Balloon Aortic Valvuloplasty via Umbilical Venous Access in a Neonate With Critical Aortic Stenosis
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
A 5-day-old neonate was referred to our tertiary care center for evaluation of respiratory distress and a systolic murmur at the right second parasternal space. On presentation, the neonate was tachypneic with a respiratory rate of 36 breaths per minute. Two-dimensional transthoracic echocardiography was suggestive of bicuspid aortic valve with critical aortic stenosis (restricted opening) with a peak aortic gradient of 40 mm Hg and good left ventricle function.
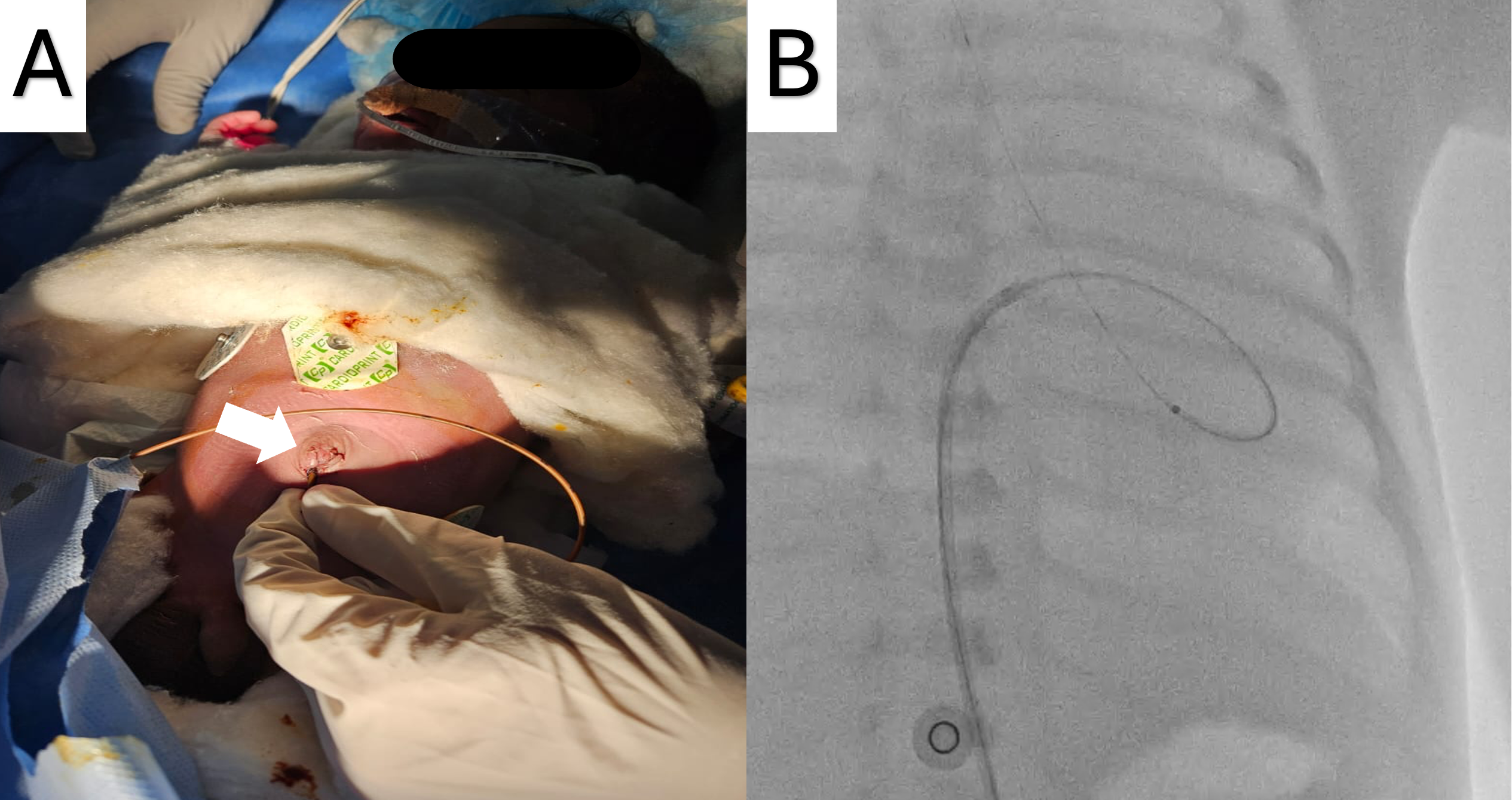
After obtaining informed consent from the parents, the neonate was planned for balloon aortic valvuloplasty (BAV) via the umbilical vein, which had been preserved by inserting a small 4F catheter (Figure A). A 0.014-inch regular workhorse percutaneous transluminal coronary angioplasty (PTCA) wire was inserted and advanced via the umbilical vein through the ductus venosus into the inferior vena cava to the right atrium (RA) (Video 1). Because of a lack of wire support, further advancement was not possible without catheter assistance. A 4F catheter was upgraded to a 5F sheath and a 5F right coronary artery catheter was advanced until it reached the RA. The wire was then manipulated and advanced into the left atrium and subsequently into the left ventricle (LV) through the patent foramen ovale (Video 2). An attempt to cross the aortic valve (AV) with the wire failed because of inadequate support. A Renegrade microcatheter (Boston Scientific) was introduced into the LV (Figure B); the AV was successfully crossed and the PTCA wire was parked in the descending aorta (Video 3). Following microcatheter removal, BAV was performed traditionally with a 4 x12-mm coronary angioplasty balloon, as the annulus measured approximately 6 mm. The post-procedural echocardiographic peak gradient was 18 mm Hg, and the procedure time lasted approximately 1 hour. The plan was to do a repeat BAV from the femoral route 1 month post-procedure.
We describe a technically challenging BAV performed through the umbilical venous route in a 5-day-old neonate presenting with critical aortic stenosis. Although femoral arterial access remains standard, umbilical venous access may serve as a viable route in select patients where arterial access is preserved for future interventions. The coronary microcatheter facilitated crossing the aortic valve, highlighting the importance of a thorough understanding of guidewires and accessories while performing complex structural interventions.
Affiliations and Disclosures
Sanjeev Kathuria, MD, DM1; Sourabh Agstam, MD, DM2; Sumod Kurien, MD, DM1
From the 1Department of Cardiology, Govind Ballabh Pant Hospital, New Delhi, India; 2Department of Cardiology, All India Institute of Medical Sciences, New Delhi, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient’s guardian for the intervention described in the manuscript and for the publication thereof, including photographs.
Address for correspondence: Sanjeev Kathuria, Department of Cardiology, Govind Ballabh Pant Hospital, New Delhi 110002, India. Email: sanjeevkath@hotmail.com; X: @Agstamsourabh