Team-Based Innovation in the EP Lab: Single-Operator Transesophageal Echocardiography During Combined Pulsed Field Ablation and Left Atrial Appendage Closure Procedures
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2026;26(5).
Carolyne Myers, RT(R)
Lead Technologist, Cardiac Catheterization & Electrophysiology Lab, Franciscan Health Michigan City, Michigan City, Indiana
Electrophysiology (EP) is advancing rapidly, and procedural efficiency now depends as much on coordinated team dynamics as on emerging technology. Although single-operator transesophageal echocardiography (TEE) during combined EP and structural heart procedures is widely regarded as impractical—given traditional reliance on a second cardiologist, anesthesiologist, or imaging specialist—Franciscan Health Michigan City has successfully implemented this approach in a community hospital setting.
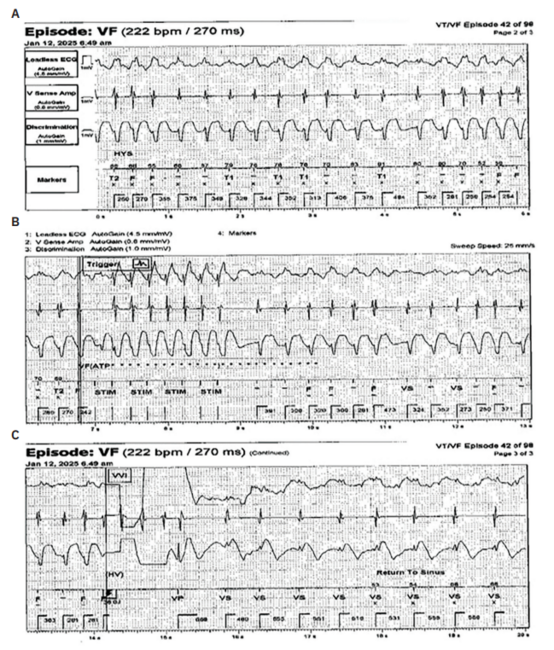
Under the leadership of Naseer Nasser, MD, the cardiac catheterization laboratory team has completed more than 45 combined pulsed field ablation (PFA) and Watchman (Boston Scientific) left atrial appendage closure (LAAC) procedures for the treatment of atrial fibrillation (AF) using a single-operator TEE workflow without intracardiac echocardiography (ICE). In this model, the operating electrophysiologist performs both the interventional and imaging components, with the TEE probe prepared, draped, and manipulated in a sterile fashion by the physician throughout the procedure. Continuous TEE imaging is used for thrombus exclusion, transseptal puncture guidance, pulmonary vein (PV) visualization during PFA, and Watchman sizing and deployment.
A highly coordinated cath lab team supports this workflow, including a lead technologist functioning in a dual role as scrub technologist to maintain sterility and manage device exchanges. This experience demonstrates how physician leadership, coding proficiency, operational discipline, and collaborative teamwork can safely integrate single-operator TEE into complex EP and structural heart interventions while optimizing procedural efficiency and resource utilization in a community hospital setting.
Clinical Benefits of a Combined Procedural Approach
Combining PFA for rhythm control with LAAC device implantation for stroke prevention provides comprehensive AF management in a single session. This integrated approach allows patients to undergo one anesthesia exposure, facilitates earlier discontinuation of oral anticoagulation therapy, and reduces bleeding risk while promoting faster recovery.
Performing both interventions through a single transseptal puncture minimizes catheter manipulation and vascular trauma. Real-time TEE imaging by the operating electrophysiologist enables precise device placement and immediate recognition of potential complications without interoperator delays.
Efficiency and Workflow Optimization
This single-operator model eliminates the need for a second interventionalist or echocardiography specialist to manage the TEE probe. Cath lab technologists and nurses assist with probe setup, anesthesia coordination, and real-time imaging display, allowing the electrophysiologist to transition seamlessly between imaging and intervention.
Integrating imaging and therapy shortens total procedure time by approximately 45 to 60 minutes per case, improving patient safety and increasing procedural efficiency. The resulting workflow optimization allows completion of up to 2 additional procedures per day. With Medicare reimbursement averaging $30,000 to $35,000 per Watchman case, this represents an estimated $60,000 to $70,000 in additional daily capacity—an important operational and economic advantage for community hospitals.
