


Preoperative Devascularization of Large Neck Tumors Encasing the Internal Carotid Artery Using Hybrid Trapping Technique
Key Summary
- The authors describe a novel “technique of hybrid trapping” (THT) in a 32-year-old man with a Shamblin III carotid body tumor encasing the internal carotid artery (ICA). The approach combined balloon occlusion testing, ICA coil occlusion, and proximal common carotid artery control during surgery.
- Complete R0 tumor resection was achieved with minimal intraoperative blood loss, preserved cranial nerves, no postoperative neurological deficits, and discharge on postoperative day 5.
- The authors propose THT as a potential alternative to conventional embolization in selected patients with adequate collateral circulation; bilateral tumors and inadequate circle of Willis collateralization were noted limitations.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Vascular Disease Management or HMP Global, their employees, and affiliates.
VASCULAR DISEASE MANAGEMENT. 2026;23(6):E74-E78
Abstract
Preoperative control of vascularity in neck tumors encasing the internal carotid artery (ICA) remains surgically challenging, particularly when tumors extend to the skull base. We describe a novel hybrid technique, the technique of hybrid trapping (THT), which combines distal endovascular occlusion of the ICA with proximal surgical control of the common carotid artery. A 32-year-old patient with a Shamblin group III carotid body tumor underwent balloon occlusion test followed by parent artery occlusion of the ICA using coils, and subsequent surgical resection with proximal vascular control. The technique enabled effective devascularization, minimized intraoperative bleeding, and facilitated complete tumor excision. THT may represent a safe and effective alternative to conventional embolization in selected patients.
Large neck tumors, especially carotid body tumors (CBTs) encasing the carotid vessels, present significant surgical challenges due to high vascularity and proximity to critical neurovascular structures.1 Conventionally, preoperative embolization is performed for such cases, which has an intrinsic risk of non-target embolization through external carotid artery (ECA)–internal carotid artery (ICA) collaterals.2 Additionally, distal control of the ICA near the skull base is surgical, which would involve more extensive dissection and longer time.3
