


The Clinical Utility of the Zilver Vena Venous Self-Expanding Stent to Treat Symptomatic, Post-thrombotic Ileocaval Venous Obstruction
Abstract
Chronic venous disease of the lower extremities has varied etiology, and several epidemiologic studies have shown prevalence ranging from 50% to 70% of the general population. Patients with severe symptoms or failed conservative management can benefit from endovascular treatment with stent placement. In this case study, we report our experience in treating patients with chronic venous disease using the Zilver Vena venous self-expanding stent (Cook Medical), a Nitinol (nickel titanium) alloy, open-cell design, dedicated venous stent. Prospective and retrospective studies have demonstrated favorable clinical outcomes with good patency rates. At the Vascular Interventional Advances (VIVA) Conference in October 2021, late-breaking clinical trials presented 3-year outcomes from the VIVO clinical study, which showed very high patency rates (90.3 ± 2.2%) for Zilver Vena stents by ultrasound at 3 years. Also noted were freedom from clinically driven reinterventions at 92.6 ± 2% and freedom from reinterventions at 82.9 ± 2.6%. Based on our experience and published clinical research, endovascular treatment of chronic venous disease with the Zilver Vena Venous Self-Expanding Stent is associated with improved outcomes and symptom alleviation.
VASCULAR DISEASE MANAGEMENT 2022;19(1):E14-E18
Key words: chronic venous disease, endovascular venous intervention, May-Thurner syndrome, venous stent
Introduction
Chronic venous disease of the lower extremities has varied etiology, including thrombotic occlusion, external compression, inadequate muscle pump function, and reflux disease due to incompetent valves. Longstanding venous disease leads to venous hypertension, increased capillary permeability, edema, and skin changes.1 Several epidemiologic studies have shown a prevalence from 50% to 70% in the general population.2-4 Most patients present with minor symptoms such as telangiectasias, reticular veins, and varicose veins, and a small but significant number present with severe symptoms such as pelvic congestion syndrome (PCS), chronic venous stasis dermatitis, and venous ulcers.5
