Large-Bore Closure Technique Using a Novel Vascular Closure Device
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2026;26(6):7.
David Baning, BS, RT(R)(VI)
Special Procedures Technologist - Electrophysiology, Banner University Medical Center – Phoenix, Phoenix, Arizona
Recovery time from electrophysiology (EP) procedures has traditionally been lengthy and costly. Most ablations require multiple devices to be used simultaneously, necessitating several venous—and sometimes arterial—access sheaths. As a result, patients often require up to 6 hours of monitored recovery before discharge when manual pressure techniques, including figure-of-8 sutures, are used for hemostasis.
In recent years, venous closure devices (VCDs) have helped offset these costs. Although VCDs involve an up-front expense, they can significantly shorten recovery time, allowing for earlier ambulation and discharge. When combined with a reduction in groin complications, many health systems now view VCDs as a fiscally prudent choice.
With the introduction of numerous pulsed field ablation systems, most of which require a sheath larger than 12 French (F), the challenge of closing large-bore vascular access sites has become increasingly important,particularly beyond traditional manual pressure or figure-of-8 techniques. Closure methods capable of effectively managing large-bore access can enhance patient comfort, reduce complication rates, and enable rapid discharge, potentially sparing the facility the cost of an inpatient overnight stay.
Although several devices on the market currently have the ability to close large-bore venous holes, the focus of this methodology is specifically designed for the MYNX Control Venous VCD (Cordis) and is not intended to be a comparison of other devices currently available. This singular device is indicated for sheaths ranging from 6F and 12F without the need for different versions for different sized holes. Bores up to 20F can still be considered on-label provided the large-bore sheath is exchanged for an 11F, 10-cm sheath and the vessel is allowed to rebound for at least 5 minutes. Sheaths should be closed in cranial to caudal order. Preferably, the large-bore sheath is positioned cranially for most orientation and should therefore be closed first. Coagulopathy should be returned to normal via reversal agents or sufficient half-life clearance before MYNX venous closure in accordance with the manufacturer’s recommendations. Light pressure around the 11F sheath may be necessary during this time to prevent oozing from the puncture site.
To use the device (Figure), prepare it according to the manufacturer’s instructions for use. Insert the device into the 11F sheath and engage the sheath catch on the sidearm tubing. Inflate the balloon to its maximum diameter by depressing the locking syringe until the plunger begins to move back slowly, indicating that maximum inflation has been achieved and the overpressure valve has engaged. Lock the balloon in its inflated position using the stopcock.
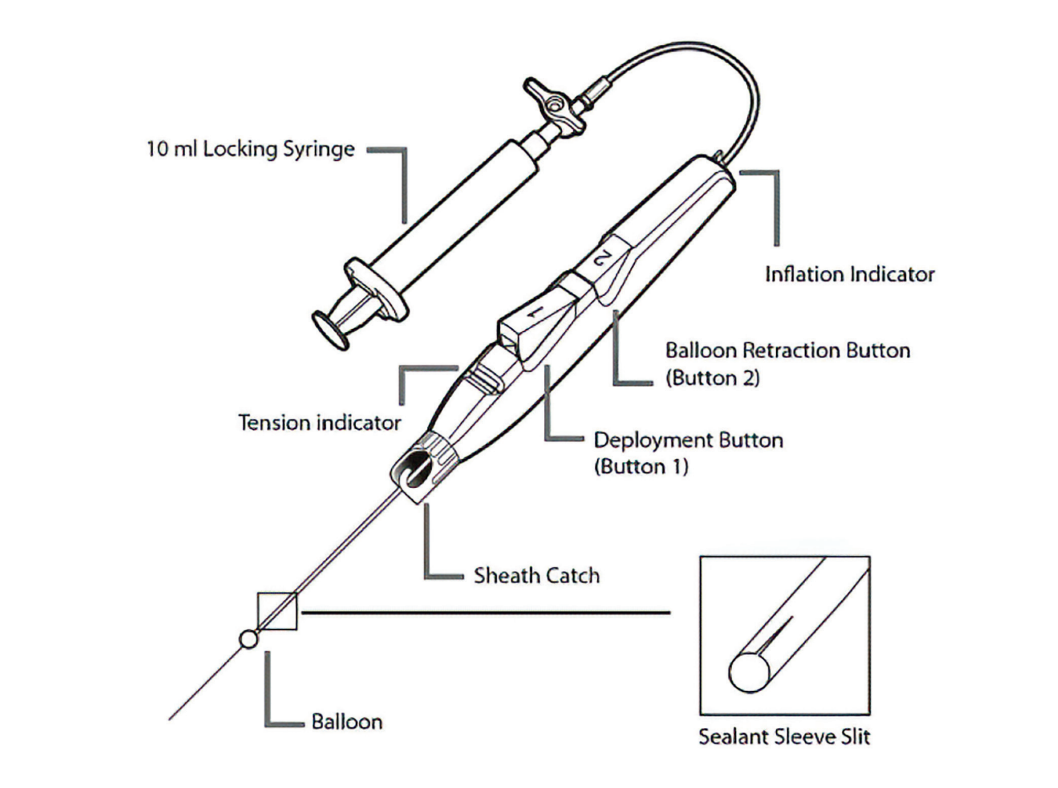
Using the middle and index fingers of the hand closest to the puncture site, place the middle finger just anterior to the puncture site and apply gentle pressure. Elevate the device to approximately 45 degrees and position the index finger immediately posterior to the point where the sheath enters the skin to provide support. If the presence of additional sheaths prevents placement of the index finger in this position, proceed using gentle anterior pressure only.
While maintaining gentle pressure with the middle finger, slowly withdraw the device and sheath together until resistance from the balloon is felt against the middle finger. Continue applying pressure to support the balloon while withdrawing the device and sheath until the tension indicator aligns with the outside marker for deployment. The deployment button (1) will not function until the tension indicator is aligned with the external deployment marker. Gentle pressure at the deployment site may be necessary during the 2-minute deployment period to prevent oozing.
After the 2-minute deployment period has elapsed, lock the 10-mL locking syringe in the fully rearward (locked) position and turn the stopcock to deflate the balloon. Press the balloon retraction button (2) to withdraw the balloon into the device, then remove the deployment device from the body. Apply manual pressure to the site for 2 minutes or until hemostasis is achieved.
Although this technique requires more finesse than closure of smaller-bore size access sites, the benefits may be substantial. These include shorter time to discharge and fewer admissions related to reduced groin complications—2 factors closely associated with higher patient satisfaction scores.
In the era of large-bore access for contemporary EP procedures, thoughtful vascular closure strategies are increasingly important. When performed in accordance with recommended technique and patient selection, novel venous closure devices can facilitate efficient hemostasis, earlier ambulation, and same-day discharge while minimizing groin-related complications. As procedural complexity continues to evolve, optimized large-bore venous closure may enhance patient comfort, reduce complication rates, and enable rapid discharge, potentially sparing the facility the cost of an inpatient overnight stay.
Disclosures: The author has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest, and has no conflicts of interest to report
Related Content