Tackling the Calcium Challenge: Managing Recoil, Rupture, and Occlusion
An Interview With Kumar Madassery, MD
An Interview With Kumar Madassery, MD
Key Summary
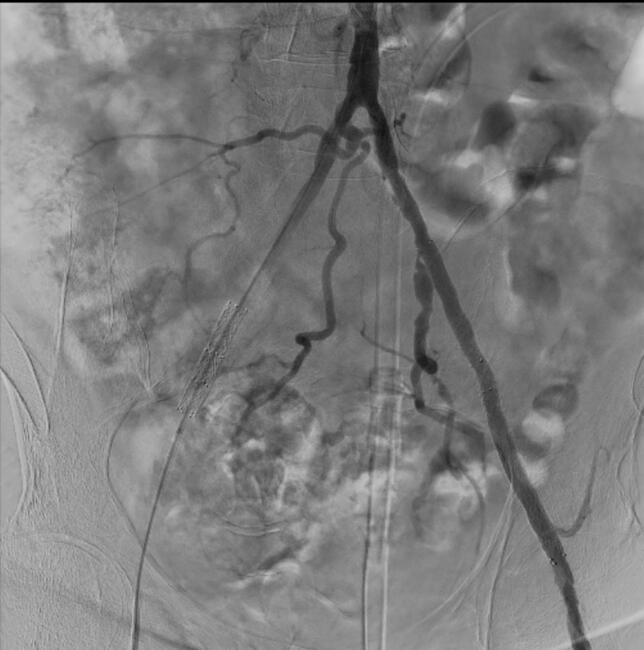
- Discussion focuses on patients with calcified lower-extremity arterial disease/chronic limb-threatening ischemia (CLTI), where clinicians assess calcium burden using intravascular ultrasound (IVUS) and noninvasive imaging in routine interventional practice.
- Heavy calcium often prevents adequate vessel expansion, which can lead to recoil, rupture, or occlusion; using calcium-modifying approaches can improve results, although distal vessels such as the ankle and foot remain particularly challenging, and poor expansion may result in suboptimal scaffold/drug-coated balloon (DCB) performance and restenosis.
- Vessels should be carefully assessed and prepared before intervention, and placing stents should be avoided when expansion is inadequate; however, current tools still have limitations, especially in severe or distal calcium, highlighting the need for continued advances in calcium-modifying strategies and procedural planning.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Vascular Disease Management or HMP Global, their employees, and affiliates.
VASCULAR DISEASE MANAGEMENT. 2026;23(4):E56-E57

Rush University Medical Center, Chicago, Illinois
At the Society of Interventional Radiology Annual Scientific Meeting in Toronto, vascular interventional radiologist Kumar Madassery, MD, from Rush University Medical Center in Chicago, highlighted one of the most stubborn obstacles in vascular intervention—heavy arterial calcium. In his presentation “Calcium Adventures: Management of Recoil, Rupture, Occlusion Due to Heavy Calcium,” he explored why calcified lesions continue to complicate treatment and how evolving imaging, vessel preparation strategies, and emerging technologies are helping clinicians improve outcomes.
Your presentation focuses on complications such as recoil, rupture, and occlusion. What makes calcium such a persistent challenge in interventional procedures today?
As we've advanced our ability to treat more and more complex levels of disease within the vasculature, we found that our patient population around the world has a higher level of complex arterial calcium. We are finding more difficult nodular, eccentric, and at times, uncrossable lesions. One problem is that in the past, the tools we have used really could not attack the problem of severe calcium, which can make it almost impossible to expand a vessel, as that calcium creates a barrier. This can result in recoil, re-occlusion, ineffective stent expansion, and sometimes rupture. We now have and are seeing more tools coming down the pipeline with a focus on modifying calcium, which is allowing us to disrupt the walls more, and has changed how complete we are able to treat the lower extremity arteries. Despite this, we still have trouble when we get to the ankle and to the foot regions where the vessels are smaller and can have a high level of intimal calcium. Also, unfortunately, with current approaches you still may have limitations to fully expand the vessel, sometimes you still may end up rupturing the vessel, and often you get recoil because you just can't expand that vessel well enough. This is why calcium has been the scourge of our CLTI world.
Can you walk us through some of the key strategies or tools you'll highlight in your talk for managing these calcium-related complications?
Several strategies are needed when addressing heavily calcified revascularization cases. For one, for these patients with a higher calcium burden, identifying the burden and distribution of calcium is important. Using our imaging techniques, including IVUS and noninvasive imaging, we have to determine how much calcium are we going to run into here, and if we will be dealing with circumferential, eccentric, nodular, coral reef variations of it. Based on that, we can then try to augment our interventions and our vessel prep, whether using atherectomy, lithotripsy, and/or any other modification tool, to increase vessel compliance, we can be better at preplanning to tackle that calcium, which is going to be a problem in the end. I will be talking through the diagnosis of it in terms of strategies for planning, what tools we currently have and some of their limitations, and also how to navigate the issues you may run into when you get ineffective expansion or rupture. How do you deal with scaffolds in the presence of heavy calcium? Those are going to be some of the main points of the strategies I'll talk about.
Are there particular cases or lessons from your own practice that shape the approach you're presenting?
Yes, what I've learned over the years of doing this is that we are severely undertreating the vessels to the point where you get ineffective scaffold expansion and other things such as DCB incorporation. If we don't get the vessel to expand properly, we can never get a good long-term result. We know that the definitive treatments we have do better when that calcium is modified. I have learned early on from not treating a vessel well myself, and I put very terrible stents in there, which never properly expanded, to try and not make that mistake again. If I cannot get a proper expansion, maybe don't place a scaffold. Or if I find that the calcium is eccentric or nodular, find another way to tackle that to prevent a restenosis and occlusion, things like that. Those learning lessons are good for clinicians to be more deliberate in their treatment of calcium.
What is the most important takeaway that you want attendees to get from your presentation?
To be aware of how difficult it is to treat calcium, how much of a problem it will be in your patients having long-term patency, to manage the possibility of complications that you have to be prepared for, and how to mitigate those possibilities. n