


Right Coronary Artery Takeoff Plane and Implications for Brachiocephalic Interventions and Next Generation Transcatheter Aortic Valve Intervention Embolic Protection Devices
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Objectives. The authors hypothesized that the origin of the right coronary artery (RCA) is a direct continuation of the major aortic arch branches (MAAB) takeoff plane, which may have implications for brachiocephalic interventions and next generation transcatheter aortic valve intervention (TAVI) embolic protection devices (EPDs).
Methods. In this single-center, retrospective, cross-sectional study, the authors analyzed computed tomographic angiography (CTA) images from 92 patients undergoing TAVI evaluation to determine the spatial relationship between the origin of the RCA and the MAAB takeoff plane. Patients with prior cardiothoracic or aortic interventions and those with anomalous RCA origin were excluded. Using double oblique imaging planes, the authors assessed whether the RCA and MAAB takeoffs were visualized within the same sagittal plane.
Results. The mean age of the patients was 76.4 years; 52% were female. Most patients had hypertension (90%), coronary artery disease (65%), or a history of smoking (47%). The RCA origin aligned with the forward and downward continuation of the MAAB plane in 77.1% of the patients.
Conclusions. This novel anatomical relationship, not previously described in literature, may be clinically useful during cardiac catheterization when cannulating brachiocephalic vessels to visualize right and left internal mammary arteries and during brachiocephalic interventions such as subclavian and carotid stenting. Additionally, the findings suggest that some third generation TAVI EPDs with anchoring probes resting in the aortic root may lie in close proximity to the RCA ostium. This proximity could hinder urgent RCA cannulation during TAVI procedures. As new EPD designs gain traction globally, it is essential for TAVI operators to understand this anatomical nuance.
Introduction
We previously demonstrated that the major aortic arch branches (MAAB) are narrowly aligned along a curvilinear plane traversing the superior-most aspect of the greater aortic curvature.1 During coronary procedures using the femoral approach (FA), the frequent inadvertent cannulation of the right brachiocephalic artery (RBCA) by the disengaged 3-dimensional (3D) right coronary artery (RCA) catheter2 led us to hypothesize that the normal RCA origin is aligned along a continuation of the aforementioned MAAB takeoff plane. We further hypothesized that this RCA origin plane gradually swings anteriorly and downwards in the ascending aorta, culminating at the anterior-most aspect of the aortic root, namely, the right aortic cusp that usually houses the RCA origin. This anatomic relationship is already used by cardiologists to engage the MAAB when visualization of right or left internal mammary arteries (RIMA, LIMA) is needed and during subclavian and carotid interventions.
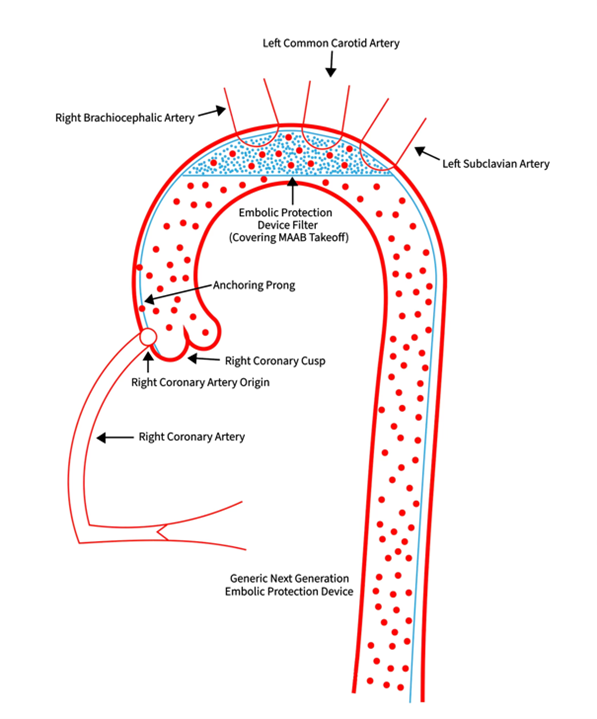
With expanding transcatheter aortic valve implantation (TAVI) indications, post-intervention cerebrovascular accidents (CVA) remain a significant concern.3 To mitigate this risk, 1 distal embolic protection device (EPD) (Sentinel, Boston Scientific) has been approved for use in the United States, and several more are undergoing various stages of development and approval. Some of the third generation TAVI EPDs in use outside the United States and currently in trials in the United States use centrifugal forces to ensconce the filter against the greater aortic curvature, thereby covering the takeoff plane of the major aortic arch branches. The device’s anchoring probe extends forward and downward, ending in the aortic root (Figure 1). Based on our findings, we suspect that this probe should be in close proximity to the RCA origin. Thus, the objective of this study was to determine if the RCA takeoff is in the same plane as the takeoff plane of the MAAB.