We describe a hybrid approach, technique of hybrid trapping (THT), which combines distal ICA occlusion via interventional radiology and proximal common carotid artery (CCA) control during surgery. This method aims to achieve efficient vascular trapping, thereby reducing intraoperative bleeding and improving surgical outcomes.
Technique Description
Concept
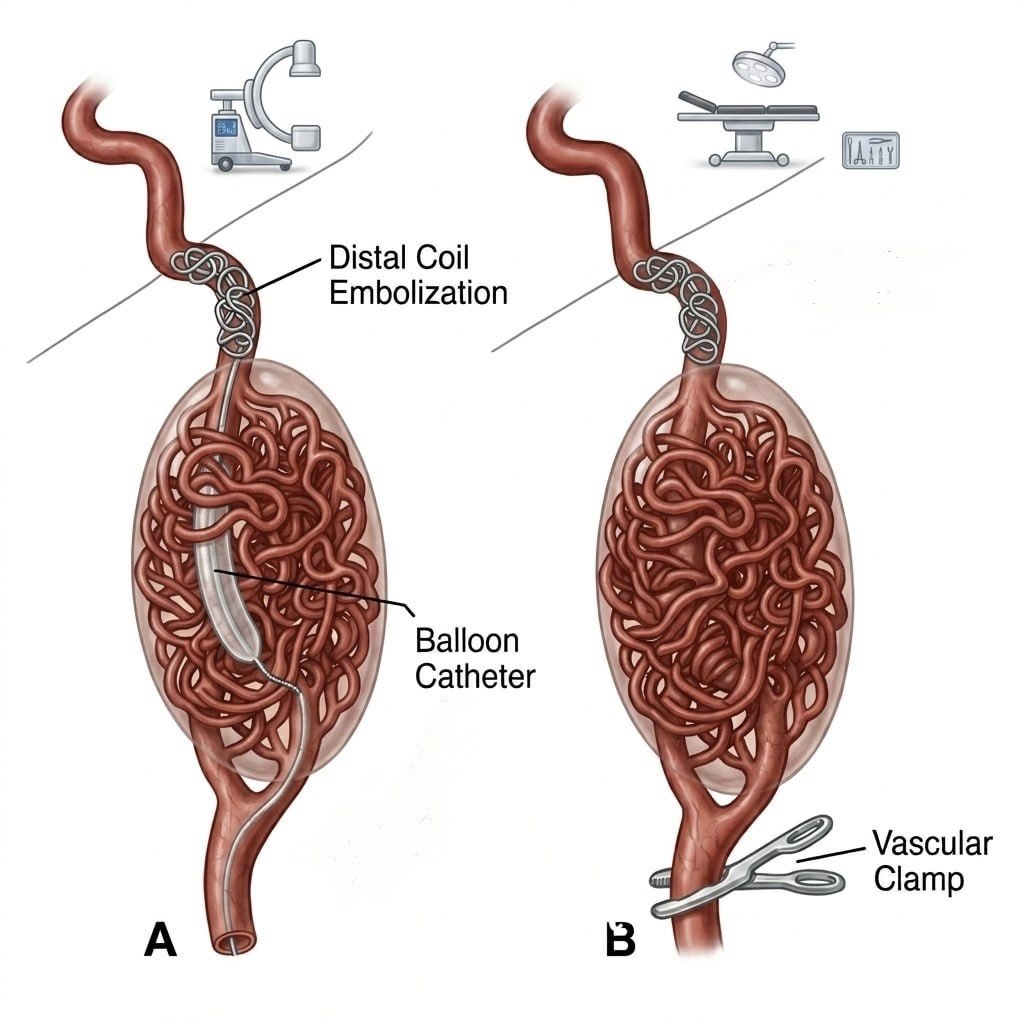
The THT is based on distal control by means of endovascular occlusion of the ICA near the skull base and proximal control by surgical clamping/ligation of the CCA (Figure 1). Because of this trapping, there is no further requirement of embolization of the tumor. This dual approach prevents antegrade and retrograde blood flow, minimizing bleeding from the ICA and ECA. It enables safer tumor dissection and decreases surgery time and blood loss.
Prerequisites
This technique requires adequate crossflow across the ipsilateral side and across the anterior communicating artery (ACOM) and posterior communicating artery (PCOM), as well as successful tolerance of a balloon occlusion test.4 This technique is not suitable for the patients with bilateral tumors.
Illustrated Case
A 32-year-old man presented with painless swelling on the right side of the neck of 3 months’ duration without any associated neurological deficits or compressive symptoms. Imaging demonstrated a large, heterogeneously enhancing lesion in the carotid space extending from the C2 to C4 vertebral levels, encasing the right CCA, ICA, and external ECA, suggestive of a CBT. It measured approximately 4.2 x 6.7 x 6.8 cm (AP x TR x CC).
A cerebral angiogram performed under local anesthesia revealed a highly vascular mass located in the right carotid space just above the CCA bifurcation, causing splaying of the ICA and ECA. The arterial supply to the lesion arose predominantly from multiple branches of the right ECA, especially the ascending pharyngeal artery, with additional contributions from the V2 segment of the right vertebral artery and the cervical segment of the right ICA. Crossflow was observed across the right PCOM with minimal flow across the anterior ACOM, likely due to preferential flow through the ipsilateral PCOM (Figure 2).