When conservative treatment strategy fails, endovascular treatment with stent placement is prudent for central venous obstruction.5-7 Various venous stents are marketed with different stent designs. The Zilver Vena venous self-expanding stent (Cook Medical) is an open-cell design, self-expanding venous stent that was FDA approved in the United States in October 2020. In this case report, we present our experience using the Zilver Vena stent to treat 2 symptomatic patients with post-thrombotic iliac veno-occlusive disease.
Case I
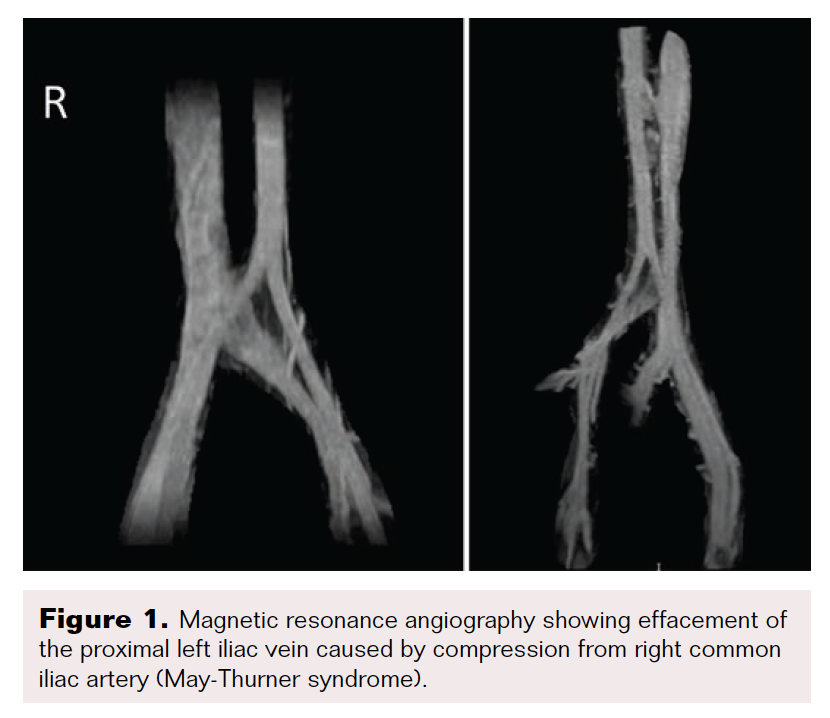
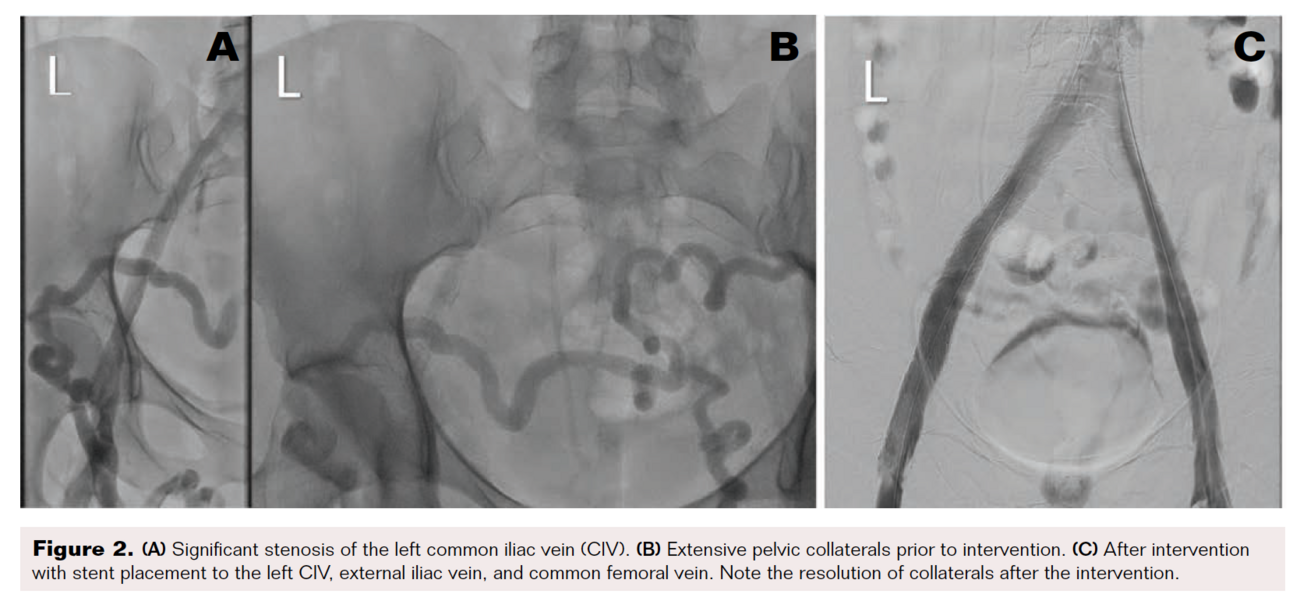
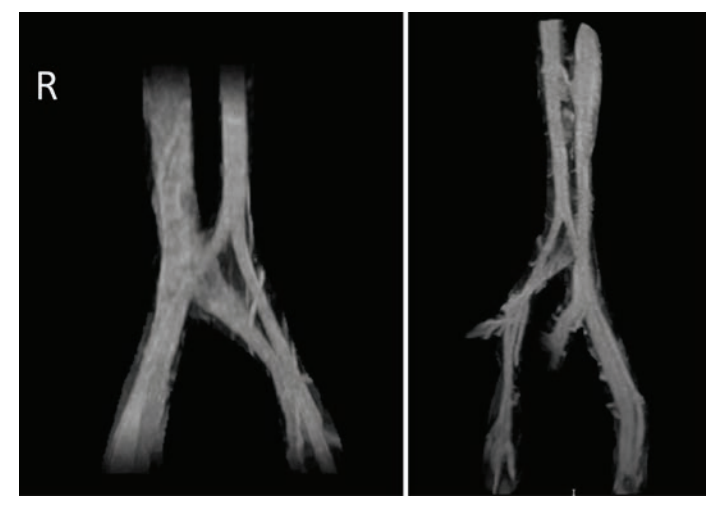
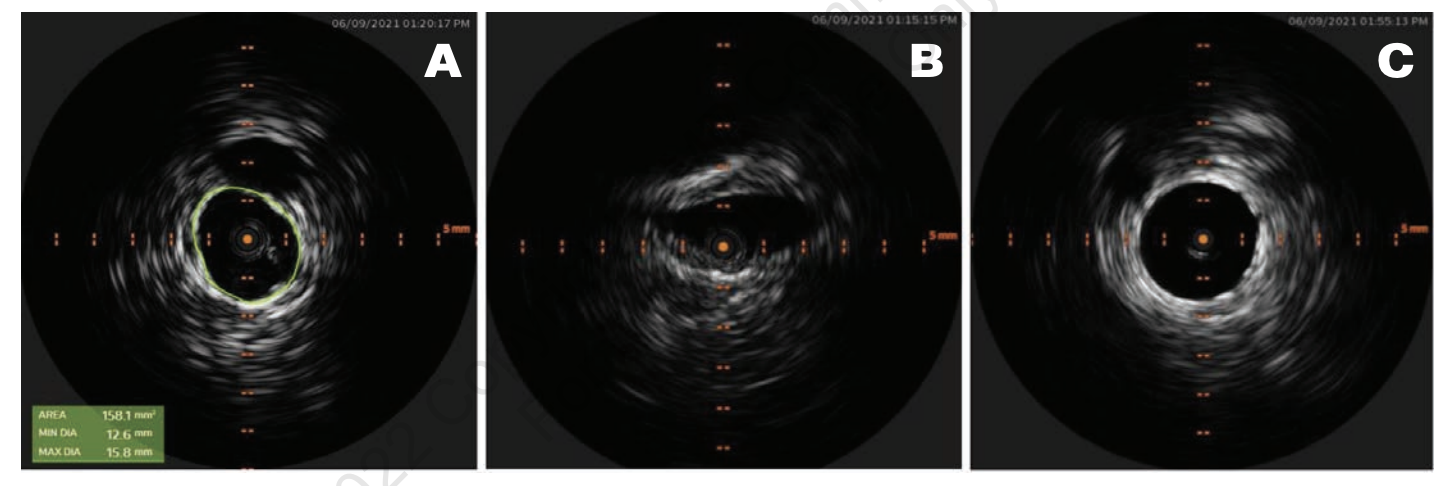
A 39-year-old woman with a history of recurrent deep vein thrombosis (DVT), pulmonary embolism (PE), and protein C deficiency on oral anticoagulation (OAC) was referred to our clinic for chronic bilateral lower extremity swelling, redness, and varicose veins. She was initially diagnosed with DVT and PE in 2003, for which she was on OAC with warfarin. Her warfarin was discontinued 6 months later, and she did well until 2018 when she had a recurrent DVT and PE following an 8-hour plane ride. At that time, a workup revealed a protein C deficiency, and she had been on OAC with apixaban 5 mg twice daily ever since. Her leg swelling, redness, and pain became severe a few weeks before presentation, which was aggravated by standing for long periods. She also complained of frequent dyspareunia and periodic pelvic pain. On physical examination, she was noted to have varicose veins on both legs, 2+ pedal edema up to the level of the thigh, and redness in both legs. We ordered a venous ultrasound (US) of the