


Bullet Captured From the Right Atrium Using the Protrieve Sheath, Preventing Central Embolization
© 2023 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Vascular Disease Management or HMP Global, their employees, and affiliates.
VASCULAR DISEASE MANAGEMENT 2023;29(8):E146-E149
Abstract
A 21-year-old man presented as a Level 1 trauma following a gunshot wound to the left lower quadrant of the abdomen. A bullet was first identified on radiographic imaging but was not found during exploratory laparotomy. Subsequent chest radiographs and computed tomography demonstrated the bullet to be at the junction of the right atrium and inferior vena cava with slight variation of positioning, suggesting mobility and an intravascular location. Following interventional radiology consultation, the bullet was determined to be intravascular by fluoroscopy. The migratory bullet was extracted safely using a snare and a Protrieve sheath (Inari Medical), a novel device designed to trap thromboemboli in the inferior vena cava during mechanical thrombectomy procedures.
Introduction

Extravasation and embolization of a bullet or ballistic fragments following a gunshot wound may lead to myriad complications if it enters a large vein and travels to the right cardiac chambers and pulmonary arteries.1 Most interventions to retrieve a bullet embolism from the right circulation are operative; however, in some circumstances, endovascular retrievals are an appropriate, less invasive option.1 This case demonstrates the first known use of the new Protrieve sheath (Inari Medical) (Figure 1) to facilitate the safe removal of a bullet from the right atrial junction with the inferior vena cava (IVC) of a Level 1 trauma patient with a gunshot wound. The Protrieve sheath is indicated for the removal of peripheral thromboemboli in cases of complex deep vein thrombosis (DVT). When deployed, the Protrieve sheath funnel has a diameter of 33.5 mm, which provides atraumatic caval wall apposition and the ability to trap emboli during a procedure. In this case, the unique use of the Protrieve sheath enabled extraction of the bullet while preventing further proximal migration to the right heart and pulmonary arteries.
Case Report
Medical History
A 21-year-old man presented as a Level 1 trauma patient following a gunshot wound to the lower left quadrant of the abdomen.
Investigations
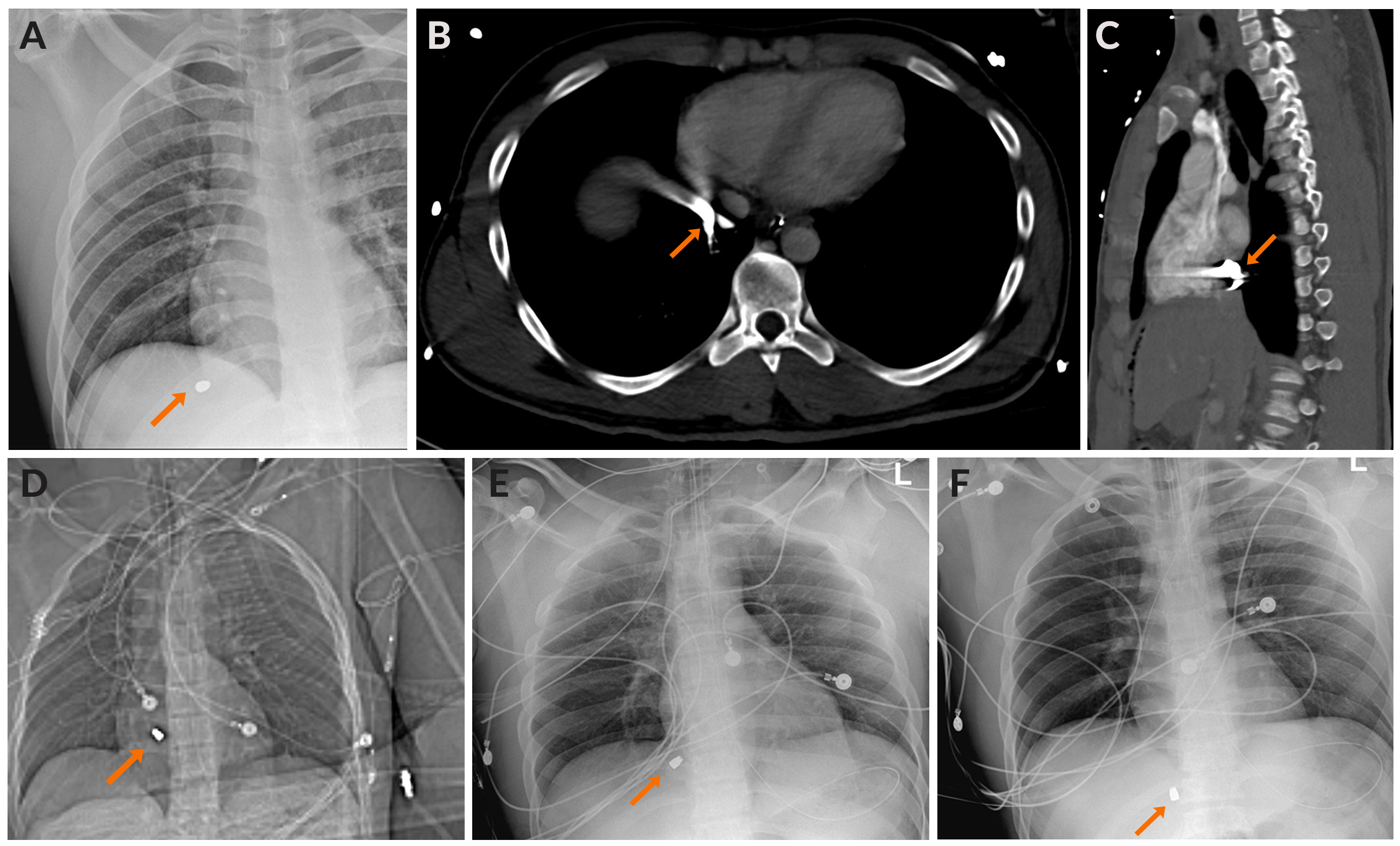
An extended focused assessment with sonography for trauma was positive for intra-abdominal fluid, likely blood products. Radiographs of the chest, abdomen, and pelvis were performed, and a bullet was noted in the high right upper quadrant of the abdomen under the right hemidiaphragm (Figure 2A). No exit wound was seen on physical exam.
