

Advancing Diabetes Management Through Continuous Ketone Monitoring
Click above to download the full white paper.
EXECUTIVE SUMMARY
Diabetic ketoacidosis (DKA) is one of the most dangerous and costly complications of diabetes, with an average hospital admission in the United States exceeding $30,836 and total annual charges surpassing $6.7 billion as of 2017. Despite advances in glucose monitoring and insulin delivery, DKA remains a growing clinical burden in the United States with rates continuing to rise, particularly among younger adults aged 18 to 44 years. Recent analyses report approximately a 55% increase in DKA hospitalization rates over the past decade. Severe DKA is linked to higher hemoglobin A1c (HbA1c), greater insulin requirements, and increased risk of subsequent DKA, underscoring lasting clinical and developmental consequences. Recent analyses of national mortality data report DKA-related mortality increasing by 37% in the most recent decade and rising further during the COVID-19 pandemic, underscoring persistent gaps in diabetes management and timely intervention.
Use of current ketone testing methods—including urine strips, blood meters, and breath analyzers—remains episodic and reactive. Surveys indicate that nearly one-third of people with type 1 diabetes (T1D) do not have ketone testing supplies at home, and fewer than one in five own a blood ketone meter. As a result, many patients and providers lack timely visibility into ketone levels until symptoms appear and a metabolic crisis is already underway.
Continuous ketone monitoring (CKM) offers a transformative solution by providing real-time beta-hydroxybutyrate (BHB) measurements, enabling early detection of rising ketones before full metabolic decompensation. Early feasibility studies have shown that CKM sensors can reliably track ketone levels over extended periods, and development is now progressing toward integrated devices that measure both glucose and ketones simultaneously to streamline workflows. These devices can connect to mobile apps and cloud-based systems, enabling remote monitoring and coordinated care. One device has already received Breakthrough Device designation from the US Food and Drug Administration (FDA), signaling recognition of its potential to meet a significant unmet clinical need. Recent international expert consensus recommendations endorsed by the International Society for Pediatric and Adolescent Diabetes (ISPAD) and published in 2026 highlight CKM as an emerging diabetes safety technology with the potential to reduce the risk of diabetic ketoacidosis through earlier detection of rising ketone levels and structured alert thresholds for clinical action.
CKM is particularly valuable for high-risk groups, including individuals with T1D, type 2 diabetes (T2D) on insulin, and those taking sodium-glucose cotransporter-2 (SGLT2) inhibitors. Successful adoption of CKM will require clinical validation, demonstration of cost-effectiveness, and integration into existing care platforms. Even a modest reduction in DKA-related hospitalizations could generate significant healthcare savings while improving patient safety and quality of life.
In summary, CKM represents a paradigm shift in diabetes care. By moving from episodic, reactive testing to continuous prevention, CKM has the potential to reduce emergency department visits, prevent hospital admissions, improve outcomes, and establish a new standard of safety in diabetes management.
INTRODUCTION
Diabetic ketoacidosis (DKA) persists as one of the most dangerous, disruptive, and costly complications across the diabetes continuum. Even as continuous glucose monitoring (CGM), automated insulin delivery, and evidence-based care pathways have improved glycemic control, DKA rates and DKA-related expenditures continue to rise, especially in younger adults and other high-risk groups.1 The epidemiology is shifting as well: the expansion of sodium-glucose cotransporter-2 (SGLT2) inhibitor use into broader type 2 diabetes (T2D) populations has enlarged the cohort susceptible to ketone overproduction and euglycemic presentations, extending risk beyond the traditional type 1 diabetes (T1D) population.2
Real-world use of ketone testing remains largely episodic and reactive, leaving predictable blind spots that delay recognition and intervention. This enduring gap in diabetes safety underscores the need for a proactive, population-level strategy. Continuous ketone monitoring (CKM) offers that opportunity—delivering real-time detection of metabolic risk before crisis develops. By shifting care from reactive management to continuous prevention, CKM has the potential to transform diabetes safety at both the individual and system levels.
This white paper examines how CKM represents a new frontier in diabetes management: one that improves patient outcomes, reduces avoidable emergency resource utilization, and generates meaningful cost savings for payers. Integrating CKM into care pathways provides a practical framework for earlier intervention, fewer hospital admissions, and a redefined standard of safety for individuals living with diabetes.