lower extremity to assess for reflux and to rule out DVT. We ordered a magnetic resonance angiography (MRA) with the suspicion of a central venous obstruction and PCS. Her US showed a chronic, nonocclusive thrombus in the left common femoral vein (CFV). Her MRA showed effacement of the proximal left iliac vein by the right common iliac artery, which was consistent with May-Thurner syndrome (Figure 1). In addition, the MRA showed varices of the anterior pelvic wall. We performed venography with intravascular US (IVUS)-guided percutaneous transluminal angioplasty (PTA) and stent placement. US-guided access was obtained from both right and left popliteal veins, and 8 Fr sheaths were inserted. Contrast venography was performed to both the deep femoral and iliac veins, demonstrating vessel patency throughout with visually apparent luminal narrowing in the left iliac vein. IVUS confirmed a 40% compression of the right external iliac vein (EIV) and a diffuse 80% fibrotic stenosis of the left common iliac vein (CIV) to CFV (Figure 2A). Extensive pelvic collaterals were also noted (Figure 2B). We performed PTA of the left CIV with a 16 mm x 40 mm Atlas Gold balloon (BD). Following balloon angioplasty, through the 8 Fr sheath, we deployed a 16 x 140 mm Zilver Vena stent from the left CIV into the EIV and deployed another 16 x 60 mm Zilver Vena stent overlapping with the first stent from the EIV into the CFV. The stents were post-dilated with the same Atlas Gold balloon, and a postprocedure venogram and IVUS showed excellent results, with complete resolution of the pelvic collaterals (Figure 2C). She was discharged home on clopidogrel 75 mg daily in addition to the apixaban 5 mg twice daily that she was already on. On a follow-up visit 1 month later, the patient reported significant reduction of her lower extremity edema, pain, and redness. On a 6-month follow-up, she reported complete resolution of these symptoms as well as pelvic pain and dyspareunia.

