

Beneficence and Nonmaleficence in Cancer Pain Measurement: A Bioethical Framework for Analyzing Quality Measures
The predominant US health care quality measure development and endorsement processes, as summarized in the Center for Medicare and Medicaid Services (CMS) Blueprint, define various well-accepted criteria for evaluating measures. In this blog series, we will view quality measure evaluation through the lens of bioethical principles, using oncology measures as examples. While bioethical principles are fundamental to all health care practices, they are not formally prioritized during quality measure development. This first blog in the series will apply the principles of beneficence and nonmaleficence to analyze the Oncology: Medical and Radiation Plan of Care for Pain measure, developed by the American Society of Clinical Oncology (ASCO). Future blogs in the series will explore the principles of autonomy and justice.
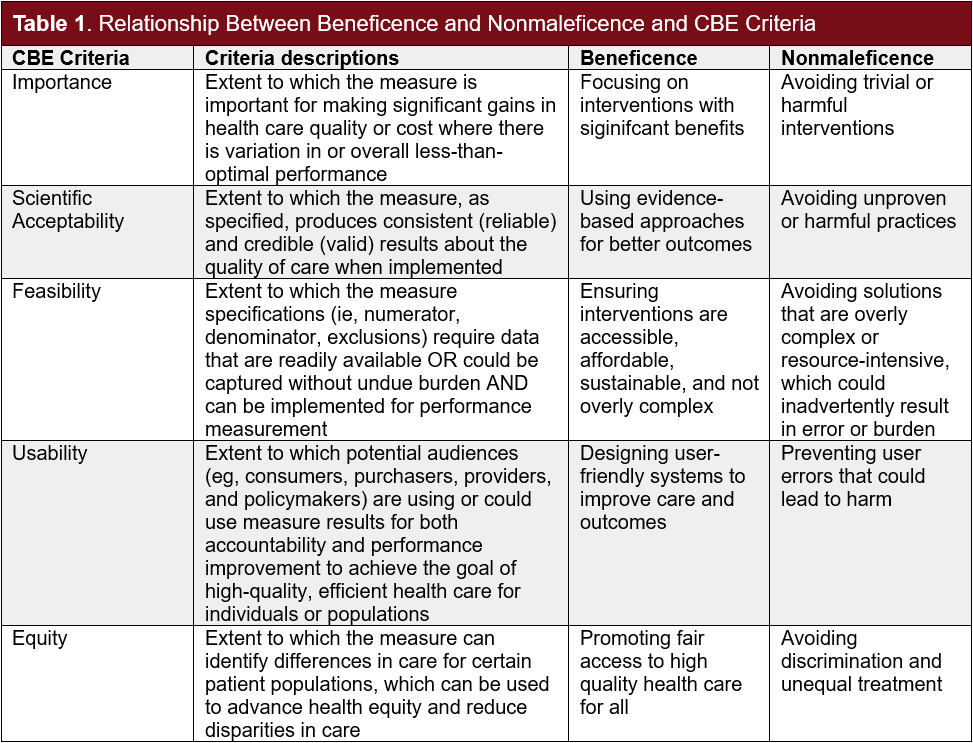
Bioethicists Beauchamp and Childress describe the principles of beneficence, nonmaleficence, autonomy, and justice to collectively form a framework for analyzing ethical issues in health care. The current federal Consensus-Based Entity (CBE), the Partnership for Quality Measurement (PQM), is responsible for endorsing quality measures and applies specific criteria of importance, scientific acceptability, feasibility, usability, and equity to evaluate measures. These criteria overlap somewhat with bioethical principles, such as beneficence and nonmaleficence, particularly in considering unintended consequences of measures (Table 1). Although the PQM’s endorsement criteria implicitly touch on components of the four bioethical principles, an intentional ethical perspective would provide insight into how quality measures serve public health, enhance quality of care, and improve patient outcomes.