Methods
This was a single-center, retrospective, cross-sectional study. All patients aged 18 years or older who presented to the Newark Beth Israel Medical Center from July 2022 to April 2023 for TAVI workup were considered for the study. Computed tomography of the chest, abdomen, and pelvis was performed as per TAVI protocol. Patients with any prior cardiothoracic or aortic interventions and those with anomalous RCA origin were excluded.
Ethical approval for this study was waived by the institutional review board (IRB) at Newark Beth Israel Medical Center, as this was a retrospective study with evaluation of imaging and demographic data (IRB approval #2024.11). No drugs or interventions were used, and patients were de-identified. Investigators were blinded during analysis. The requirement to obtain written informed consent was waived by the IRB because this study was a retrospective data review and the standard of care was not altered—patients had already undergone the imaging as part of TAVI workup.
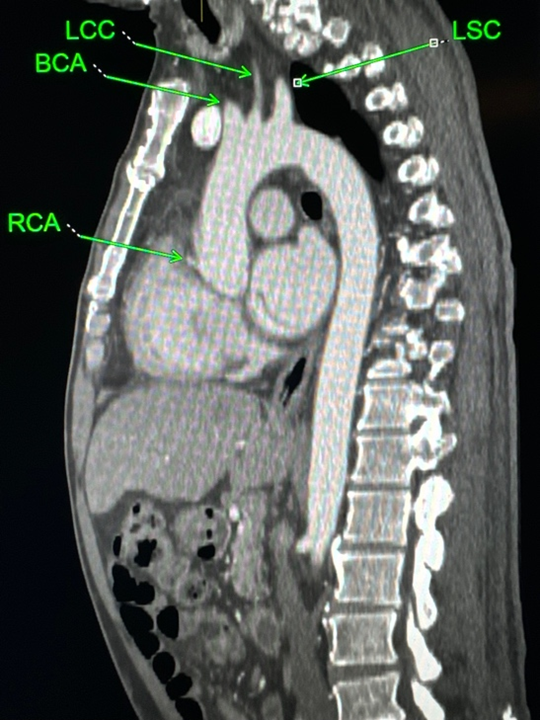
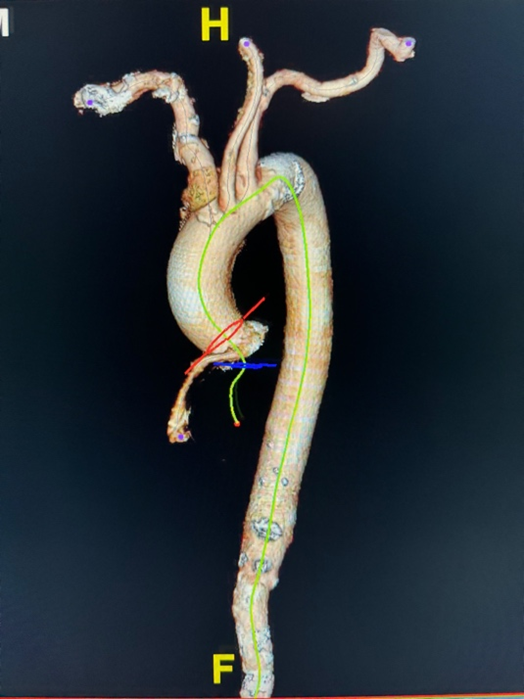
Chest computed tomographic angiography (CTA) images (TAVI protocol) were used to form a double oblique plane using free manipulation of the standard axial, coronal, and sagittal planes. We started in the standard axial plane at the aortic root approximately at the level of the RCA takeoff. Then, we used the coronal plane to tilt the axial plane approximately parallel to the aortic annulus. Next, we adjusted the new oblique axial and coronal planes to visualize the MAAB and RCA takeoffs in the oblique sagittal plane. Cases were considered positive when the MAAB and RCA takeoffs were identified in same oblique sagittal plane (Figures 2 and 3).
Statistical analysis
Data were collected and stored in Microsoft Excel. Statistical analysis was performed using SPSS (IBM) to assess the frequency of patients showing RCA and MAAB takeoff in the same plane. Demographic data were similarly stored, and all results are presented in the Table.