The patient was taken to the operating room by the trauma surgical team, where an emergency exploratory laparotomy was performed. The abdomen was packed to achieve hemostasis. A small bowel injury was noted, and a small-bowel resection as well as a reanastomosis were performed. Of note, during surgery there was no significant hematoma seen surrounding the IVC to suggest injury. The bullet was not found during the exploratory laparotomy. Abdominal closure was not performed at that time.
The patient was brought to the computed tomography (CT) scan room for a CT of the chest, abdomen, and pelvis following trauma and urogram protocols. The scan was notable for a metallic bullet at the inferior cavoatrial junction (ICAJ). Subsequent chest radiographs demonstrated slight variation of the bullet, suggesting mobility and an intravascular location. The bullet projected over the upper IVC in multiple locations, also indicating mobility (Figure 2B-F).
Management
Interventional radiology (IR) was consulted and given the CT and radiographic images; an intravascular location was highly suspected. Plans were made for fluoroscopic-guided intravascular foreign body retrieval using a Protrieve sheath to provide a conduit for a snare device and to prevent central migration of the bullet toward the pulmonary arteries during the procedure.
The patient was brought into the IR suite and placed supine on the fluoroscopy table. The right side of the neck and upper chest and the bilateral groins were prepped and draped in usual sterile fashion.
Initial fluoroscopic images confirmed the bullet to be at the level of the ICAJ. It did not appear to be attached to the vascular or cardiac walls, as it moved freely from the right atrium to the ICAJ with cardiac and respiratory variation.
Following the administration of a local anesthetic, the right internal jugular (IJ) vein was accessed utilizing micropuncture technique followed by placement of a 0.035" Amplatz wire into the IVC.
Next, the venotomy was dilated over the Amplatz wire, followed by placement of a 20F Protrieve sheath. The sheath was advanced to the right atrium, and the Protrieve funnel was deployed under fluoroscopic guidance to preclude migration of the bullet through the tricuspid valve. The sheath dilator was then retracted and removed. It was noted that the patient did not experience any cardiac ectopy and remained in normal sinus rhythm following deployment of the Protrieve funnel.
Subsequently, an 18-30 mm EN Snare Endovascular Snare System (Merit Medical) was assembled and advanced through the Protrieve sheath. Under fluoroscopy, the bullet was seen tumbling in the IVC at the ICAJ as the snare was utilized to capture it (Figure 3A, Video 1). The bullet was retracted through the mesh funnel and into the plastic sheath tip of the Protrieve sheath (Figure 3B, Video 2). The sheath was then retracted over the wire while tension was held on the bullet with the snare (Video 3). Fluoroscopy confirmed that the bullet did not move from the sheath tip and the bullet was then removed along with the sheath (Figure 3C-D). The sheath dilator was replaced into the venotomy site.