Case II
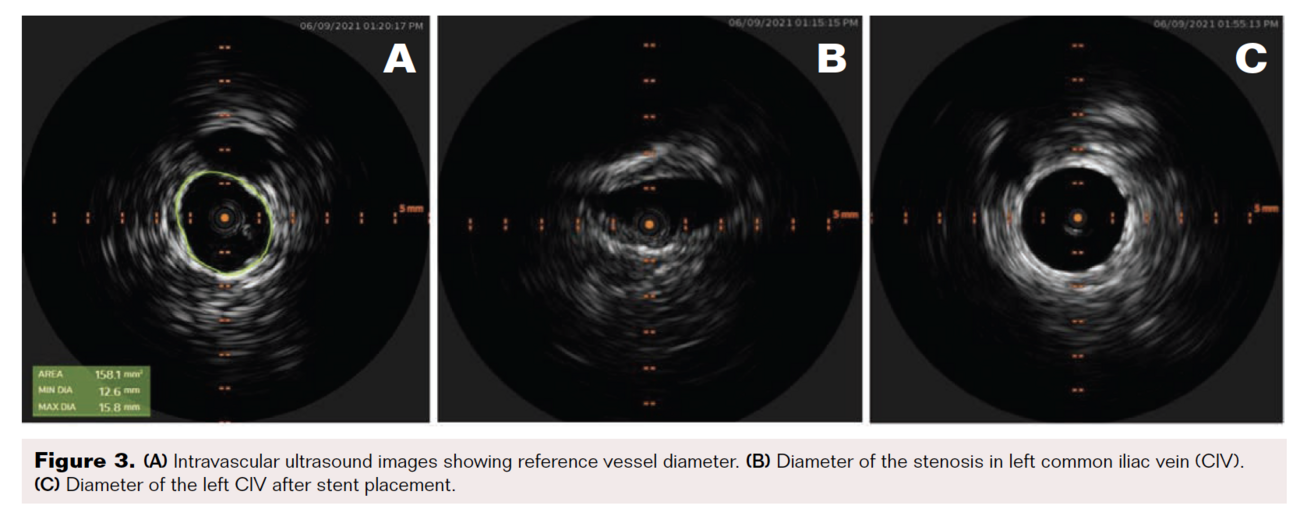
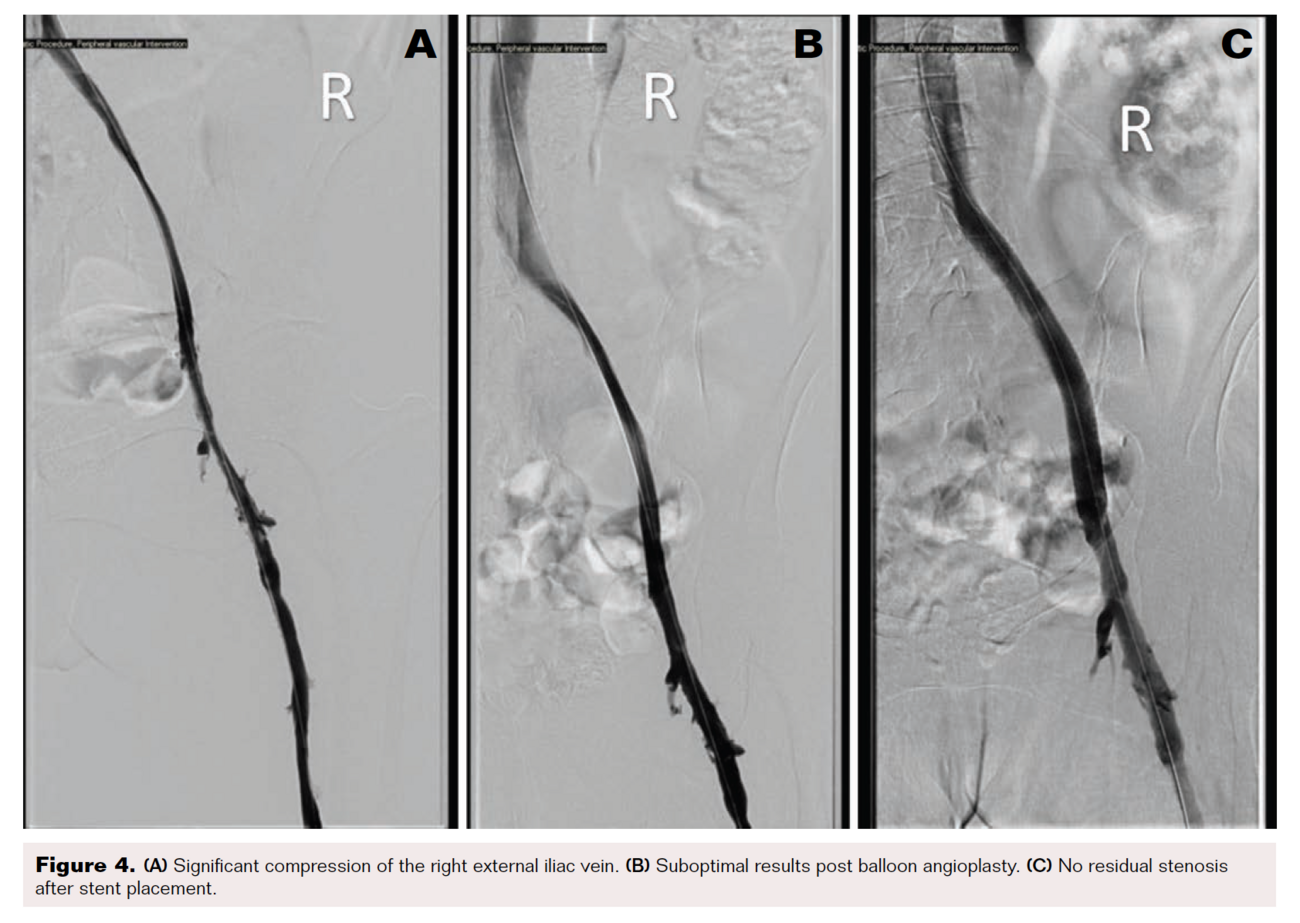
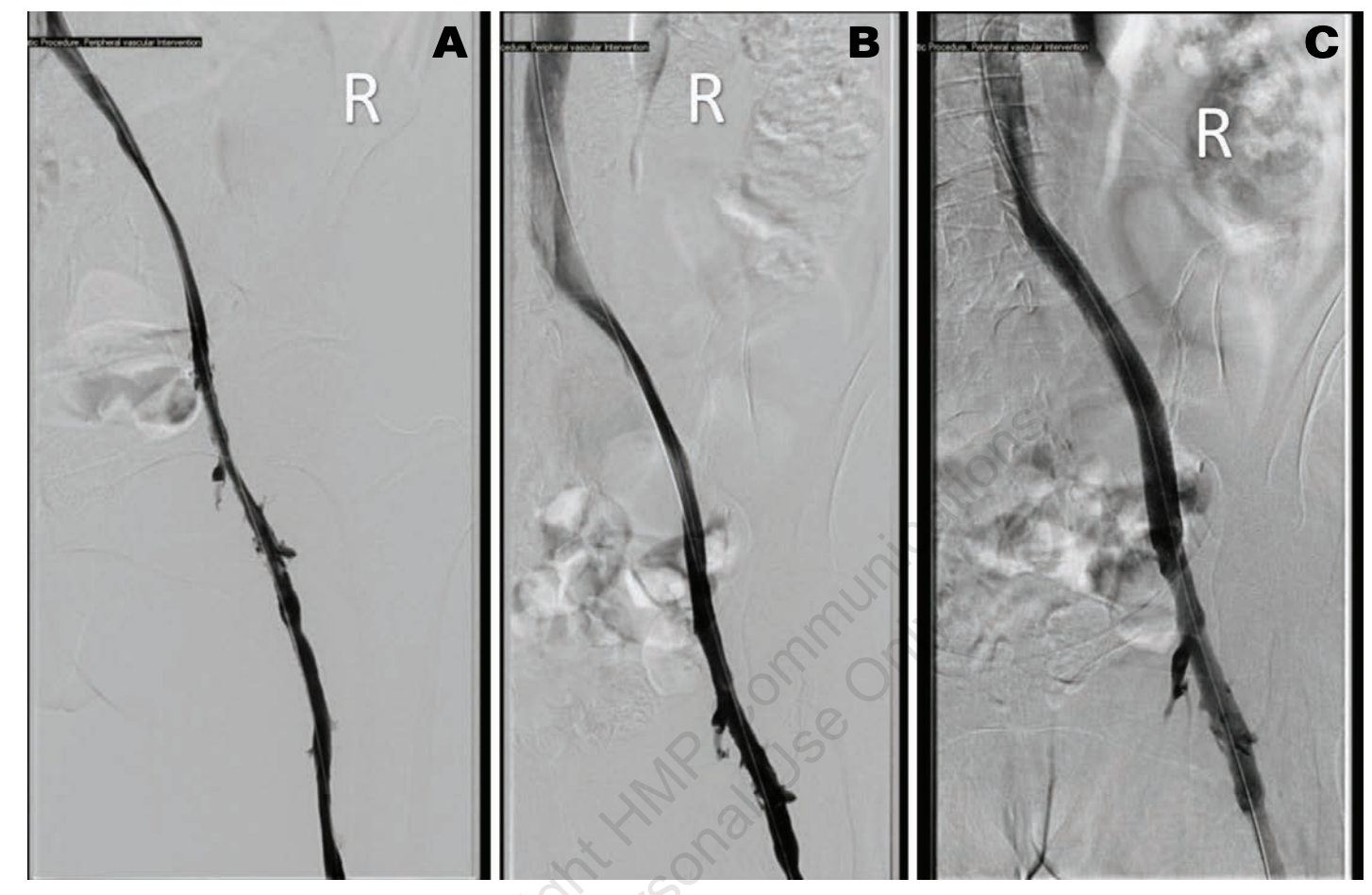
A 57-year-old woman with a history of severe rheumatoid arthritis and urothelial carcinoma of the bladder with a chronic urostomy in place was referred to our clinic for chronic right lower extremity pain and swelling. At the time of original presentation, she was experiencing symptoms for 2 years. Our initial workup with venous duplex US of the lower extremity showed patent veins with no evidence of thrombus; severe venous reflux disease was noted in the right greater saphenous vein (GSV) and small saphenous vein (SSV). After failed conservative management for several months with a graded compression stocking, leg elevation, and calf exercises, she underwent ablation of the GSV with Varithena (Boston Scientific), followed by ablation of the SSV a few months later with radiofrequency ablation. Despite ablation, swelling persisted, and 2 months after her