Recognition of PPF as a distinct form of fibrotic disease outside of IPF has expanded awareness of fibrosing ILDs. Patients with fibrosing ILDs such as chronic hypersensitivity pneumonitis, interstitial pneumonia, connective tissue disease–associated ILD, and unclassifiable ILD are at risk of developing a progressive fibrosing phenotype. An estimated 13% to 40% of these non-IPF fibrosing ILDs progress within two years despite appropriate management, with clinical trajectories, including rate of decline in forced vital capacity (FVC) and transplant-free survival, closely resembling those seen in IPF.8 Collectively, fibrosing ILDs exert substantial human and economic costs. Patients experience severe dyspnea, worsening cough, functional limitations, and deterioration of quality of life. At the same time, health care systems absorb costs from frequent hospitalizations due to acute exacerbations, oxygen therapy, and end-of-life care.1
THE CLINICAL TOLL OF DIABETIC KETOACIDOSIS: WHY EARLY DETECTION MATTERS
 DKA occurs when the body produces high levels of ketones, the acidic byproducts of fat metabolism.2 The underlying pathophysiology centers on unchecked ketone production resulting from insulin deficiency and counter-regulatory hormone excess. Among the ketone bodies, beta-hydroxybutyrate (BHB) is the most clinically relevant as it accumulates in the bloodstream and drives the anion gap metabolic acidosis that defines DKA.2,3 If left untreated, the resultant acidosis can progress rapidly to altered consciousness, cardiac collapse, coma, or death, underscoring the imperative for earlier and more reliable detection of rising ketone levels.3 The clinical stakes are especially high in pediatrics and young adults because any single DKA episode can impair development, including neurocognitive functions.4 In a large US claims-database study of 455,423 patients with T1D, the overall incidence rate of DKA was 55.5 events per 1,000 patient-years, with the highest incidence occurring among adolescents aged 10 to 19 years.5
DKA occurs when the body produces high levels of ketones, the acidic byproducts of fat metabolism.2 The underlying pathophysiology centers on unchecked ketone production resulting from insulin deficiency and counter-regulatory hormone excess. Among the ketone bodies, beta-hydroxybutyrate (BHB) is the most clinically relevant as it accumulates in the bloodstream and drives the anion gap metabolic acidosis that defines DKA.2,3 If left untreated, the resultant acidosis can progress rapidly to altered consciousness, cardiac collapse, coma, or death, underscoring the imperative for earlier and more reliable detection of rising ketone levels.3 The clinical stakes are especially high in pediatrics and young adults because any single DKA episode can impair development, including neurocognitive functions.4 In a large US claims-database study of 455,423 patients with T1D, the overall incidence rate of DKA was 55.5 events per 1,000 patient-years, with the highest incidence occurring among adolescents aged 10 to 19 years.5
In the acute setting, ketone monitoring can aid in the diagnosis and resolution of DKA. Traditional DKA diagnostic criteria that rely on pH or bicarbonate levels may miss DKA episodes when used alone.6 These criteria may not diagnose DKA accurately in the presence of mixed acid-base disorders, where bicarbonate or pH levels may not meet the classic thresholds for DKA.7 However, BHB levels remain elevated in these cases. Therefore, measurement of BHB is crucial to DKA diagnosis when acidosis is absent or masked.
RISING INCIDENCE AND ECONOMIC BURDEN: THE AVOIDABLE COST CURVE
 Despite advances in glucose monitoring and insulin delivery, DKA rates continue to rise, revealing a critical gap in comprehensive metabolic monitoring. Studies show a significant increase in DKA over the last two decades in the United States, with the highest rates observed in adults aged 18 to 44 years.1 Recent analyses also report approximately a 55% increase in DKA hospitalization rates over the past decade, particularly among younger adults.8 Recent analyses of national mortality data indicate that 40,770 deaths in the United States were attributed to DKA between 1999 and 2022, with DKA-related mortality increasing by 37% in the most recent decade and rising further during the COVID-19 pandemic, underscoring persistent gaps in diabetes management and timely intervention.9 The direct financial implications are substantial: the estimated average cost is approximately $30,836 per hospital admission, with total annual hospital charges in the United States surpassing $6.7 billion as of 2017.1
Despite advances in glucose monitoring and insulin delivery, DKA rates continue to rise, revealing a critical gap in comprehensive metabolic monitoring. Studies show a significant increase in DKA over the last two decades in the United States, with the highest rates observed in adults aged 18 to 44 years.1 Recent analyses also report approximately a 55% increase in DKA hospitalization rates over the past decade, particularly among younger adults.8 Recent analyses of national mortality data indicate that 40,770 deaths in the United States were attributed to DKA between 1999 and 2022, with DKA-related mortality increasing by 37% in the most recent decade and rising further during the COVID-19 pandemic, underscoring persistent gaps in diabetes management and timely intervention.9 The direct financial implications are substantial: the estimated average cost is approximately $30,836 per hospital admission, with total annual hospital charges in the United States surpassing $6.7 billion as of 2017.1
Many DKA cases are preventable, and a significant portion of this economic burden is considered avoidable with proper outpatient management, patient education, and consistent access to testing supplies.10 For managed care leaders, DKA represents an actionable opportunity: earlier risk detection and intervention can translate directly into reduced emergency department utilization, fewer admissions, and meaningful budget impact.
THE CURRENT KETONE TESTING LANDSCAPE
While glucose monitoring has become standard of care in diabetes management, particularly through CGM devices, use of ketone monitoring remains sporadic and reactive, despite its central role in preventing metabolic decompensation.
