


Transradial Carotid Artery Stenting
Abstract
Transradial carotid artery stenting is an increasingly popular alternative to carotid endarterectomy. The advantages of transradial access along with techniques to selectively engage the carotid artery are further illustrated by the case herein.
Case
A 62-year-old male with history of atrial fibrillation on anticoagulation presented with a transient episode of left-sided weakness. Additional comorbidities included diabetes, heart failure with left ventricular ejection fraction of 30-35%, and coronary artery disease not suitable for revascularization. Computed tomography (CT) angiography did not reveal any focal infarcts but confirmed an 80% stenotic lesion in the right internal carotid artery and 60% stenosis of the right subclavian artery just distal to the right common carotid artery takeoff.
The patient was scheduled for percutaneous carotid artery stenting (CAS) when he was turned down for carotid endarterectomy due to prohibitive risk factors for surgery. A left radial artery access approach was utilized due to the obstructive lesion in the right subclavian artery.
A 6 French sheath was placed using a micropuncture access needle in the left radial artery. An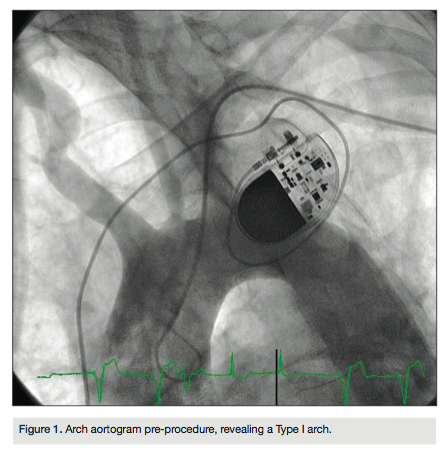 arch aortogram revealed a Type I aortic arch with no significant atheroma (Figure 1). A Simmons 2 catheter (AngioDynamics) was used to selectively engage the right common carotid artery by looping the catheter in the right coronary cusp. A stiff-angled Glidewire (Terumo) was then used as an anchor in the right external carotid artery (Figure 2A) and a Pinnacle Destination sheath (Terumo) advanced into the right common carotid artery (Figure 2B). Selective angiogram confirmed an 80% stenosis of the right internal carotid artery (Figure 3). An Emboshield distal embolic protection device (Abbott Vascular) was deployed in a straight segment in the distal right internal carotid artery. After pre-dilation with a Viatrac 4.0 x 20 mm
arch aortogram revealed a Type I aortic arch with no significant atheroma (Figure 1). A Simmons 2 catheter (AngioDynamics) was used to selectively engage the right common carotid artery by looping the catheter in the right coronary cusp. A stiff-angled Glidewire (Terumo) was then used as an anchor in the right external carotid artery (Figure 2A) and a Pinnacle Destination sheath (Terumo) advanced into the right common carotid artery (Figure 2B). Selective angiogram confirmed an 80% stenosis of the right internal carotid artery (Figure 3). An Emboshield distal embolic protection device (Abbott Vascular) was deployed in a straight segment in the distal right internal carotid artery. After pre-dilation with a Viatrac 4.0 x 20 mm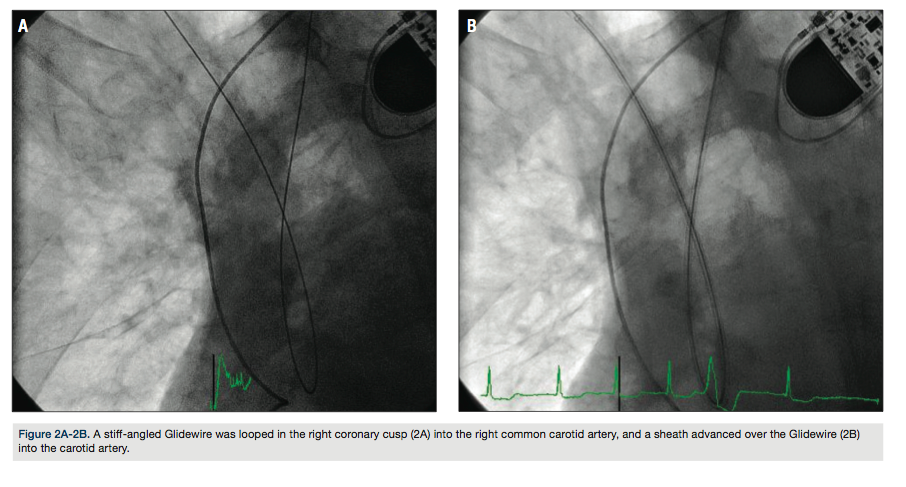 balloon (Abbott Vascular), an Xact 6-8 x 30 mm self-expanding stent (Abbott Vascular) was deployed in the right internal carotid artery, and post-dilated using a Viatrac 5.0 x 20 mm balloon. Final angiogram confirmed excellent angiographic result and brisk flow (Figure 4). The patient was discharged home the following day after initiation of dual antiplatelet therapy indefinitely.
balloon (Abbott Vascular), an Xact 6-8 x 30 mm self-expanding stent (Abbott Vascular) was deployed in the right internal carotid artery, and post-dilated using a Viatrac 5.0 x 20 mm balloon. Final angiogram confirmed excellent angiographic result and brisk flow (Figure 4). The patient was discharged home the following day after initiation of dual antiplatelet therapy indefinitely.