vein ablation she presented with dramatically worsened lower extremity pain, swelling, and redness. US of the lower extremity showed occlusive DVT of the right CFV. We scheduled her for a right venogram with planned thrombectomy of the proximal acute DVT. Access was obtained from the right popliteal vein with US guidance. The vein was initially accessed with micropuncture because the popliteal vein caliber was exquisitely small. After access, the micropuncture sheath was upsized to 8 Fr. Contrast was injected through the 8 Fr sheath to obtain diagnostic images. The patient had 90% stenosis of the right CFV with a heavy thrombus burden and severe, diffuse compression of a small caliber right EIV of 70%. An IVUS catheter was advanced into the EIV and pulled back to confirm the degree of stenosis. This confirmed small-caliber central vein sizes. IVC measured 8.3 mm in the minor axis and 16 mm in the major axis, with a cross-sectional area of 112 mm2; EIV measured 7.4 mm in diameter and 65 mm2 in a cross-sectional area; and CFV measured 11 mm in diameter and 103.8 mm2 in a cross-sectional area (Figure 3). The patient underwent thrombectomy of the right CFV utilizing ClotHunter (Boston Scientific) with ZelanteDVT (Boston Scientific), with excellent clot debulking of 0% residual clot burden after thrombectomy. For the EIV, a balloon angioplasty was performed with a 12 x 80 mm Charger balloon (Boston Scientific), which did not result in reduction of the stenosis. A 12 x 140 mm Zilver Vena stent was placed in the common iliac vein to EIV and post-dilated with the same balloon with good results.
No residual stenosis was noted post procedure (Figure 4). At the end of the procedure, hemostasis of the popliteal vein was obtained with manual compression. On follow-up over the next 6 months, the patient’s edema slowly decreased and substantially improved, along with eventually improved pneumatic mechanical compression. Her pain symptoms completely resolved soon after the procedure.