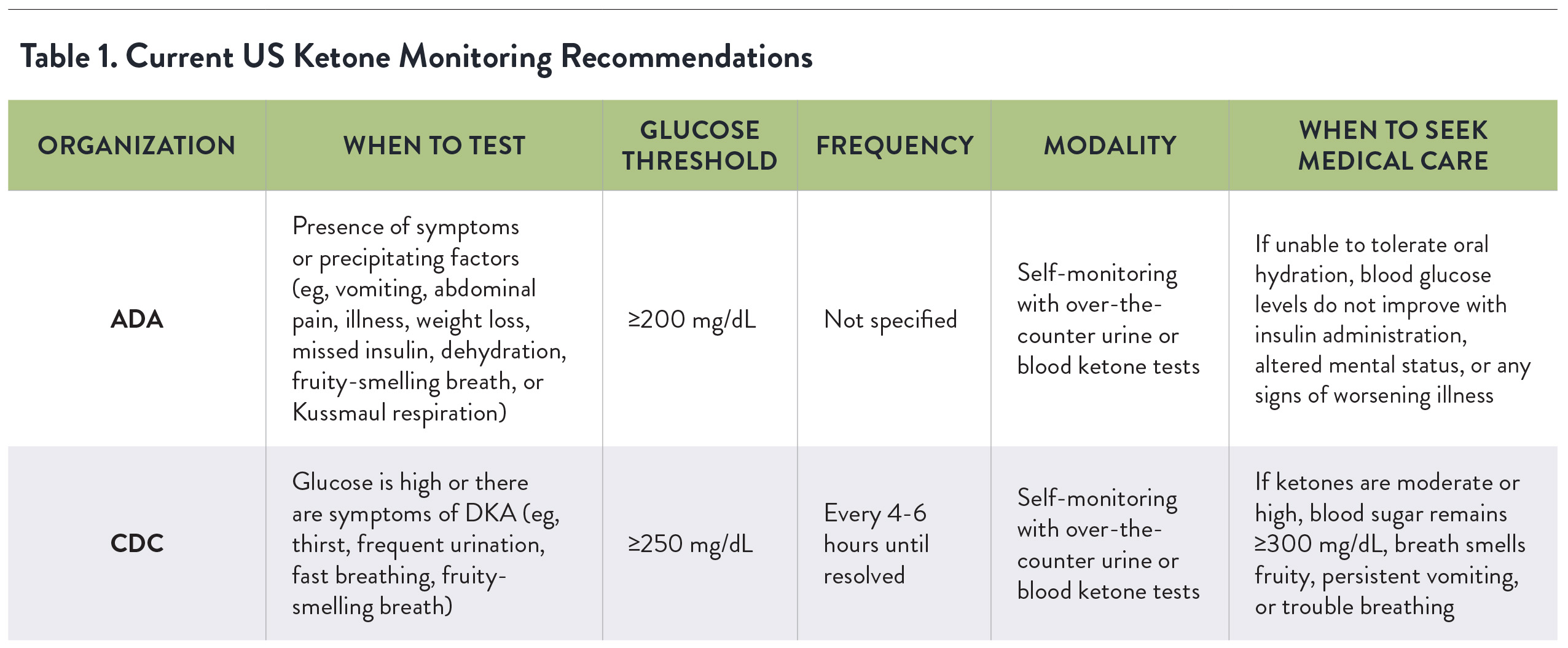
Current US recommendations for ketone self-monitoring remain symptom- and hyperglycemia-triggered rather than proactive. The American Diabetes Association (ADA) advises individuals at risk for DKA to check urine or blood ketones when precipitating factors are present (eg, illness, missed insulin, vomiting, weight loss, dehydration), particularly when glucose exceeds 200 mg/dL (11.1 mmol/L).11 The Centers for Disease Control and Prevention (CDC) recommends checking ketones when glucose is at or above 250 mg/dL, or when DKA symptoms occur, and repeating measurements every 4 to 6 hours (Table 1).12
 However, symptoms such as nausea, vomiting, and excessive thirst tend to appear late in the course of ketosis, and hyperglycemia is not always present or sufficient to prompt ketone testing, particularly in euglycemic (near-normal blood sugar) presentations associated with SGLT2 inhibitors, pregnancy, or when there is poor oral intake.3 As such, these directives are episodic, rely on patient recognition of symptoms, and provide limited guidance on testing cadence outside of illness—highlighting an opportunity for earlier, trend-based detection that continuous ketone monitoring could address.
However, symptoms such as nausea, vomiting, and excessive thirst tend to appear late in the course of ketosis, and hyperglycemia is not always present or sufficient to prompt ketone testing, particularly in euglycemic (near-normal blood sugar) presentations associated with SGLT2 inhibitors, pregnancy, or when there is poor oral intake.3 As such, these directives are episodic, rely on patient recognition of symptoms, and provide limited guidance on testing cadence outside of illness—highlighting an opportunity for earlier, trend-based detection that continuous ketone monitoring could address.
In addition, real-world adherence to currently available methods for ketone testing remains inconsistent and largely reactive, with a range of limitations (Table 2).
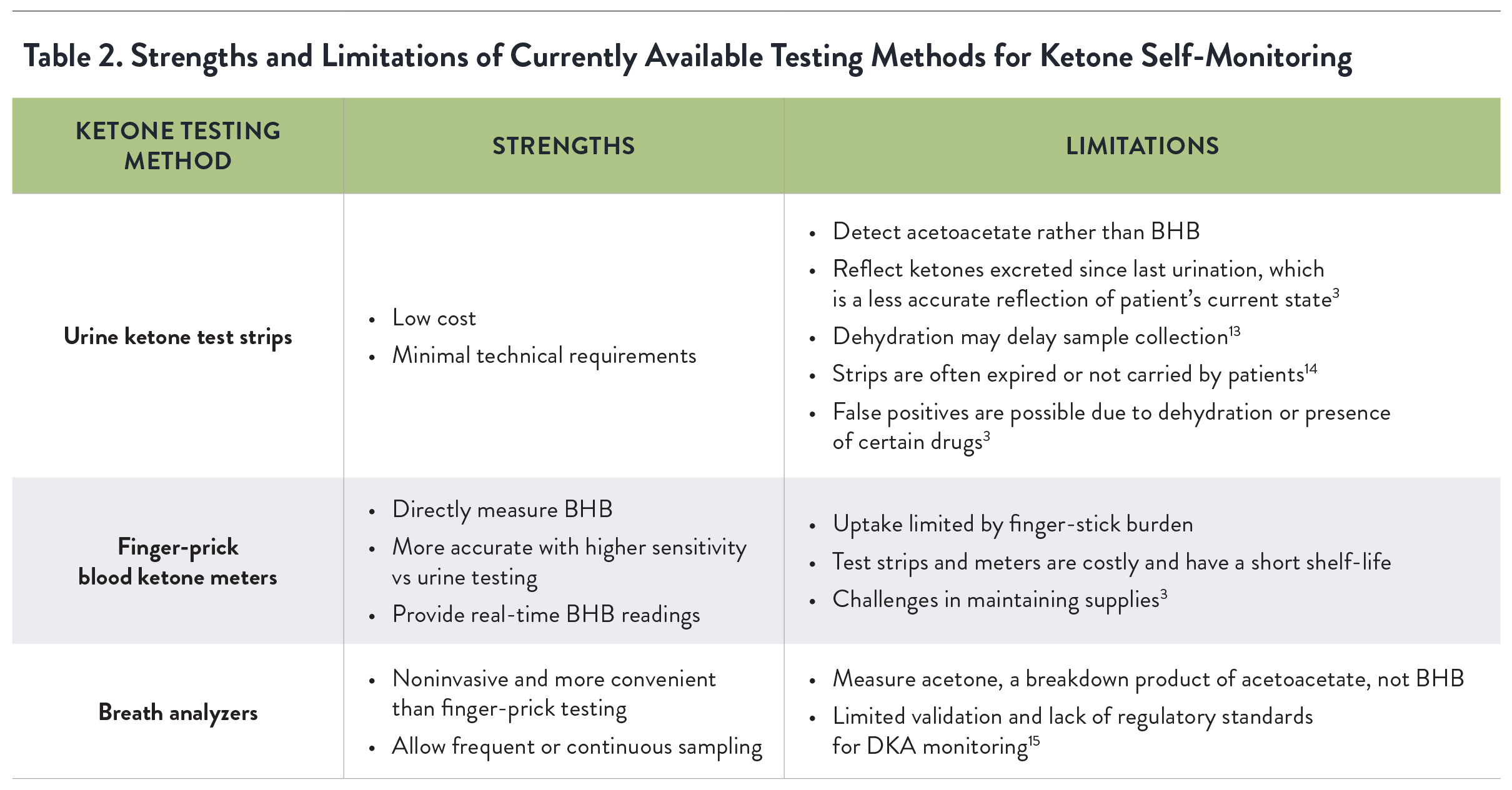
WHY TODAY’S KETONE TESTING FALLS SHORT
 In practice, ketone testing is often sporadic and delayed because patients may not test unless prompted by severe symptoms or explicit provider instructions. These challenges are reflected in population-level data: a survey of 2,995 people with T1D in the United States found that 32% had no urine or blood ketone testing materials at home, only 21% checked ketones when nauseated or vomiting, and only 18% had a blood ketone meter.3,16 Clinically, providers often lack timely visibility into ketone levels unless patients report them directly, which typically occurs only after ongoing ketosis or following a DKA event, limiting the window for outpatient course-correction.17
