10.1097/MS9.0000000000004696
14. Hahalis G, Tsigkas G, Xanthopoulou I, et al. Transulnar compared with transradial artery approach as a default strategy for coronary procedures: a randomized trial. The Transulnar or Transradial Instead of Coronary Transfemoral Angiographies Study (the AURA of ARTEMIS Study). Circ Cardiovasc Interv. 2013 Jun; 6(3): 252-261. doi:10.1161/CIRCINTERVENTIONS.112.000150
15. Gokhroo R, Kishor K, Ranwa B, et al. Feasibility of ulnar artery intervention (AJMER ulnar artery intervention group study: AJULAR): early. J Am Coll Cardiol. 2015 Mar; 65 (10_Supplement) A1684. https://doi.org/10.1016/S0735-1097(15)61684-9