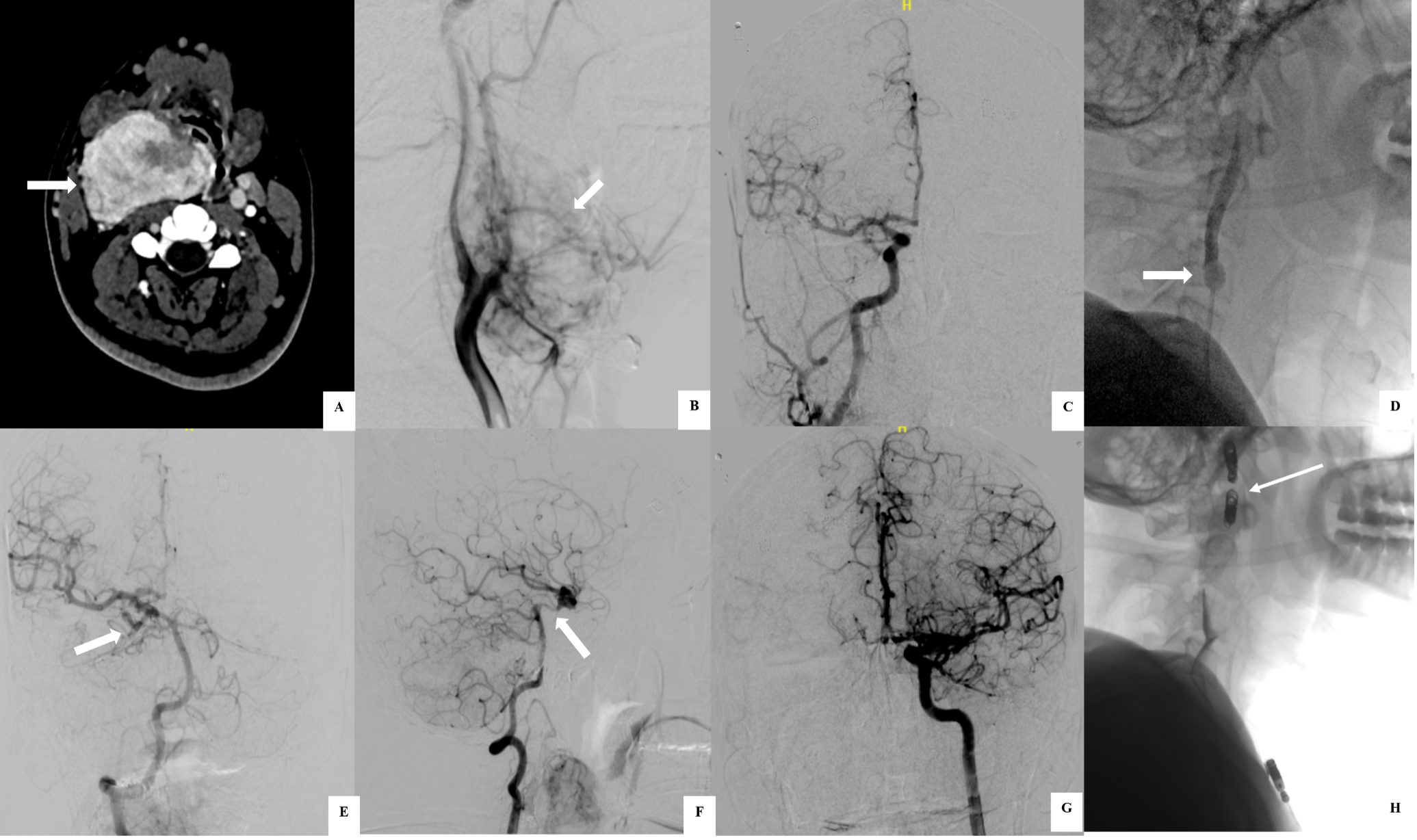
The THT was performed under local anesthesia with an aesthetic support for a hypotensive challenge. Bilateral common femoral artery access was obtained, with a 6F sheath placed on the right and a 4F sheath on the left. Through the right-sided access, a Fogarty balloon catheter was positioned in the cervical segment of the right ICA beyond the carotid bulb and inflated to achieve temporary occlusion. Through the left femoral access, a diagnostic catheter was advanced to assess crossflow across the ACOM and PCOM, which was found to be adequate, with no evidence of venous phase delay. Continuous neurological assessment was performed by engaging the patient in orientation-based questioning, while simultaneous somatosensory evoked potential monitoring was conducted. After 10 minutes of occlusion, the mean arterial pressure was reduced by approximately 20% under an aesthetic supervision to simulate a hypotensive challenge. Following a total occlusion time of 30 minutes during which the patient remained neurologically intact, the ICA was permanently occluded using a 6 mm x 20 cm detachable Interlock coil (Boston Scientific), along with 4 additional pushable coils (6 x 14 cm, 5 x 14 cm, and two 3 x 14 cm; Cook Medical).
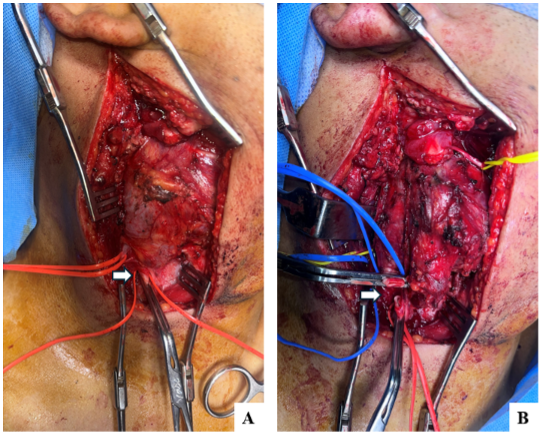
Subsequently, surgical resection was carried out under general anesthesia. Intraoperatively, a Shamblin group III CBT measuring 7 x 5 x 4 cm was identified, with complete encasement of the carotid bifurcation and compression of the internal jugular vein (Figure 3). Careful dissection allowed preservation of adjacent cranial nerves. Proximal vascular control was achieved by ligation of the CCA, and the distal ends of the ICA and ECA were transected to facilitate complete tumor excision. Total removal of the tumor with histologically negative margins and no residual microscopic disease was achieved (R0 resection), with minimal intraoperative blood loss, and meticulous hemostasis was ensured. Histopathology report later confirmed the paraganglioma diagnosis.