Discussion
Percutaneous carotid artery stenting (CAS) has become a viable alternative to the standard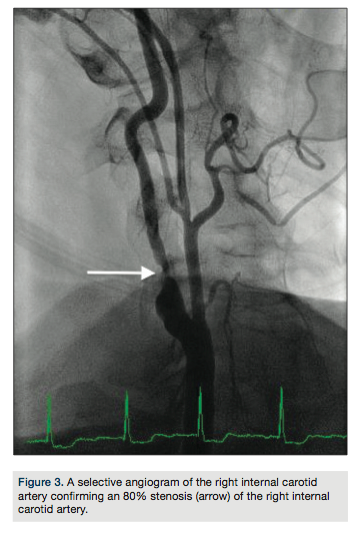 approach of carotid endarterectomy.1 The femoral artery has traditionally been the access site for CAS procedures, although complicated by anatomical variations and peripheral arterial disease.
approach of carotid endarterectomy.1 The femoral artery has traditionally been the access site for CAS procedures, although complicated by anatomical variations and peripheral arterial disease.
The advantages of transradial access for coronary interventions have been well established.2 Recently, transradial access for CAS has been evaluated with favorable outcomes.3 While CAS in the right internal carotid artery and bovine left internal carotid artery (left common carotid artery arising from right brachiocephalic artery) disease is technically uncomplicated4, it can be challenging in a non-bovine left internal carotid artery (left common carotid artery arising directly from aorta) stenosis.5
A transradial approach for CAS is a variation of the standard femoral approach.3 A diagnostic catheter, positioned in the common carotid artery, is used for insertion of an exchange-length, supportive guide wire into the external carotid artery for an anchor, over which a long sheath is advanced. Upper extremity access requires negotiation of acute angles and different strategies to selectively engage the common carotid artery. Once the sheath is in place, the remainder of the procedure, including embolic protection device deployment, balloon angioplasty, stenting, and embolic protection device retrieval, are identical to the femoral approach.
catheter, positioned in the common carotid artery, is used for insertion of an exchange-length, supportive guide wire into the external carotid artery for an anchor, over which a long sheath is advanced. Upper extremity access requires negotiation of acute angles and different strategies to selectively engage the common carotid artery. Once the sheath is in place, the remainder of the procedure, including embolic protection device deployment, balloon angioplasty, stenting, and embolic protection device retrieval, are identical to the femoral approach.
Non-bovine left internal carotid artery CAS using transradial access has been associated with a higher incidence of failure due to the extreme angles involved, resulting in poor support for the catheter system.4 In these scenarios, the wire-braided Simmons 2 catheter was found to provide easier access, with a stepwise guide wire exchange to a stiff guide wire using the telescoping technique.3
The overall complications rate for transradial CAS is low, including death (0.3%), major stroke (0.6%), minor stroke (1%), intra-procedural transient ischemic attack (3%), asymptomatic radial artery occlusion (7%), and no major vascular complications in a series of 347 patients.3
The right radial artery is the most common access utilized3, but the left radial technique has also been well established.5 For cases with poor guide support, the catheter looping and retrograde engagement technique (CLARET) has been described as an alternative strategy.6 This technique utilizes the right coronary cusp to loop the guide wire to engage the carotid artery, providing inferior support for the guide and sheath.
Multiple studies have demonstrated the feasibility of a transradial approach to CAS. While it is particularly indicated in patients where the femoral approach is not available7, it may also be the preferred approach in patients with bovine left internal carotid artery disease.5 Moreover, a transradial approach may reduce catheter-induced embolization from the transverse aortic arch.8
Disclosure: Dr. George reports that he is a consultant for Boston Scientific.
Jon C. George, MD, can be contacted at jcgeorgemd@gmail.com.
References
- Brott TG, Hobson RW, Howard G, et al. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med. 2010; 363: 11-23.
- Vorobcsuk A, Konyi A, Aradi D, et al. Transradial versus transfemoral percutaneous coronary intervention in acute myocardial infarction. Systematic overview and meta-analysis. Am Heart J. 2009; 158: 814-821.
- Etxegoien N, Rhyne D, Kedev S, et al. The transradial approach for carotid artery stenting. Catheter Cardiovasc Interv. 2012; 80: 1061-1067.
- Folmar J, Sachar R, Mann T. Transradial approach for carotid artery stenting: a feasibility study. Catheter Cardiovasc Interv. 2007; 69: 355-361.
- Patel T, Shah S, Ranian A, et al. Contralateral transradial approach for carotid artery stenting: a feasibility study. Catheter Cardiovasc Interv. 2009; 75: 268-275.
- Fang H, Chung S, Sun C, et al. Transradial and transbrachial arterial approach for simultaneous carotid angiographic examination and stenting using catheter looping and retrograde engagement technique. Ann Vasc Surg. 2010; 24: 670-679.
- Yoo BS, Lee SH, Kim JY, Lee HH, Ko JY, Lee BK, Hwang SO, Choe KH, Yoon J. A case of transradial carotid stenting in a patient with total occlusion of distal abdominal aorta. Catheter Cardiovasc Interv. 2002; 56:
- 243-245.
- Faggioli G, Ferri M, Rapezzi C, et al. Atherosclerotic aortic lesions increase the risk of cerebral embolism during carotid stenting in patients with complex aortic arch anatomy. J Vasc Surg. 2009; 49: 80-5.