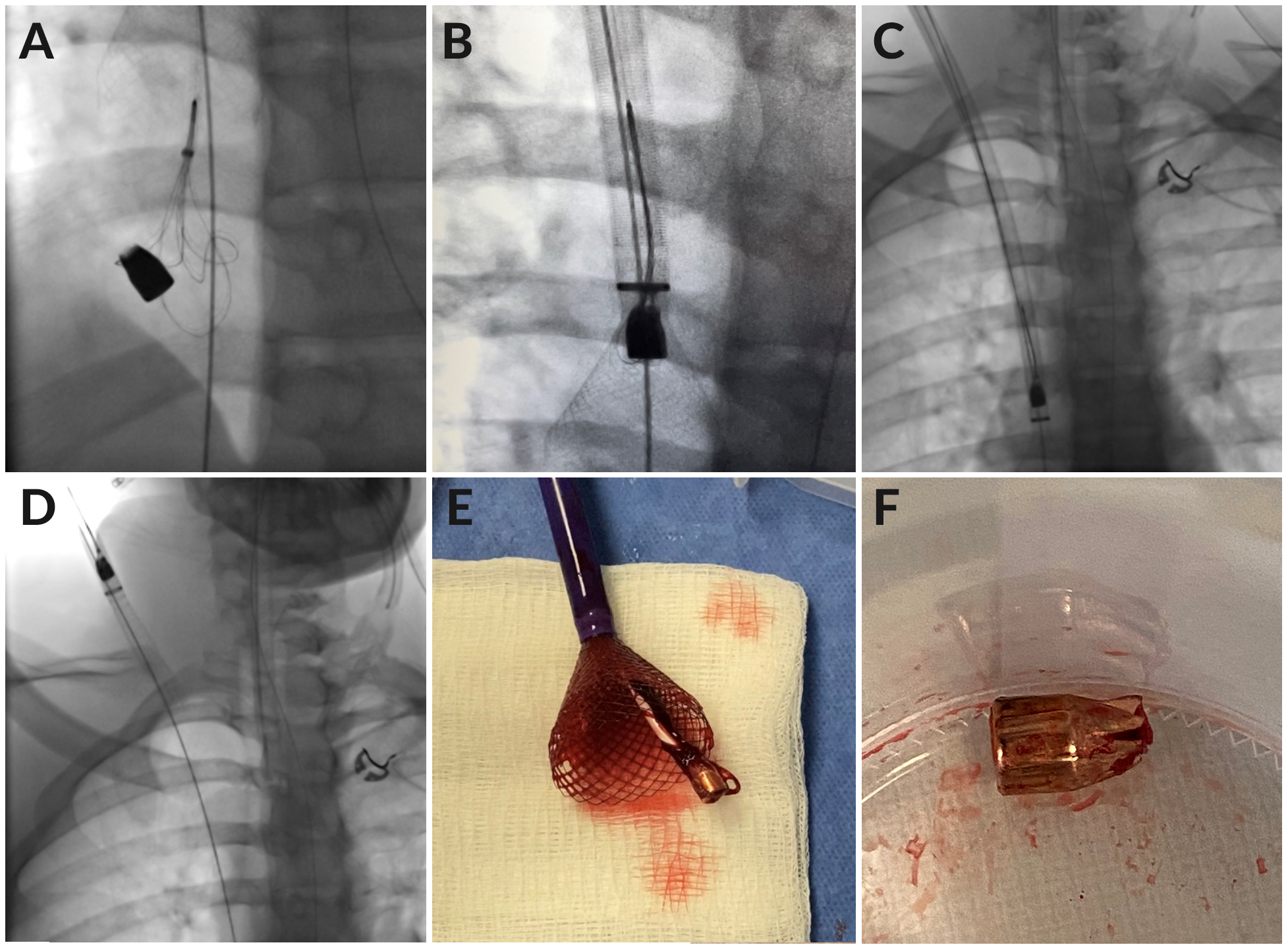
Visual inspection of the snare and sheath tip verified that the bullet had been successfully removed (Figure 3E). It was placed in a specimen container (Figure 3F) and given to the trauma team for forensic processing.
Fluoroscopic images of the chest were obtained and demonstrated no persistent metallic projectile within the chest. Transthoracic sonography showed no evidence of pericardial fluid or hemorrhage. At this point, the procedure was deemed complete. The wire and sheath dilator were removed and hemostasis was achieved with manual pressure. Skin glue was applied to the venotomy site.
Total procedure time from needle puncture to sheath removal was 25 minutes, including 12.6 minutes of fluoroscopy.
The patient tolerated the procedure well and proceeded to the operating room where the trauma surgery team performed a second-look laparotomy and abdominal closure. No additional or significant injuries were found.