In practice, ketone testing is often sporadic and delayed because patients may not test unless prompted by severe symptoms or explicit provider instructions. These challenges are reflected in population-level data: a survey of 2,995 people with T1D in the United States found that 32% had no urine or blood ketone testing materials at home, only 21% checked ketones when nauseated or vomiting, and only 18% had a blood ketone meter.3,16 Clinically, providers often lack timely visibility into ketone levels unless patients report them directly, which typically occurs only after ongoing ketosis or following a DKA event, limiting the window for outpatient course-correction.17
Storage conditions are another overlooked variable—strips are often kept in bathrooms and may degrade or expire unnoticed, producing unreliable results at critical times.18 False negatives may occur due to acidic urine from the ingestion of large quantities of ascorbic acid, while sulfhydryl drugs (eg, captopril) and highly colored urine from dehydration have been associated with false positives—both scenarios that can mislead clinical decision-making.18 Access barriers exacerbate the problem. Availability of blood ketone meters and strips may be inconsistent, particularly among underserved or high-risk populations, and research suggests low-income populations face significant barriers to diabetes technology access.19
Patient education and awareness around ketone monitoring remain limited, particularly in “sick day” education, which facilitates monitoring and insulin administration during illness or periods of stress when DKA risk increases sharply.5,15 Structured “sick day” protocols are intended to guide patients in proactive monitoring, hydration, and supplemental insulin dosing when febrile or unable to eat normally. However, these protocols may be undertaught, inconsistently reinforced, or forgotten over time.10 For adolescents and young adults striving for normalcy while managing T1D, every DKA episode can serve as a pivotal touchpoint for re-engagement. Coordinated follow-up and education at these inflection points can reduce readmissions and alter long-term disease trajectories—delivering both clinical and economic value across care systems.
 The widespread adoption of CGMs has demonstrated how continuous data can catalyze timely actions and prevent costly complications through trend-based alerts and remote oversight.2 Without routine ketone tracking, the opportunity to intervene in the early stages of DKA may be missed. Thus, the current landscape reflects a significant monitoring gap that undermines timely intervention and DKA prevention efforts.
The widespread adoption of CGMs has demonstrated how continuous data can catalyze timely actions and prevent costly complications through trend-based alerts and remote oversight.2 Without routine ketone tracking, the opportunity to intervene in the early stages of DKA may be missed. Thus, the current landscape reflects a significant monitoring gap that undermines timely intervention and DKA prevention efforts.
