The ALL-RISE Trial: FFRangio and the Next Step in Coronary Physiology
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
CLD talks with Ajay J. Kirtane, MD, SM.
Director of Columbia Interventional Cardiovascular Care and Professor of Medicine at Columbia University Irving Medical Center, New York, New York; Cardiovascular Research Foundation, New York, New York
Presented at ACC.26 by Dr. Kirtane and published simultaneously in the New England Journal of Medicine1, the ALL-RISE trial tested whether angiography-derived physiologic assessment with FFRangio (CathWorks, now part of Medtronic) could match the clinical performance of conventional invasive wire-based physiology in patients undergoing evaluation for percutaneous coronary intervention (PCI).
Can you share your perspective on the current state of physiologic assessment and tell us why the ALL-RISE trial was conducted?
 Most interventional cardiologists understand that physiology makes sense. It helps us identify the right patients for PCI and stenting. That is why physiologic assessment carries a Class 1A recommendation in the guidelines. It is supported not only by its clinical utility, but also by its high economic value, because it often results in fewer stents being placed, while ensuring that stents are used in the patients who are most likely to benefit. The challenge is that, in practice, there are workflow limitations that can make physiologic assessment burdensome because of the additional steps involved.
Most interventional cardiologists understand that physiology makes sense. It helps us identify the right patients for PCI and stenting. That is why physiologic assessment carries a Class 1A recommendation in the guidelines. It is supported not only by its clinical utility, but also by its high economic value, because it often results in fewer stents being placed, while ensuring that stents are used in the patients who are most likely to benefit. The challenge is that, in practice, there are workflow limitations that can make physiologic assessment burdensome because of the additional steps involved.
With current wire-based technologies, you have to anticoagulate, engage with a guide catheter, zero and then equalize the pressure system, and work through a series of procedural steps that add time and manipulation to the case. In many cases, after doing all of that, you may ultimately decide not to place a stent. Psychologically and practically, I think that has made widespread adoption more difficult than the guidelines would suggest it should be.
At the same time, we now have angiography-based systems that can analyze the angiogram itself, such as FFRangio, and generate physiologic values with a high degree of accuracy. Studies comparing systems like FFRangio with wire-based fractional flow reserve (FFR) have shown very good correlation between the two. But there has still been a gap in confidence for some operators. The question has been: can I really trust it? Will clinical outcomes be the same if I use this instead of a wire-based approach?
That was the rationale for designing ALL-RISE. At its core, the study was intended to answer a straightforward question: if you use this angiography-based physiologic assessment system, will clinical outcomes be comparable to those achieved with wire-based physiology? The trial showed that they were.
Can you briefly describe the trial design and outcomes?
We randomly assigned 1,930 patients to either an FFRangio-guided strategy or a wire-based physiologic assessment strategy. In both groups, angiography was performed first. Once a lesion was identified in the 50% to 90% range and considered appropriate for physiologic assessment, the patient was randomized.
In the FFRangio arm, treatment decisions were made on the basis of the angiographic physiologic assessment. In the wire-based arm, operators used the same thresholds that are standard in practice. You could either do what’s called a non-hyperemic index or FFR and make your decision based on that.
Patients were then followed for one year. The primary endpoint was major adverse cardiac events (MACE), defined as death, myocardial infarction, or unplanned clinically driven revascularization. In addition to clinical outcomes, we also looked at procedural metrics, including the time required to perform the physiologic assessment, contrast use, radiation exposure, and total procedure time.
When it came to clinical outcomes, the two groups were the same at one year. We did a noninferiority analysis, but if you look at the event curves, they are essentially superimposable. That is important, because it showed that by using FFRangio, you can preserve the clinical performance of wire-based assessment while potentially simplifying workflow and saving time in the cath lab.
We also saw a signal for less bleeding in the FFRangio arm, with the bleeding rate about half of what it was in the wire-based arm. ALL-RISE was not statistically powered for that endpoint, and the absolute event rates were low, so you have to be cautious about overinterpreting it. But mechanistically it makes sense, because we were not giving anticoagulation or using guiding catheters in the same way.
In addition, procedures were shorter in the FFRangio group. On average, there was about a 5-minute reduction in procedure time. FFRangio was also faster in terms of the physiologic assessment itself, because it calculated the value faster, and the strategy also used less contrast and less fluoroscopy. That makes sense, because many of the steps required for conventional wire-based assessment were eliminated.
This trial was specifically designed to evaluate clinical outcomes, moving beyond earlier studies that focused primarily on the diagnostic performance of FFRangio.
Yes, exactly. I think it is important to conduct clinical outcomes studies because any new technology can be shown to correlate with an existing measure, but that is not the same as demonstrating how the patients we actually treat will do.