Beneficence and Nonmaleficence
The principles of beneficence and nonmaleficence work in common to promote good and prevent harm. Beneficence refers to the obligation to act for the benefit of others, promote good, and minimize or prevent harm. This includes acting in the best interest of a patient by providing care that maximizes the chances of maintaining or improving the health of the patient. Health care professionals and organizations are responsible for acting in the best interest of the patient and preventing harm, as reflected in the adage “first, do no harm.” Nonmaleficence complements beneficence by emphasizing the obligation not to inflict harm intentionally and to prevent harm from occurring. It includes avoiding actions that are known to cause harm or could potentially cause harm, weighing all risks and benefits prior to any medical intervention, and avoiding any negligence or malpractice.
Quality measures influence patient outcomes, as well as health care structures and processes, by helping clinicians apply best practices in the delivery of care, and then assess their results. Through mechanisms such as internal benchmarking and performance evaluation, public reporting, and reimbursement/payment, clinicians are incentivized to continuously improve their quality of care. Incorporating both beneficence and nonmaleficence into quality measure evaluation can further help clinicians to assess whether their care maximizes benefits and minimizes harm for the patient. This includes identifying potential adverse events, such as side effects, medical errors, and readmissions.
Likewise, quality measures are interwoven with the practice of health care, as they are evaluated both before and after implementation for the possibility of unintended consequences. These can include exacerbating disparities, causing unintended influence on clinician decision-making, and shifting focus such that improving quality in one area might lead to quality reduction in another area. Adding the lenses of beneficence and nonmaleficence to quality measure analysis can aid in anticipating additional unintended consequences by identifying where harm can be avoided or removed for the specific patient population in need and across broader patient populations.
Oncology: Medical and Radiation Plan of Care for Pain Measure
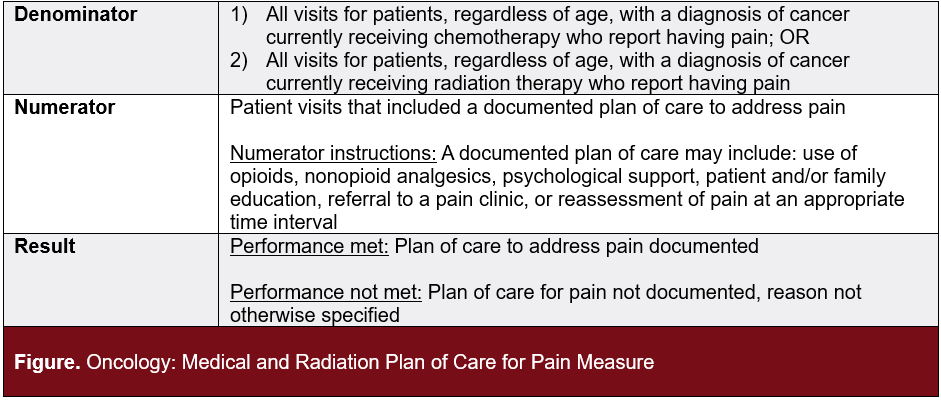
The Oncology: Medical and Radiation Plan of Care for Pain Measure evaluates the care of cancer patients undergoing chemotherapy or radiation therapy who report experiencing pain, by measuring the proportion that have a comprehensive pain management plan (Figure). Pain is a prevalent symptom in cancer, affecting 30% to 50% of oncology patients, and can severely impact quality of life. Moreover, evidence suggests that better pain management can lead to improved outcomes for cancer patients, heightening the importance of this measure. Proper assessment and management of pain are essential, as unmanaged pain may negatively impact daily activities, motivations, and interactions with others. This measure underscores the importance of personalized care plans that incorporate both medical and non-medical strategies to effectively alleviate pain, considering each patient's unique situation and preferences.