CONTINUOUS KETONE MONITORING: A NEW FRONTIER
CKM represents a new form of ketone testing technology designed to identify changing ketone levels and alert to significant changes in real time, enabling action before metabolic instability consolidates into DKA.13 CKM sensor technology is based on the continuous detection of interstitial ketone body concentrations, namely BHB, and can utilize similar sensing platforms to existing glucose monitoring devices, simplifying integration for patients and providers familiar with CGM workflows.13
The feasibility of CKM technology using BHB was established in a 2021 study in 12 healthy participants on low-carbohydrate diets, who wore three ketone sensors on the back of their upper arms to continuously measure ketone levels over 14 days.17 The sensor was found to be stable and capable of continuously tracking ketones with a single calibration through the entire 14 days of wear.17
Development of CKM technology has progressed toward integrated, dual-analyte sensors designed to measure both glucose and BHB continuously, and in real time. One such device is planned to connect to personal and caregiver mobile apps and cloud-based data management software for provider remote monitoring, leveraging established digital ecosystems to facilitate coordinated responses.20 The bio-wearable device builds on the infrastructure and clinical acceptance of CGMs and offers a streamlined method of monitoring two critical metabolic markers within a single platform.20 In 2021, the device received Breakthrough Device designation from the US Food and Drug Administration (FDA), signaling regulatory recognition of its potential to address a significant unmet clinical need.20
FROM CRISIS RESPONSE TO PROACTIVE PREVENTION
 CKM offers a paradigm shift from managing diabetes focused solely on glucose, reframing risk assessment to include dynamic ketone trajectories that better predict impending metabolic decompensation.13 By providing constant data on ketone levels, CKM enables patients and providers to identify rising trends before they progress into full DKA. Early recognition and alerting can prompt self-correction via insulin titration and hydration or trigger timely clinical intervention that averts emergency care and hospitalization.14 CGM may offer a persuasive analogy: just as continuous glucose data transformed care delivery and reduced acute-care costs, CKM could yield comparable system-level benefits as supporting evidence expands.21
CKM offers a paradigm shift from managing diabetes focused solely on glucose, reframing risk assessment to include dynamic ketone trajectories that better predict impending metabolic decompensation.13 By providing constant data on ketone levels, CKM enables patients and providers to identify rising trends before they progress into full DKA. Early recognition and alerting can prompt self-correction via insulin titration and hydration or trigger timely clinical intervention that averts emergency care and hospitalization.14 CGM may offer a persuasive analogy: just as continuous glucose data transformed care delivery and reduced acute-care costs, CKM could yield comparable system-level benefits as supporting evidence expands.21
CKM, particularly when combined with CGM, offers another layer of DKA risk mitigation across several high-risk scenarios. Priority use cases include individuals with T2D using SGLT2 inhibitors; those with a prior history of DKA or repeated episodes; people adopting very low-carbohydrate or ketogenic diets; patients engaging in periods of high-intensity exercise; individuals during illness or perioperative fasting for procedures; pregnant women with pregestational diabetes; elderly individuals; and patients who are socially and geographically isolated, for whom prompt in-person evaluation may be delayed.3,13 For patients at a high risk of developing DKA, CKM has the potential to reduce emergency department visits, prevent hospital admissions, and generate meaningful cost savings at the population level.22
A 2022 review highlighted how CKMs could enhance care delivery, including strengthening sick-day protocols, enabling earlier outpatient intervention, supporting post-discharge follow-up, and informing decisions in both inpatient and ambulatory settings.18 In the emergency department, CKM could shorten diagnostic delays by identifying rising ketone trends before laboratory confirmation is available, enabling earlier initiation of insulin therapy and fluid resuscitation.18 In the inpatient setting, real-time BHB trajectories could help providers distinguish true treatment failure and DKA resolution from the misleading “paradoxical increase” in urine acetoacetate that sometimes occurs during DKA resolution, preventing unnecessary insulin escalation and subsequent hypoglycemia.18
Perioperatively, CKM could allow anesthesiologists and surgical teams to detect stress-induced ketonemia, which contributes to elevated rates of morbidity and mortality in people with diabetes following emergency surgery, to help guide early intervention.18 CKM could also offer assurance during perioperative fasting and after bariatric surgery, where postoperative DKA is a recognized complication, particularly among patients taking SGLT2 inhibitors or with poor preoperative glycemic control.18 In pediatrics, where DKA is associated with high morbidity, continuous ketone data could enhance therapeutic precision and mitigate risks such as cerebral edema, the most common cause of death in pediatric patients with DKA.18