That distinction is especially important for a technology analyzing an angiographic image, where you are not advancing a wire or performing direct physiologic manipulation. Operators want to be confident that the information derived from that analysis will translate into appropriate patient management.
In cardiovascular medicine, we feel strongly that outcomes studies are necessary to truly earn clinicians’ trust and allow them to feel comfortable adopting a new approach. I had used the technology myself in clinical practice, but I still wondered whether the outcomes would in fact be the same. In theory, they should be, but as we know in clinical medicine, what seems likely does not always prove to be true.

Were there patients in the trial with more than one intermediate lesion?
Yes. It was a smaller proportion of the overall cohort, but that was certainly part of the study, and the technology can be used for multiple lesions and multiple vessels. There were also patients in the trial in whom more than one vessel was interrogated.
The difference is in the workflow. With a wire-based approach, you generally have to wire one vessel, do a pullback, and then wire the second vessel — sometimes with a different guide catheter. With this system, if you are looking at the left coronary system, for example, you can run the analysis and obtain information on both the LAD and the circumflex from the same angiographic dataset, which is a meaningful advantage. You can also run the analysis on the RCA without any additional in-room procedural steps.
Could you walk us through the FFRangio workflow and how it differs from wire-based physiologic assessment?
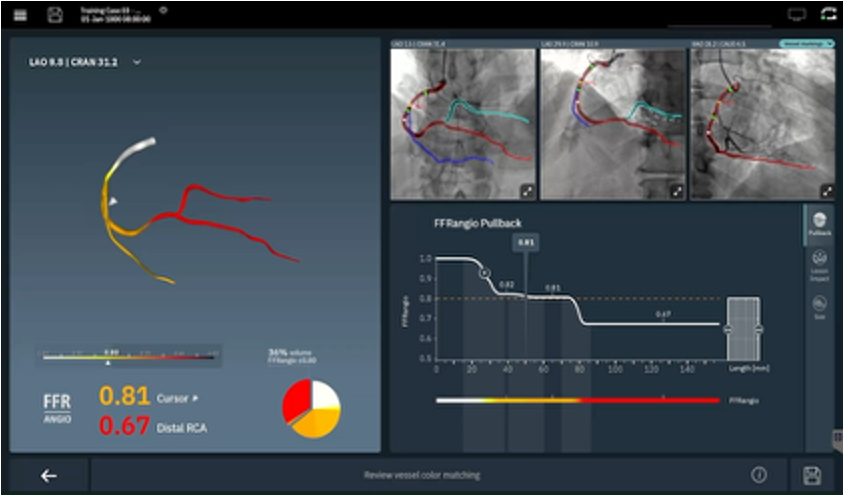
It begins with the diagnostic angiogram. With this technology, you do need three views, and that is intentional because it is part of what allows the analysis to be accurate. Those angiographic images are then transferred to a proprietary console. Within that system, the software uses AI to suggest which views might work best and make sense for the vessel being assessed. You bring up those views, and the software traces the coronary arteries automatically, identifying the vessel anatomy. You then mark the lesion of interest. Importantly, FFRangio does not only provide a physiologic assessment for that single lesion; it gives you physiologic information for all of the vessels on that side.
The physician still has to look it over and make sure it makes sense. In most cases, I do not typically need to adjust the tracing, although occasionally I do. Once that review is complete, you run the analysis, and after a brief interval, usually about a minute, the system provides the values you need.
That essentially is the workflow. It can be done in the procedure room, although we typically do it in the control room, and it is all performed without instrumenting the patient. What I usually tell the patient is, “Give us a moment while we calculate these values, and then we will know the significance of these blockages.” In some cases, if you image one coronary system first and then move to the other side, the analysis can even be running in parallel while you are acquiring the remaining angiograms, so the results are ready by the time the angiogram is complete.
It is very different from conventional wire-based physiology. If I am going to perform FFR, I need to open a pressure wire, open a guide catheter, give anticoagulation, zero the pressure system, engage the catheter, equalize pressures, carefully advance the wire across the lesion, then disengage the guide and make sure anticoagulation is adequate. Those are all real procedural steps, and while the risks are small, there is still some risk associated with guide-catheter manipulation and instrumentation in general.
I think the appeal is intuitive to interventionalists and the team in the lab. As long as the analysis can be performed efficiently, not having to do those added procedural steps is clearly an advantage.
How are cath lab staff involved?
This is an important part of the story, because staff can really be involved. Depending on how a lab is set up, the analysis can be initiated by a superuser, a technologist, or a nurse. Team members can help run the analysis, make sure the correct vessel is selected, and enter the required parameter, which is blood pressure. They can get the process started, and then the physician can come over, review it, and confirm that everything looks appropriate.