Measure Analysis: Pain Management and Patient Care
Key criteria needed to evaluate this quality measure through the lenses of beneficence and nonmaleficence include whether the measure is in the patient’s best interests, maximizes benefits, and prevents harm. Assessing patient-reported pain levels at every eligible visit fosters a care environment that prioritizes both quality of life and quality of care. This approach effectively addresses the best interests of the patient and maximizes the benefits of their care, as it reflects a consistent commitment to treating their holistic needs related to their cancer diagnosis.
Additionally, integrating pain management practices into oncology treatment plans is crucial for preventing and monitoring harm caused by cancer and its treatment. Approaches to case management vary significantly based on cancer type, stage, and patient goals, such as those for early-stage patients undergoing curative treatment vs late-stage patients in end-of-life care. Effective pain management can reduce suffering and enhance a patient’s tolerance to oncology treatment, thereby working to prevent harm.
Appropriate pain management also acts as a risk minimization strategy by serving as a preventive measure against potential complications, such as reducing the risks of overmedication, and mitigating negative mental health outcomes associated with persistent pain. This pain management measure not only helps identify opportunities for interventions that enhance patient health outcomes and quality of life but also aids in alleviating some of the challenges that oncologists encounter in managing pain.
According to ASCO, moderate-to-severe cancer pain can often be effectively managed with available medications, including opioids. However, the use of opioids presents significant challenges. Amid the ongoing opioid epidemic, clinicians face the complex task of balancing the need to prevent opioid misuse with the imperative to deliver optimal, timely, and cost-effective treatments.
This vigilant approach also allows for the early identification and management of emerging mental health concerns, such as anxiety and depression. Research indicates that approximately 30% to 50% of oncology patients experience psychiatric comorbidities, such as depression or anxiety disorders. In cancer patients, where pain is highly prevalent, psychiatric disorders are frequently observed and can significantly impact adherence to treatment regimens and quality of life.
Opportunities for Enhancement
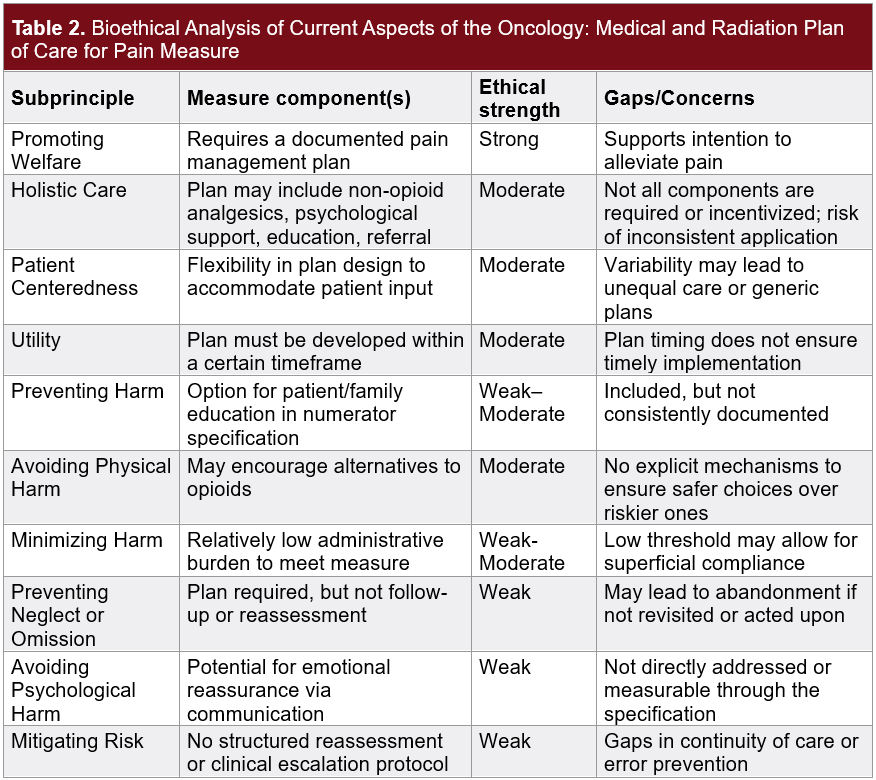
To effectively identify opportunities to improve the Oncology Plan of Care for Pain measure, it is important to analyze how its components align with the subprinciples of beneficence and nonmaleficence, as well as to identify any existing gaps (Table 2).