 Beyond acute care, CKM has important implications for transitional and preventive medicine. Recently discharged patients with recurrent DKA, postbariatric surgery patients, or those in long-term care facilities could be monitored remotely, with CKM data shared directly with providers or caregivers. This proactive surveillance may reduce avoidable readmissions, align with value-based care initiatives, and improve quality of life for high-risk patients. To maximize its utility, providers should view CKM data not only as a diagnostic adjunct, but also as a continuous stream of actionable information—capable of guiding real-time interventions, refining treatment algorithms, and transforming care across the continuum of diabetes management.18
Beyond acute care, CKM has important implications for transitional and preventive medicine. Recently discharged patients with recurrent DKA, postbariatric surgery patients, or those in long-term care facilities could be monitored remotely, with CKM data shared directly with providers or caregivers. This proactive surveillance may reduce avoidable readmissions, align with value-based care initiatives, and improve quality of life for high-risk patients. To maximize its utility, providers should view CKM data not only as a diagnostic adjunct, but also as a continuous stream of actionable information—capable of guiding real-time interventions, refining treatment algorithms, and transforming care across the continuum of diabetes management.18
FROM EVIDENCE TO IMPLEMENTATION
The clinical value of blood ketone monitoring in T1D has been well established for decades. A 2006 study in pediatric and young adult T1D patients found that sick-day management using BHB monitoring resulted in significantly higher ketone testing adherence and a reduced rate of hospitalizations and emergency assessments compared to traditional urine ketone testing, validating BHB-based strategies as both clinically effective and patient acceptable.23 These findings support the clinical utility and patient acceptability of CKM as a more effective strategy for mitigating the risk of DKA and associated healthcare utilization.23
Importantly, CKM may also play a role in expanding the use of SGLT2 inhibitors to patients with T1D. Though beneficial in T1D, agents from the SGLT2 class have failed to gain FDA approval to treat T1D due to the increased risk of DKA.3 Continuous safety monitoring could provide a framework for safer deployment in selected patients under protocolized oversight, pending supportive evidence.3
The feasibility of a CKM device has been demonstrated, though optimization is still underway, particularly regarding sensor accuracy across physiologic ranges, calibration routines, and wearability in diverse settings.3 More studies are needed to confirm that CKM systems deliver accurate data and that their use improves clinical outcomes by aiding in the prediction and prevention of metabolic decompensation in diabetes.15
Recent publications also highlight the potential value of continuous dual glucose–ketone monitoring systems that measure both glucose and BHB on a single platform. Such systems may enable earlier detection of ketosis, including situations where diabetic ketoacidosis develops without marked hyperglycemia (eg, euglycemic DKA associated with SGLT2 inhibitors).24 Costs and physical burden to the patient can be minimized by combining ketone sensing with the measurement of glucose as part of a single platform and integrating CKM data into existing care management systems, thereby streamlining workflows and payer coverage pathways.3
Integration of continuous glucose and ketone sensing may also enhance automated insulin delivery systems. Current algorithms primarily rely on glucose sensor data, but incorporation of ketone detection could enable earlier alerts and algorithm adjustments in response to rising ketone levels, potentially allowing earlier intervention to prevent progression to DKA.24
Because these devices should be able to predict an impending increase in ketone levels, alerts delivered via wireless transmission could lead to nurse-led outreach or virtual visits, enhancing the patient-provider collaborative model and improving outcomes through timely, protocol-driven responses.15
GAPS, CHALLENGES, AND EQUITY CONSIDERATIONS
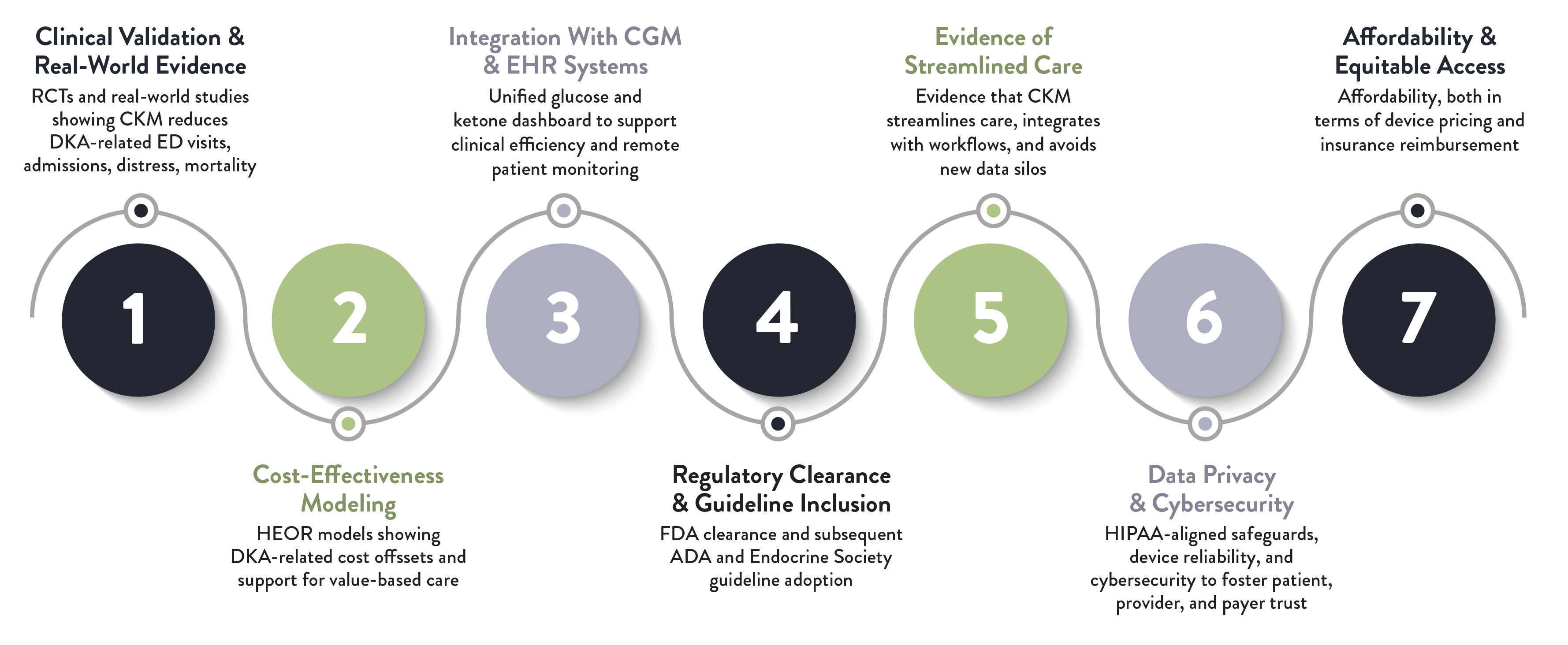
For widespread adoption of CKM systems by both providers and payers, several elements must be addressed in a deliberate, evidence-first roadmap:
-
Clinical validation and real-world evidence: Clinicians will require robust randomized clinical trials and large-scale real-world studies demonstrating that CKM reduces DKA-related emergency visits, diabetes distress, admissions, and mortality, similar to the trajectory by which CGM earned guideline endorsement. Without this evidence base, guidelines such as those from the ADA and Endocrine Society are unlikely to recommend routine use, and payers will be reluctant to cover the technology.