What is appealing about that workflow is that it strengthens the team-based aspect of the procedure. Different members of the cath lab team can be doing different things at the same time, so the work can happen in parallel. By contrast, with a conventional pressure-wire setup, everything is much more sequential and linear.
With this approach, non-physician staff can take on a meaningful role in the workflow, with physician oversight, and I think that is genuinely empowering for the cath lab team.
Physiologic lesion assessment has been supported for years, yet adoption remains uneven. FFRangio seems like technology that could be adopted much more quickly because it is more user-friendly.
That is part of the goal. What’s also appealing is that because this is a software-based platform, it can be iterated very quickly. The version I first used years ago in the validation studies is very different from the version that existed when we got it in our cath lab, and the current version is much better. We have made suggestions over time about features and refinements, and because it is software, those kinds of changes can be implemented much more rapidly.
That is very different from hardware. If you introduce a new stent platform or even make meaningful changes to an existing one, you have to go through a much more extensive validation process. With software, you have much more flexibility to improve the user experience and functionality on a faster cycle, provided you are not fundamentally changing the underlying algorithm.
Noninferiority trials have become increasingly important across interventional cardiology. As people are evaluating a noninferiority trial, what should they look for to judge whether it is a strong study and well designed?
One thing to pay attention to in a noninferiority trial is the actual event rates, not just whether the study technically met its statistical margin. You can have a situation in which the treatment group looks a little worse than the control group, but still satisfies the noninferiority criterion because it remains within the prespecified margin. Statistically, that may be acceptable, but clinically it can still give people pause if the event rates are directionally higher.
That is not what we saw here. In this trial, the event rates were essentially the same: 7.1% in the wire-based group and 6.9% in the FFRangio group.1 So this was not a case where the new strategy barely cleared the bar despite looking somewhat worse. The clinical outcomes were, in practical terms, virtually identical.
The other thing to consider is whether the new approach offers any meaningful advantages beyond being simply comparable. Noninferiority is one thing if you are talking about a very similar, essentially incremental, technology. But in this case, there are additional features that make the strategy attractive. The workflow is simpler, the procedure is more efficient, and you avoid additional procedural instrumentation.
If you ultimately decide not to treat a lesion, being able to avoid anticoagulation and the other steps that come with wire-based assessment is a real advantage. So when I look at a noninferiority trial, I always ask whether this is just a “me too” technology or whether it offers some material benefit beyond similar outcomes.
In this case, I think it does. ALL-RISE showed similar clinical outcomes between the two groups, but with clear workflow advantages for FFRangio. If that makes physiologic assessment easier to incorporate into routine practice, then it could help improve overall adoption, which is a very good thing.
What do you see as the future of this technology?
First, the hope is that this trial will make people more enthusiastic about using physiology and, ultimately, increase adoption. At the same time, it is important to be clear about what was and was not studied in this trial. We did not study certain populations in depth. Only about 10% of patients had acute coronary syndromes, and most of those patients were biomarker-negative. Questions such as non-culprit vessel assessment in acute coronary syndromes remain important areas for future study.
I also think there may be opportunities to expand this general approach beyond epicardial lesion assessment. One potentially important direction would be the assessment of microvascular dysfunction. Right now, that really still requires a wire-based approach, and it can be somewhat finicky. If an angiography-based method could eventually be developed and validated for that purpose, it would be a major advance for patients.
There is a great deal that could come next. The interface can certainly continue to improve, and software-based platforms can be iterated quickly. But the version studied in this trial is the same one I was using in clinical practice, so it was reassuring to see that specific version validated in a randomized outcomes study.
Any final thoughts?
I would emphasize that this was an important clinical question to answer, and fortunately ALL-RISE provided a fairly definitive answer. The clinical outcomes were virtually indistinguishable between the two strategies, but there were clear workflow advantages with the FFRangio-based approach. Despite strong evidence and guideline support, adoption of physiology has remained disappointingly low, so the hope is that these trial results help jump-start broader use.
Reference
1. Fearon WF, Jeremias A, Witberg G, Al-Lamee R, Cohen DJ, Kaki A, Sharma RP, Yeh RW, Chehab BM, Kim MC, Otake H, Tayal R, Matsuo H, McEntegart M, Patel AK, Sandoval Y, Al-Azizi KM, Dan K, Razzouk L, Fournier S, Popma A, Popma JJ, Zhao D, Redfors B, Madhavan MV, Kornowski R, Leon MB, Kirtane AJ; ALL-RISE Investigators. Angiography-derived fractional flow reserve to guide PCI. N Engl J Med. 2026 Mar 29. doi:10.1056/NEJMoa2600949