Sterile TEE Preparation and Continuous Imaging Model
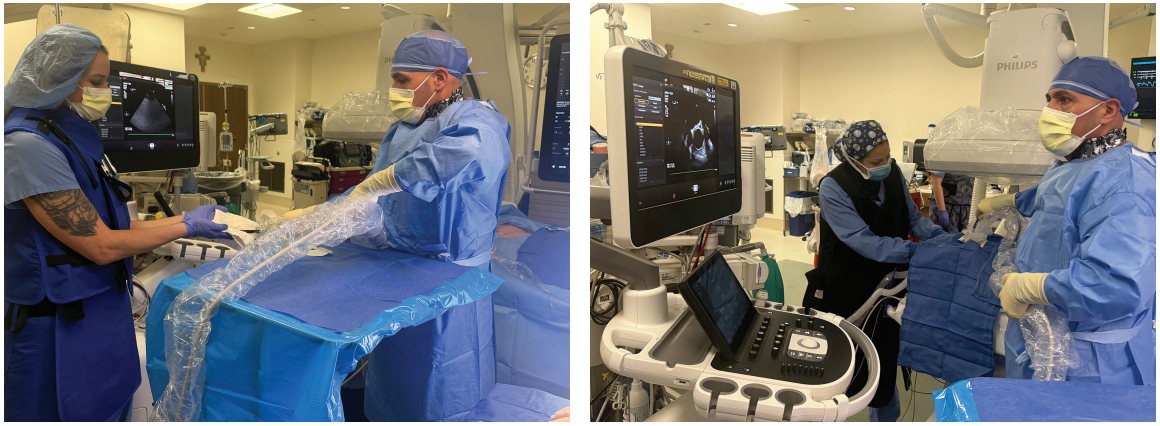
After induction of general anesthesia, the operating physician prepares and drapes the TEE probe with a sterile cover and applies sterile draping to the patient’s face. This allows the probe to remain within the sterile field for the entire procedure.
Unlike conventional workflows in which TEE is used intermittently or managed by a second operator, the probe remains continuously in place and accessible to the physician without breaking sterility. This enables uninterrupted imaging throughout transseptal access, PFA, and Watchman deployment. ICE is not used at any stage; all imaging guidance is provided exclusively by TEE and fluoroscopy.
Integrated Procedural Workflow
Preprocedural Imaging
TEE is used to exclude thrombus in the LA and LAA, assess LAA anatomy, and obtain baseline views for transseptal puncture. When not actively manipulated, the probe is maintained in a neutral mid-esophageal position.
TEE-Guided Transseptal Access (Operator Transition #1)
The operator manipulates the TEE probe to obtain bicaval and short-axis views. After confirming tenting and puncture trajectory, the physician briefly transitions to the transseptal needle and sheath, then returns to TEE to confirm LA access and sheath positioning.
PFA (Operator Transition #2)
During PFA, the operator intermittently adjusts the TEE probe to confirm PV engagement and LA anatomy while performing ablation. Continuous sterile access to the probe allows real-time imaging without workflow interruption.
Watchman Sizing and Deployment (Operator Transition #3)
TEE is used for LAA measurement, sheath alignment, device compression and seal assessment, and stability confirmation. Standard imaging angles (0°, 45°, 90°, 135°) are obtained. The operator alternates briefly between probe manipulation and sterile-covered device controls to confirm final placement and exclude pericardial effusion.
Across the entire procedure, the workflow typically involves 3 predictable operator transitions between imaging and intervention, integrated into a smooth procedural rhythm.
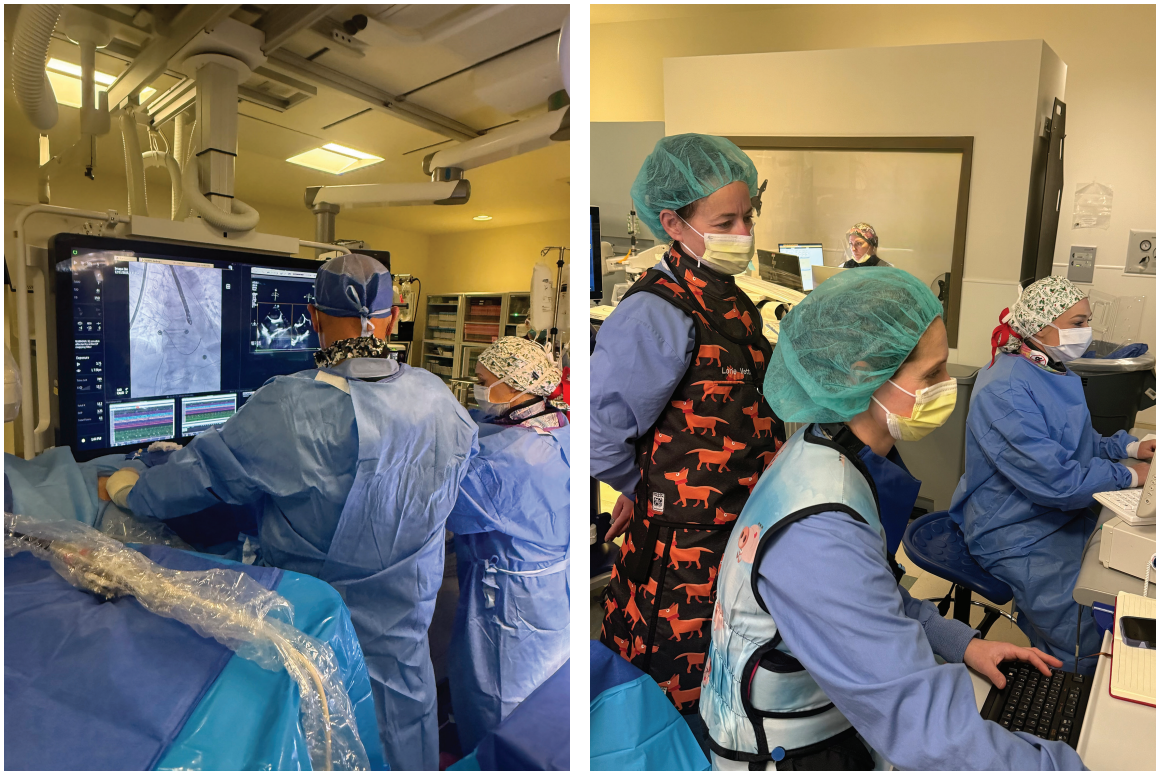
Cath Lab Team Integration
The success of single-operator TEE depends on coordinated team execution:
- Physician: Prepares and drapes the TEE probe, performs continuous imaging, PFA, and Watchman deployment.
- Lead technologist (also scrub technologist): Maintains sterile field, prepares devices, manages sheath exchanges, and supports procedural flow at the table.
- Circulating nurse: Supports probe stabilization when needed, coordinates room workflow, and interfaces with anesthesia.
- Anesthesia team: Maintains airway control and hemodynamic stability during prolonged TEE manipulation.
This integrated staffing model eliminates the need for a second interventionalist or imaging specialist while maintaining procedural safety and efficiency.