In evaluating the measure, there are opportunities for enhancement through the introduction of additional reporting mechanisms to better align with the principles of beneficence and nonmaleficence. For example, clinicians could be required to report on the implementation of structured reassessment and clinical escalation protocols, surpassing the current requirement of merely documenting a plan for pain. By focusing on these protocols, which would ensure continuous engagement and adjustment of care plans, clinicians could achieve more meaningful improvements in patient outcomes and satisfaction, thereby ensuring that any additional efforts translate into real benefits for the care needs of each patient.
Furthermore, follow-up metrics could be implemented to track the success and adherence to these protocols, facilitating ongoing evaluation and refinement. Additional reporting mechanisms could include enhanced documentation and incentives for holistic care. However, it is crucial to ensure that such measures do not become mere “checkbox” activities without meaningful impact. Instead, metrics should focus on whether patient perception of their management goals are being understood and incorporated, as well as whether treatments effectively help with pain management. Assessing the implementation of holistic care components can help clinicians gain insights into overall patterns of care and patient needs, ultimately enhancing the quality of care they deliver.
Conclusion
This analysis of the Oncology: Medical and Radiation Plan of Care for Pain measure illustrates how two principles of a bioethical framework can be applied to assess quality measures, particularly through the lenses of beneficence and nonmaleficence. These principles highlight the importance of promoting welfare, patient-centeredness, holistic care, harm prevention and reduction, and risk management within quality measurement. By integrating an ethical framework into quality measure analysis, measure developers and implementers can enhance the effectiveness of quality measures in addressing health outcomes and meeting patient needs.
 About Nandita Ammanamanchi, BA
About Nandita Ammanamanchi, BA
Nandita Ammanamanchi is a senior analyst on the Market Access team at Real Chemistry, where she applies her expertise in health care research, health equity, and data analytics to inform strategic decision-making across therapeutic areas. She is currently pursuing a Master of Science in Bioethics at Harvard Medical School, with a capstone focus on narrative ethics in high-intensity care settings. Nandita brings a multidisciplinary lens to complex challenges in health care policy and access, and is passionate about leveraging data and research to drive equitable health outcomes and shape the future of health care.
 About Rachel Delinger, MPH
About Rachel Delinger, MPH
Rachel Delinger is a senior manager on the Real Chemistry Market Access team. She is data-driven with expertise in outcomes research and real-world evidence generation, and works across functions to inform market access strategy, serve as a quantitative methodologist, and supports evidence generation efforts that align with evolving access landscapes. She brings a strong analytical foundation to market access strategy, bridging clinical, economic, and patient-centered perspectives.

About David Blaisdell, BA
David Blaisdell, a senior director at Real Chemistry, leads and manages client projects, providing insight and subject matter expertise, particularly on quality landscape analyses and measure gap identification. David has led and contributed to projects focused on oncology quality measurement to identify key gaps in measures used in accountability programs and opportunities for measure development. Through this experience, David helps clients navigate measurement and value-based payments and define strategies for success.
 About Tom Valuck, MD, JD
About Tom Valuck, MD, JD
Tom Valuck, MD, JD, is the editor of Quality Outlook. He formerly led the Market Access Value-Based Care discipline for the Market Access team at Real Chemistry. The team uses research and strategic advisory services to help our clients improve health and health care by assessing, responding to, and shaping the value landscape.
Tom is a thought leader on health care system transformation, focused on achieving better health and health care outcomes at a lower cost. Tom’s work includes facilitating the exploration of next-generation measurement and accountability models for health care delivery systems. He also helps clients develop strategies to achieve success within the value-based marketplace.



