Interventional Radiology vs Interventional Cardiology for Genicular Artery Embolization: Who's the Best?
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Vascular Disease Management or HMP Global, their employees, and affiliates.
VASCULAR DISEASE MANAGEMENT. 2026;23(4):E54-E55
Genicular artery embolization (GAE) for chronic knee osteoarthritis is a rapidly emerging alternative to total knee replacement in individuals hoping to delay the more invasive surgery, or for those who are not candidates for knee replacement.1 As with many embolization procedures, the field has classically been dominated by interventional radiology (IR). Recently, interventional cardiology (IC) and vascular surgery have begun offering GAE, mostly in the outpatient setting.
In this edition of Vascular Disease Management, Hullon and Ahad present their work comparing cost effectiveness of GAE performed by interventional radiology and interventional cardiology. The authors report that IR was the primary provider of GAE, yielding greater health benefits (0.58 quality-adjusted life years [QALYs]) at a lower cost ($3940) compared to GAE by IC (0.51 QALYs at $4610). Additional analysis indicated that IC-performed GAE could become cost-effective if costs decreased, greater success rates were achieved, or utility improved.
While we commend the authors for their work showing the cost-effectiveness of GAE (when performed by IR over IC), we believe the wrong question is asked with this study. The better question is, How does procedural experience affect cost-effectiveness in GAE procedures? Experience is the key confounder here given the procedural results should be similar if similar techniques are utilized by both specialties. Pitting specialties against one another should generally be avoided, as this may exacerbate the emerging scarcity of care for patients.2 Furthermore, comparison between specialties feels contrary to our collective mission as health care providers and physicians, which is to help patients.
Additional confounders may have also been present but not necessarily obtainable from the large registry data. For example, if one group was using a more costly embolization material (ie, microspheres vs imipenem/cilastatin) this may have importantly biased the results. Also, the site of service was not obtained for GAE. One could assume that procedures mainly done in the ambulatory surgical center would be more cost-effective than those done in the hospital. Evaluating both embolization material type and site of service would be interesting areas of additional study as they relate to cost and quality.
Another criticism of the manuscript is that the number of procedures performed by each group were not listed. As IC-performed GAE is a recent development, it is possible that the number of GAEs by this group was very low, exposing the results to outliers (also known as heavy-tail influence).
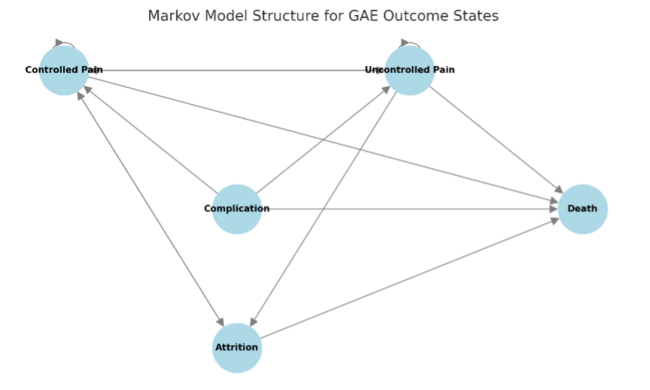
Furthermore, we do have a structural concern about the model design, which should be mentioned. The cost modeling was constructed as follows: “clinical effectiveness data were primarily sourced from 3 high-quality randomized controlled trials (RCTs) (Landers et al,3 van Zadelhoff et al,4 Bagla et al5) and the meta-analysis by Taslakian et al,6 which provided pooled estimates on pain reduction, functional improvement, and success rates.” However the meta-analysis contained the two RCTs already included in the model, which may have biased the results in favor of IR.
In conclusion, Hullon et al have performed a cost-effective analysis showing IR-performed procedures were more cost-effective with a higher utility than those performed by IC. We believe that the primary reason for this is procedural experience, given IC has largely just begun performing GAE. Rather than pitting specialties against each other, we should be looking at the effect of the learning curve on cost and quality in GAE. n
Click here to watch Dr Finn's video commentary.
References
1. Sajan A, Epelboym Y, Martínez AF, Little M, Talaie R, Isaacson A. Transarterial embolization for musculoskeletal pain management: AJR Expert Panel Narrative Review. AJR Am J Roentgenol. 2025;224(2):e2431626. doi:10.2214/AJR.24.31626
2. Silvestre J, Wooster MD, Seeger S, Rowe VL, Reitman CA. Trends in supply, demand, and workforce adequacy in vascular surgery: forecasting a national shortage. J Vasc Surg. 2025;82(3):1066-1072. doi:10.1016/j.jvs.2025.04.071
3. Landers S, Hely R, Hely A, et al. Genicular artery embolization for early-stage knee osteoarthritis: results from a triple-blind single-centre randomized controlled trial. Bone Jt Open. 2023;4(3):158-167. doi:10.1302/2633-1462.43.BJO-2022-0161.R2
4. van Zadelhoff TA, Bos PK, Moelker A, Bierma-Zeinstra SMA, van der Beijden RA, Oei EHG. Genicular artery embolisation versus sham embolisation for symptomatic osteoarthritis of the knee: a randomised controlled trial. BMJ Open. 2924;14(10):e087047. doi:10.1136/bmjopen-2024-087047
5. Bagla S, Piechowiak R, Sajan A, Orlando J, Hartman T, Isaacson A. Multicenter randomized sham controlled study of genicular artery embolization for knee pain secondary to osteoarthritis. J Vasc Interv Radiol. 2022;33(1):2-10.e2. doi:10.1016/j.jvir.2021.09.019
6. Taslakian B, Miller LE, Mabud TS, et al. Genicular artery embolization for treatment of knee osteoarthritis pain: systematic review and meta-analysis. Osteoarthr Cartil Open. 2023;5(2):100342. doi:10.1016/j.ocarto.2023.100342