-
Cost-effectiveness analyses: Payers may seek clear evidence of cost-effectiveness, showing that CKM use can prevent costly acute events, including DKA readmissions, and support value-based care initiatives. Cost modeling and health economic analyses—similar to those performed for CGM—will need to establish that upfront investment in CKM devices offsets downstream utilization costs.
-
Seamless integration with existing CGM platforms and electronic health records: The ability for providers to view ketone and glucose data alongside other physiologic metrics in a consolidated dashboard may simplify management of ketone levels before the condition progresses to DKA and may support clinical efficiency and remote patient monitoring.
-
Regulatory clearance and guideline inclusion: FDA clearance based on clinical validation is the entry point; however, subsequent incorporation by the ADA and Endocrine Society may catalyze clinical trust and payer coverage, just as ADA recommendations and Centers for Medicare & Medicaid Services (CMS) coverage decisions helped accelerate CGM adoption.
-
Evidence of streamlined care: Providers may also seek evidence that CKM streamlines care rather than creates parallel data silos, and that it integrates with telehealth and remote patient monitoring opportunities to strengthen reimbursable workflows.
-
Data privacy and cybersecurity: From a system design perspective, CKMs should be user-friendly, durable, and cybersecure to ensure patient trust and protect sensitive health information. Both providers and payers may demand clear safeguards to comply with the Health Insurance Portability and Accountability Act (HIPAA) and maintain patient trust.
-
Affordability and equitable access: Finally, affordability, both in terms of device pricing and insurance reimbursement, will be critical to broad uptake and to avoid widening disparities in diabetes technology access.15
ENTERING A NEW FRONTIER IN REAL-TIME DIABETES SAFETY
Preventing DKA remains one of the most urgent challenges in diabetes care, both for patient safety and for controlling costs. CKM addresses this gap by enabling earlier detection of metabolic instability and creating the potential to reduce hospitalizations. Even a modest reduction in DKA-related admissions could generate substantial savings for health plans, particularly those managing large populations with T1D. CKM may also expand the use of certain medications, such as SGLT2 inhibitors for the T1D population, by ensuring safe monitoring of onset of DKA.
A new consensus opinion on the use of novel CKM technologies in the care of people with diabetes has been published in the January 2026 issue of The Lancet Diabetes & Endocrinology by a panel of international experts in the management of DKA.25 These recommendations have been endorsed by the International Society for Pediatric and Adolescent Diabetes (ISPAD) and are available online.
The expert panel notes that although ketone self-testing is recommended during periods of increased risk, many individuals with diabetes do not routinely measure ketones and may be uncertain how to respond when levels rise.25 The consensus report provides practical recommendations for the clinical application of CKM to reduce the risk of DKA. The panel notes that CKM could provide users with immediate feedback on rising BHB concentrations, enabling earlier recognition of ketosis and prompting timely intervention before progression to DKA. To support consistent interpretation of CKM data, the group recommends standardized ketone thresholds linked to clinical action: normal (<0.6 mmol/L), elevated (0.6–1.5 mmol/L), high (>1.5 to <3.0 mmol/L), and urgent high (≥3.0 mmol/L). These thresholds are intended to guide patient self-management and clinician response, with urgent high ketone levels prompting immediate medical evaluation.25
The report also emphasizes the importance of clinical education, standardized alert thresholds, and integration of CKM data into routine diabetes management workflows to ensure safe and effective use of this emerging technology. In addition, the report emphasizes that CKM may help identify individuals at heightened risk of recurrent DKA and support earlier preventive interventions across high-risk populations, including those using insulin pump therapy or SGLT2 inhibitors.25
Beyond immediate cost savings, CKM supports payer priorities by reducing avoidable emergency utilization, improving quality metrics, and advancing value-based care initiatives. By shifting management from reactive crisis response to proactive, real-time monitoring, CKM fosters earlier intervention, stronger patient engagement, and long-term system sustainability. More than an incremental innovation, CKM offers a population-level advancement capable of reshaping outcomes, lowering costs, and setting a new standard for real-time diabetes safety.