Results
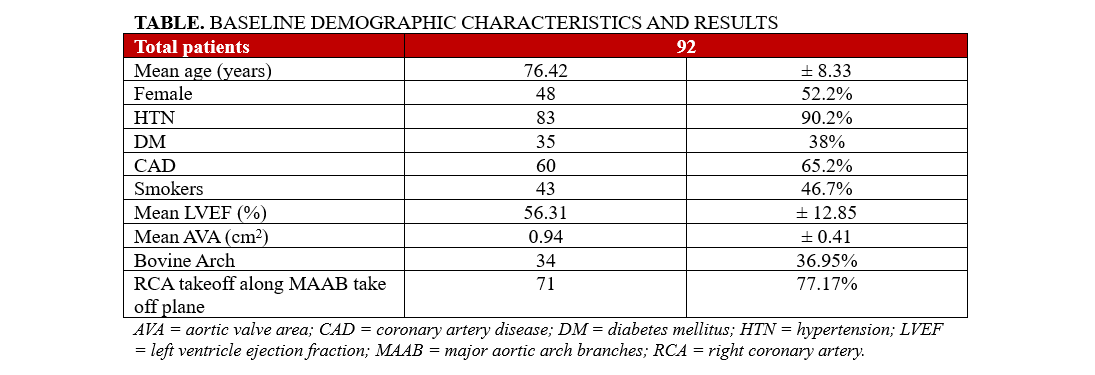
The mean age of the 92 patients with complete data was 76.4 years. Among them, 48 (52%) were female and 44 (48%) were male. Hypertension was present in 83 patients (90%), diabetes in 35 (38%), and coronary artery disease in 60 (65%). Additionally, 43 (46.7%) were current or former smokers. The mean left ventricular ejection fraction was 56%, and the mean aortic valve area was 0.9 cm². Thirty-four patients (37%) had bovine aortic arch. A total of 71 (77.1%) of the 92 patients had the RCA origin along the forward and downward extension of the MAAB takeoff plane.
Discussion
We have previously demonstrated that the MAAB are aligned along a plane traversing the superior-most aspect of the transverse aorta. Our current findings highlight a significant anatomical relationship (hitherto not described in literature) between the RCA takeoff and the forward and downward extension of the MAAB takeoff plane. Specifically, in 77.1% of the patients, the RCA takeoff plane aligned with the forward and downward extension of the MAAB takeoff plane.
An upwardly pointing 3D RCA catheter withdrawn gently along the ascending aorta to the transverse aorta has been shown to seamlessly engage the right brachiocephalic artery2 and is already in use by cardiologists for cannulating these vessels when performing brachiocephalic interventions like subclavian and carotid stenting. In addition, when such cannulation is required during cardiac catheterization procedures to visualize RIMA or LIMA bypass grafts, based on our findings, the simple withdrawal of the 3D RCA Catheter from the RCA will usually land the catheter in the right brachiocephalic artery, the left common carotid artery, and the left subclavian artery sequentially.
This takeoff plane alignment may also have practical implications when third generation TAVI EPDs with an aortic root anchoring probe are used to prevent periprocedural stroke because the anchoring probe of such devices will likely settle close to the RCA origin and pose an impediment to urgent RCA cannulation. TAVI operators need to be mindful of this anatomical relationship.
Limitations
This study is limited by its single-center design and relatively small sample size. Larger studies are needed to corroborate our findings.
Conclusions
We conclude that the RCA takeoff plane is aligned with the forward and downward extension of the MAAB takeoff plane. This knowledge can help operators during brachiocephalic and carotid interventions. Additionally, this relationship may pose an impediment to urgent RCA cannulation (if it becomes necessary) when third generation embolic protection devices with an aortic root anchoring probe are employed.
Affiliations and Disclosures
Umair Bajwa, MD; Mohammad Chaudhry, MD; Danielle Retcho, MD; Sohira Idrees, BA; Lukasz Partyka, MD; Rajiv Tayal, MD; Arash Salemi, MD; Sergio Waxman, MD; Najam Wasty, MD
From the Newark Beth Israel Medical Center, Newark, New Jersey.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Umair Bajwa, MD, Newark Beth Israel Medical Center, Newark, NJ 07112, USA. Email: umairbajwadr@gmail.com, X: @UmairBajwaMD
References
- Tayal R, Khakwani MZ, Lesar B, et al. Takeoff orientation of the major aortic arch branches irrespective of arch type: ramifications for brachiocephalic interventions including carotid stenting. SAGE Open Med. 2018;6:2050312118776717. doi:10.1177/2050312118776717
- Wasty N, Abidi M, Tanwir A, et al. Feasibility of the 3D RCA catheter to engage the brachiocephalic vessels during carotid angiography and stenting. Catheter Cardiovasc Interv. 2011;77(5):742-745. doi:10.1002/ccd.22762
- Okuno T, Alaour B, Heg D, et al. Long-term risk of stroke after transcatheter aortic valve replacement: insights from the SwissTAVI registry. JACC Cardiovasc Interv. 2023;16(24):2986-2996. doi:10.1016/j.jcin.2023.10.021