The patient had an uneventful postoperative recovery and was discharged on postoperative day 5 without any neurological deficits.
Discussion
The THT provides several advantages over conventional embolization. It is primarily employed in selected clinical scenarios, including but not limited to:
(a) Cases where preservation of the ICA is not feasible based on preoperative CT imaging, such as tumors demonstrating 360-degree encasement of the ICA (Shamblin III)1;
(b) Tumors with intracranial extension, where complete (R0) resection cannot be achieved through a neck incision alone and postoperative radiotherapy is planned for residual intracranial disease; and
(c) Tumors in which en bloc excision with the carotid vessels is anticipated.
This approach facilitates superior distal vascular control, particularly near the skull base, which is often difficult to achieve using surgical techniques alone. Also, by avoiding embolic agents within the external carotid circulation, it minimizes the risk of non-target embolization.5,6 The technique significantly reduces intraoperative blood loss, thereby improving surgical field clarity and facilitating complete tumor resection. Additionally, it may contribute to reduced operative time and decreased radiation exposure compared with prolonged endovascular procedures. The underlying principle of vascular trapping can also be extended to other clinical scenarios, including skull base tumors and highly vascular tumors in different anatomical regions.
However, THT has certain limitations. It is not suitable for bilateral disease unless a vascular bypass is planned. Successful implementation requires adequate intracranial collateral circulation, particularly through the circle of Willis. Despite trapping, some residual collateral supply, such as from the vertebral artery or contralateral external carotid artery, may persist, which supplies part of a tumor that has to be attempted during surgery.
Conclusion
The THT is a safe and effective method for preoperative devascularization of large CBTs encasing the ICA. It minimizes intraoperative bleeding and enhances surgical resectability in carefully selected patients.
Affiliations and Disclosures
Rajat Singhal, DM, DNB, FRCR, EBIR, Rajchandra Singh Kharayat, DM, DNB, and Shyamkumar N. Keshava, FRCR (UK), FRANZCR, DNB, DRNB, are from the Department of Interventional Radiology, Christian Medical College, Vellore, India; L. Samuel Prabhu Mithra, Mch, MS and Deepak Selvaraj, Mch, MS, MRCS, are from the Department of Vascular Surgery, Christian Medical College, Vellore, India.
Acknowledgement: The authors would like to extend their sincere gratitude to Dr. Sneha H for her valuable assistance with the graphical illustrations.
The authors report no financial relationships or conflicts of interest regarding the content herein.
This study was conducted in accordance with institutional ethical standards. Informed consent was obtained from the patient for publication.
Manuscript accepted April 22, 2026.
Address for Correspondence: Shyamkumar N. Keshava, Department of Interventional Radiology, Division of Clinical Radiology, Christian Medical College Vellore, Tamil Nadu – 632002, India. Email: shyamkumar.n.keshava@gmail.com
References
1. Metheetrairut C, Chotikavanich C, Keskool P, Suphaphongs N. Carotid body tumor: a 25-year experience. Eur Arch Otorhinolaryngol. 2016;273(8):2171-2179. doi:10.1007/s00405-015-3737-z
2. Zhang J, Fan X, Zhen Y, et al. Impact of preoperative transarterial embolization of carotid body tumor: a single center retrospective cohort experience. Int J Surg. 2018;54(Pt A):48-52. doi:10.1016/j.ijsu.2018.04.032
3. Kilic Y, Jalalzai I, Sönmez E, Erkut B, Jalalzai M. The surgical treatment of carotid body tumor as well as the prevention and management of complications. Cureus. 2024;16(1):e51807. doi:10.7759/cureus.51807
4. Narayanan S, Singer R, Abruzzo TA, et al; Standards and Guidelines Committee of the Society of NeuroInterventional Surgery. Reporting standards for balloon test occlusion. J Neurointerv Surg. 2013;5(6):503-505. doi:10.1136/neurintsurg-2013-010848
5. Economopoulos KP, Tzani A, Reifsnyder T. Adjunct endovascular interventions in carotid body tumors. J Vasc Surg. 2015;61(4):1081-1091.e2. doi:10.1016/j.jvs.2015.01.035
6. Abu-Ghanem S, Yehuda M, Carmel NN, Abergel A, Fliss DM. Impact of preoperative embolization on the outcomes of carotid body tumor surgery: a meta-analysis and review of the literature. Head Neck. 2016;38 Suppl 1:E2386-2394. doi:10.1002/hed.24381