REFERENCES
- Ramphul K, Joynauth J. An update on the incidence and burden of diabetic ketoacidosis in the U.S. Diabetes Care. 2020;43(12):e196-e197. doi:10.2337/dc20-1258
- Virdi N, Poon Y, Abaniel R, Bergenstal RM. Prevalence, cost, and burden of diabetic ketoacidosis. Diabetes Technol Ther. 2023;25(S3):S75-S84. doi:10.1089/dia.2023.0149
- Kong YW, Morrison D, Lu JC, Lee MH, Jenkins AJ, O'Neal DN. Continuous ketone monitoring: exciting implications for clinical practice. Diabetes Obes Metab. 2024;26 Suppl 7(Suppl 7):47-58. doi:10.1111/dom.15921
- Dovc K, Neuman V, Gita G, et al. Association of diabetic ketoacidosis at onset, diabetes technology uptake, and clinical outcomes after 1 and 2 years of follow-up: a collaborative analysis of pediatric registries involving 9,269 children with type 1 diabetes from nine countries. Diabetes Care. 2025;48(4):648-654. doi:10.2337/dc24-2483
- Li L, Andrews EB, Li X, et al. Incidence of diabetic ketoacidosis and its trends in patients with type 1 diabetes mellitus identified using a U.S. claims database, 2007-2019. J Diabetes Complications. 2021;35(7):107932. doi: 10.1016/j.jdiacomp.2021.107932
- Misra S. Rise in diabetic ketoacidosis during the COVID-19 pandemic: several questions remain. Lancet Diabetes Endocrinol. 2022;10(11):763-765. doi:10.1016/S2213-8587(22)00272-8
- Cao S, Cao S. Diabetic ketoalkalosis: a common yet easily overlooked alkalemic variant of diabetic ketoacidosis associated with mixed acid-base disorders. J Emerg Med. 2023;64(3):282-288. doi:10.1016/j.jemermed.2022.12.023
- Umpierrez GE, Davis GM, ElSayed NA, et al. Hyperglycemic crises in adults with diabetes: a consensus report. Diabetes Care. 2024;47(8):1257-1275. doi:10.2337/dci24-0032
- Gill VJS, Govekar S, Soni S, Grover A, Shekhar S. Trends and disparities in DKA-related mortality in the United States (1999-2022): insights from the CDC WONDER database. J Endocr Soc. 2025;9(Suppl 1):A622
- Kreider KE. Updates in the management of diabetic ketoacidosis. J Nurse Pract. 2018;14(8):591-597. doi:10.1016/j.nurpra.2018.06.013
- American Diabetes Association Professional Practice Committee. 6. Glycemic goals and hypoglycemia: standards of care in diabetes—2025. Diabetes Care. 2025;48(1 Suppl 1):S128-S145. doi:10.2337/dc25-S006
- Centers for Disease Control and Prevention. Diabetic ketoacidosis. Published May 15, 2024. Accessed October 20, 2025. https://www.cdc.gov/diabetes/about/diabetic-ketoacidosis.html
- Huang J, Yeung AM, Bergenstal RM. Update on measuring ketones. J Diabetes Sci Technol. 2024;18(3):714-726. doi:10.1177/19322968231152236
- Lee MH, Paldus B, Krishnamurthy B, et al. The clinical case for the integration of a ketone sensor as part of a closed loop insulin pump system. J Diabetes Sci Technol. 2019;13(5):967-973. doi:10.1177/1932296818822986
- Nguyen KT, Xu NY, Zhang JY, et al. Continuous ketone monitoring consensus report 2021. J Diabetes Sci Technol. 2022;16(3):689-715. doi:10.1177/19322968211042656
- Albanese-O'Neill A, Wu M, Miller KM, et al; T1D Exchange Clinic Network. Poor adherence to ketone testing in patients with type 1 diabetes. Diabetes Care. 2017;40(4):e38-e39. doi:10.2337/dc16-2620
- Alva S, Castorino K, Cho H, Ou J. Feasibility of continuous ketone monitoring in subcutaneous tissue using a ketone sensor. J Diabetes Sci Technol. 2021:15(4):768-774. doi:10.1177/19322968211008185
- Jaromy M, Miller JD. Potential clinical applications for continuous ketone monitoring in the hospitalized patient with diabetes. Curr Diab Rep. 2022;22(10):501-510. doi:10.1007/s11892-022-01489-6
- Fallon C, Jones E, Oliver N, Reddy M, Avari P. The impact of socio-economic deprivation on access to diabetes technology in adults with type 1 diabetes. Diabet Med. 2022:39(10):e14906. doi:10.1111/dme.14906
- Abbott. Abbott Announces Development of Novel Continuous Glucose-Ketone Monitoring System. Press release. Published June 3, 2022. Accessed October 8, 2025. https://abbott.mediaroom.com/2022-06-03-Abbott-Announces-Development-of-Novel-Continuous-Glucose-Ketone-Monitoring-System
- Norman GJ, Fernandes J, Nemlekar P, Andrade SB, Lupton L, Berk A. Initiating continuous glucose monitoring is associated with improvements in glycemic control and reduced health care resource utilization for people with diabetes in a large US-insured population: a real-world evidence study. J Manag Care Spec Pharm. 2025;31(1):15-24. doi:10.18553/jmcp.2024.24255
- Zhang JY, Shang T, Koliwad SK, Klonoff DC. Continuous ketone monitoring: a new paradigm for physiologic monitoring. J Diabetes Sci Technol. 2021;15(4):775-780. doi:10.1177/19322968211009860
- Laffel LM, Wentzell K, Loughlin C, Tovar A, Moltz K, Brink S. Sick day management using blood 3-hydroxybutyrate (3-OHB) compared with urine ketone monitoring reduces hospital visits in young people with T1DM: a randomized clinical trial. Diabet Med. 2006;23(3):278-284. doi:10.1111/j.1464-5491.2005.01771.x
- Garg SK, Parkin CG. Role of Continuous Dual Glucose-Ketone Monitoring in Diabetes Care. Diabetes Technol Ther. 2025;27(S4):S1-S5. doi: 10.1177/15209156251369529. PMID: 41267373
- Dhatariya K, Bergenstal RM, Al-Sofiani M, et al. Continuous ketone monitoring for people with diabetes: international expert recommendations on the application of a new technology. Lancet Diabetes Endocrinol. 2026;14(1):82-92
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of First Report Managed Care or HMP Global, their employees, and affiliates.