The patient was transferred to the trauma intensive care unit (ICU) for further critical care and monitoring. He was extubated later the same day, weaned off oxygen, then transferred out of the trauma ICU 2 days later. He was discharged home 6 days after presentation, 5 days after bullet removal.
Discussion
Most bullets or bullet fragments located in the vasculature enter through the venous system, with most vein entries occurring in the IVC (25%).1 The high IVC entry rate is likely a result of the comparatively large size of this vessel. The same study reports that, once in the vascular system, 77% of ballistic emboli in the right circulation migrate to either the heart or the pulmonary arteries.1 Though complications from such emboli are infrequent, the chance for arrhythmia, infection, and thrombosis remain.1 Therefore, the minimally invasive endovascular capture and removal of venous ballistic emboli from the IVC is warranted, particularly for trauma patients who are already undergoing abdominal surgery.
Both early experience with the Protrieve device at this institution and successes reported in the published literature2-4 prompted consideration of its creative use for this case. Shin et al described using the Protrieve sheath to provide embolic protection in 2 patients undergoing malignant IVC thrombectomy.2 Amin related a complex mechanical thrombectomy procedure using the Protrieve sheath in which IVC thrombus and a thrombosed filter were removed effectively with an intraprocedural embolus trapped by the device funnel and removed without complication.3 Chick and Shaikh demonstrated the effective use of the Protrieve device to simplify complex DVT thrombectomy procedures; in the first of 2 cases, a single IJ access site was used to extract thrombus extending from the intrahepatic IVC to the left renal vein, the infrarenal IVC, and the right common iliac vein. In the second case involving extensive, chronic thrombus throughout the right iliocaval and iliofemoral venous segments and left renal vein, the chronic thrombus was removed rapidly while avoiding embolic complications.4
In the case described here, it was moderately difficult to determine the location of the bullet on CT scan due to imaging artifacts. However, it had been seen in multiple locations overlying the upper IVC and right atrium, suggesting an intravascular location that would allow mobility. Given the location, the operators were challenged to deploy the Protrieve sheath at a level that would prevent them from accidentally causing central embolization of the bullet. Although there was an initial preference to place the Protrieve funnel closer to the right atrial and IVC junction, it was ultimately deployed at the level of the mid-right atrium, which proved successful at preventing bullet migration into the right ventricle.
Once extracted, visual examination of the bullet determined it to be an intact projectile, with no suspected fragments remaining in the patient. Fluoroscopic examination of the chest and abdomen showed no other retained metallic foreign body.
This creative application of the Protrieve sheath blocked further migration of the bullet to the heart or pulmonary arteries and averted associated complications for this patient as well as a more challenging potential retrieval from the right ventricle or pulmonary arteries. He was seen in the trauma clinic 2 weeks after discharge and was noted to be progressing appropriately with recovered bowel function, stable vital signs and hemoglobin, as well as no signs or symptoms of ongoing bleeding.
Conclusion
Under urgent conditions, IR completed the effective, rapid removal of a migratory bullet from a patient with a gunshot wound to the abdomen while preventing further intraprocedural embolization with the Protrieve sheath. Futures studies are needed to validate the effectiveness of the device in other applications. n
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no financial relationships or conflicts of interest regarding the content herein.
Manuscript accepted July 10, 2023.
Address for correspondence: William Terrill, MD, Allegheny Clinic Radiology, Allegheny General Hospital, 320 E. North Ave., Pittsburgh, PA 15212. Email: William.Terrill@AHN.org
Related Articles
Video Commentary: Dodging a Bullet
Simplifying Complex DVT Thrombectomy Cases With the New Protrieve Sheath
REFERENCES
1. Kuo AH, Gregorat AE, Restrepo CS, Vinu-Nair S. Systematic review of civilian intravascular ballistic embolism reports during the last 30 years. J Vasc Surg. 2019;70(1):298-306. doi:10.1016/j.jvs.2019.02.004
2. Shin DS, Abad-Santos M, Kuyumcu G, et al. Embolic protection during malignant inferior vena caval thrombectomy using the Protrieve sheath. Cardiovasc Intervent Radiol. 2023;46(4):535-537. doi:10.1007/s00270-023-03366-5
3. Amin V. Use of the Protrieve sheath to trap embolizing thrombus during a complex mechanical thrombectomy procedure with a thrombosed IVC filter. J Vasc Surg Cases Innov Tech. 2023;9(2):101122. doi:10.1016/j.jvscit.2023.101122
4. Chick JFB, Shaikh A. Simplifying complex DVT thrombectomy cases with the new Protrieve sheath. Vascular Disease Management. 2023;29(1).