Discussion
Ileocaval venous obstruction (ICVO) by thrombotic occlusion or external compression leads to chronic venous disease resulting from venous hypertension. It often manifests as lower extremity edema, skin discoloration, venous claudication, orthostatic pain, and lower extremity ulcers, and may even predispose patients to DVT of the lower extremities.7,8 With enhanced clinical awareness, increased use of imaging techniques such as IVUS, and development of dedicated venous stents, more attention is being paid to this disease entity.8 Addressing ICVO by means of percutaneous angioplasty may not be sufficient due to residual stenosis from fibrosis or vessel recoil. Unlike arterial system disease, even a small amount of residual stenosis in the venous system can result in persistent venous hypertension.7 For arterial disease, a stenosis of 70% is traditionally considered significant for intervention, but a lower threshold is recommended for venous disease.7 It is important to restore the lumen diameter because it results in alleviation of symptoms, even with concomitant venous reflux disease.6,8 An ideal venous stent should be able to withstand the deformative force during ambulation while being flexible. Unlike arterial stents, which are more rigid, venous stents require flexibility while withstanding external compressive forces.
The Zilver Vena venous self-expanding stent is a Nitinol (nickel titanium) alloy, open-cell design, dedicated venous stent. It is available in 10 mm to 16 mm diameter and 40 mm to 140 mm length. It has a 7 Fr delivery system that is the smallest platform of all dedicated venous stents currently available and is passed over a 0.035" wire. In our cases, all procedures were completed over an 8 Fr sheath without need for upsizing. This was particularly useful in the second case where vein sizes were much smaller than average, expected norms. The Zilver Vena stent has 4 radio-opaque gold markers on each end that facilitate accurate positioning of the stent. Deployment is performed over a pin-and-pull mechanism with a smooth delivery, resulting in accurate stent placement. Typical sizing of the stent is 1 mm to 4 mm, oversized with respect to the estimated vessel diameter. Diameter of the vessel is determined by measuring the most normal-looking segment of the CIV, EIV, or CFV.
Alternatively, the size of the expanded balloon diameter used for predilatation can be used. Both of our patients who were treated with the Zilver Vena stent had thrombotic disease. In the first case, the patient suffered from chronic veno-occlusive disease from prior thrombosis that led to iliac vein scarring. The presence of pelvic collaterals is a strong indicator of the chronicity of the patient’s disease process that dates back over a decade. Consequently, she also suffered from PCS, which is one of the most common causes of noncyclic pelvic pain in premenopausal women, accounting for more than a third of chronic pelvic pain cases.9,10 It has a diverse etiology, contributing to chronic venous insufficiency and extrinsic venous compression.9–11 PCS leads to dysmenorrhea, dyspareunia, urinary urgency, and varices of the perineum and lower extremities. It leads to significant limitation of day-to-day activities and adversely affects quality of life.9
In the second case, superficial venous ablation was initially the target of treatment. The fact that the patient’s symptoms paradoxically worsened, and she ultimately developed a DVT, indicates the importance of considering central vein compression or stenosis in the differential diagnosis of patients presenting with symptoms of venous congestion. Around 2% to 5% of patients with chronic venous disease have iliac vein compression.12 The prevalence of central vein compression could be much higher, as a majority of patients are asymptomatic to minimally symptomatic and do not undergo workup.12 In our practice, we typically try to augment common femoral reflux and assess flow dynamics with a Valsalva maneuver to identify potential upstream iliac vein stenosis. Unfortunately, this was not performed in this patient, which may have led to the failure in identifying the upstream iliac disease. If there is strong suspicion for central vein compression, further imaging may be considered, such as MRA or venography. Given the very small iliac vein size (measured at 7.4 mm by IVUS), we attempted PTA first after thrombectomy, which resulted in suboptimal luminal gain. After stent placement, there was no residual stenosis, with a uniform gain in lumen size.
Several case reports using Zilver Vena stents have reported similar optimal outcomes.13-15 VIVO-EU is a prospective, single-arm, multicenter study that looked at the safety and patency rates of Zilver Vena stents; it followed 35 study patients for 12 months and showed high patency rates, reduction in symptoms, and low morbidity.16 A retrospective analysis of 58 patients who underwent Zilver Vena stent placement showed good patency rates (60.3% primary patency and 81% secondary patency) at 5 years, with clinical improvement in symptomatology.17 At the Vascular InterVentional Advances (VIVA) conference in October 2021, late-breaking clinical trials presented 3-year outcomes from the VIVO clinical study, which showed very high patency rates (90.3 ± 2.2%) for Zilver Vena stents by US at 3 years. It also noted freedom from clinically driven reinterventions at 92.6 ± 2% and freedom from reinterventions at 82.9 ± 2.6%. The study authors also noted sustained clinical improvement as measured by VCSS, VDS, CEAP “C”, and CIVIQ scores. No stent fractures were observed during the 2-year follow-up period.18
Conclusion
Based on the available evidence and experience at our center, venous intervention for ICVO with appropriately sized Zilver Vena venous self-expanding stents is associated with improved outcomes and symptom alleviation.