Clinical and Professional Advantages
Comprehensive AF Management
Patients receive rhythm control via PFA and stroke prevention via Watchman implantation in a single session, minimizing cumulative procedural risk and recovery time.
Enhanced Procedural Safety
Key safety features include a single transseptal puncture, continuous real-time imaging, immediate detection of complications, and reduced catheter manipulation.
Earlier Anticoagulation Discontinuation
Appropriate patients can discontinue oral anticoagulants earlier, reducing bleeding risk and long-term medication burden.
Professional Autonomy and Skill Integration
Electrophysiologists trained in TEE achieve greater procedural control by integrating imaging and therapy to enhance anatomical precision. At Franciscan Health Michigan City, cath lab nurses and technologists function as extensions of the operator, managing probe setup, hemodynamic monitoring, and device preparation. This role flexibility improves team performance and contributes to higher job satisfaction.
Team-Driven Culture of Innovation
Beyond reimbursement accuracy, the single-operator workflow shortens procedure time, reduces handoffs, and illustrates how coordinated teamwork can achieve both clinical and operational excellence. The success of these cases reflects a unified culture built on trust and adaptability. Nurses, technologists, and anesthesia staff anticipate procedural milestones, maintain imaging quality, and uphold safety standards at every stage.
This collaborative approach enables a community hospital to deliver EP and structural heart care that rivals that of large academic centers, while maintaining same-day discharge consistency and high patient satisfaction. Ultimately, this team-based model demonstrates that community hospitals can achieve tertiary-level innovation efficiently and sustainably.
Conclusion
The single-operator TEE workflow at Franciscan Health Michigan City demonstrates that innovation is most effective—and not cumbersome—when it is intentionally designed and supported by cohesive teamwork. By maintaining continuous sterile TEE imaging, eliminating the need for ICE, and enabling the operator to manipulate the probe throughout the procedure, the team delivers a streamlined, safe, and reproducible model of care. In addition, by combining PFA and LAAC device implantation within a single anesthesia session and aligning practice with CMS coding standards, the program shows that community hospitals can achieve tertiary-level outcomes efficiently and sustainably. Experience from more than 45 successful cases provides a practical model for EP labs seeking to enhance safety, efficiency, and value-based care through collaboration and cross-disciplinary expertise.
Disclosures: Carolyne Myers, RT(R) has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest, and has no disclosures to report.
Related Content