The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted December 9, 2021.
Address for correspondence: Avaneesh Jakkoju, MD, Cardiovascular Institute of the South, 225 Dunn St., Houma, LA 70360. Email: ajakkoju@gmail.com
REFERENCES
1. Williams ZF, Dillavou ED. A systematic review of venous stents for iliac and venacaval occlusive disease. J Vasc Surg Venous Lymphat Disord. 2020;8:145-153.
2. Callam MJ. Epidemiology of varicose veins. Br J Surg. 1994;81:167-173.
3. Evans CJ, Fowkes FG, Ruckley CV, Lee AJ. Prevalence of varicose veins and chronic venous insufficiency in men and women in the general population: Edinburgh Vein Study. J Epidemiol Community Health. 1999;53:149-153.
4. Zahariev T, Anastassov V, Girov K, et al. Prevalence of primary chronic venous disease: the Bulgarian experience. Int Angiol. 2009;28:303-310.
5. Raffetto JD, Mannello F. Pathophysiology of chronic venous disease. Int Angiol. 2014;33:212-221.
6. Neglén P, Hollis KC, Olivier J, Raju S. Stenting of the venous outflow in chronic venous disease: long-term stent-related outcome, clinical, and hemodynamic result. J Vasc Surg. 2007;46:979-990.
7. Jayaraj A, Raju S. The venous stent: is it primetime yet? In: Chaar CIO, ed. Current Management of Venous Diseases. Cham, Switzerland: Springer International Publishing; 2018:489-496.
8. Shamimi-Noori SM, Clark TWI. Venous stents: current status and future directions. Tech Vasc Interv Radiol. 2018;21:113-116.
9. Brown CL, Rizer M, Alexander R, Sharpe 3rd EE, Rochon PJ. Pelvic congestion syndrome: systematic review of treatment success. Semin Intervent Radiol. 2018;35:35-40.
10. Kuligowska E, Deeds 3rd L, Lu 3rd K. Pelvic pain: overlooked and underdiagnosed gynecologic conditions. Radiographics. 2005;25:3-20.
11. Durham JD, Machan L. Pelvic congestion syndrome. Semin Intervent Radiol. 2013;30:372-380.
12. Radaideh Q, Patel NM, Shammas NW. Iliac vein compression: epidemiology, diagnosis and treatment. Vasc Health Risk Manag. 2019;15:115-122.
13. Andersen PE, Midtgaard A, Brenøe AS, Elle B, Duvnjak S. A new nitinol stent for use in superior vena cava syndrome. Initial clinical experience. J Cardiovasc Surg (Torino). 2015;56:877-881.
14. Hashimoto S, Shiraishi J, Kimura M, et al. Zilver stent implantation through 4.5 French guiding sheath in iliac vein compression syndrome complicated with acute deep vein thrombosis. J Cardiol Cases. 2013;7:e53-e56.
15. Hng JZK, Su S, Atkinson N. May-Thurner syndrome, a diagnosis to consider in young males with no risk factors: a case report and review of the literature. J Med Case Rep. 2021;15:141.
16. O’Sullivan GJ, Karunanithy N, Binkert CA, Ortega MR, Lichtenberg M, McCann-Brown JA. One year outcomes of the VIVO-EU study of treatment of symptomatic iliofemoral outflow obstruction with the Zilver Vena venous self-expanding stent. Cardiovasc Intervent Radiol. 2021;44:1930-1936.
17. Salem AM, AboElNeel HA, Fakhr ME. Long-term outcome of dedicated venous stents in management of chronic iliofemoral obstruction. J Vasc Surg Venous Lymphat Disord. 2022;10:52-59.
18. Hofmann LV, Comerota A, McCann-Brown JA. Abstract No. LB01 VIVO clinical study of the Zilver Vena venous stent in the treatment of symptomatic iliofemoral venous outflow obstruction: 2-year outcomes. J Vasc Interv Radiol. 2021;32:S42.

{kind=link}