


Plug-Based Vascular Closure Device in Transfemoral Transcatheter Aortic Valve Implantation
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Objectives. Failure of vascular closure device (VCD) is the most common cause of access-site vascular complications in transfemoral transcatheter aortic valve implantation (TAVI). The authors sought to determine if the systematic use of arteriotomy-site ballooning with concomitant manual compression following the delivery of a plug-based VCD (MANTA, Teleflex) can optimize toggle-plug assembly apposition to the common femoral artery (CFA) wall and improve the final hemostatic efficacy.
Methods. In this prospective, observational, single-center study, 323 consecutive patients undergoing transfemoral TAVI from October 2021 to December 2024 underwent access closure with the MANTA VCD. The primary endpoints were VCD failure rate, predictors of VCD failure, and access-site and access-related major and minor vascular complications, according to the Valve Academic Research Consortium-3 definition.
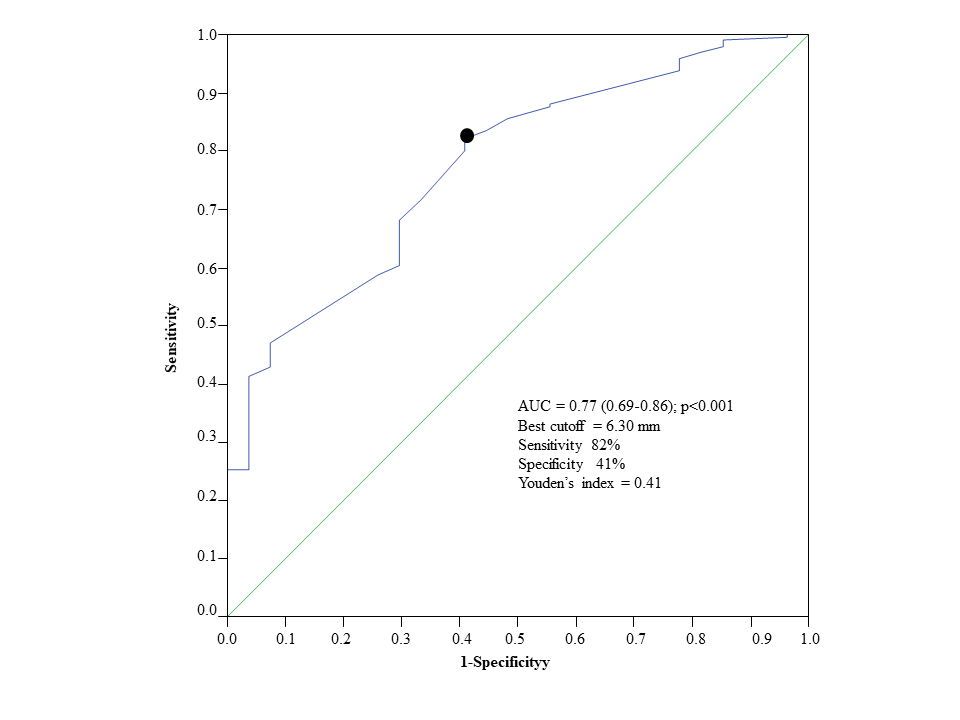
Results. VCD failure occurred in 12 (3.7%) patients (Failure group). The independent predictors of failure were minimum CFA diameter and patient risk as assessed by the Society of Thoracic Surgeons Predicted Risk of Mortality score. Receiver operating characteristic analysis showed CFA minimum diameter with an area under the curve of 0.77 (0.69-0.86, P < .001); the best cutoff was 6.30 mm (sensitivity 83%; specificity 59%; positive predictive value 7%; negative predictive value 99%). Access-site vascular complications occurred in 21 (6.5%) patients.
Conclusions. The systematic use of arteriotomy-site ballooning plus concomitant manual compression following MANTA VCD delivery should be considered to improve the final hemostatic efficacy. This device should be avoided when dealing with small (< 6.3 mm) CFA diameters.
Introduction
Although the incidence of access-site vascular complications has decreased over time, they remain a major issue in patients undergoing transfemoral transcatheter aortic valve implantation (TAVI).1 Failure of vascular closure device (VCD) is the most common cause of access-site vascular complications.1,2 Currently, 2 different VCDs are available: 1) a suture-based VCD (ProGlide, Abbott) and 2) a plug-based VCD (MANTA, Teleflex). Despite previous promising results from observational and propensity-matched studies,3-10 successive data from randomized trials did not support the superiority of the MANTA VCD over the ProGlide VCD in limiting access-site vascular complications.11,12 The CHOICE-CLOSURE trial12 showed that the suture-based technique with 2 ProGlides plus the liberal (~60%) use of an additional small plug-based VCD (Angioseal, Terumo) was associated with a lower rate of access-site or access-related major and minor vascular complications compared with the plug-based technique. Notably, the observed 19.4% access-site or access-related major and minor vascular complications rate in the MANTA-VCD group was higher than expected (8% to 14.5%).3-5,13 Differences in patients’ risk profile, procedural and anatomic features (such as sheath-to-femoral artery ratio [SFAR], calcification, and tortuosity) and the sole use of the MANTA 18F may have played a role in the reported high complications rate.14
Incomplete apposition of the toggle-plug assembly has been proposed as a possible cause of failure of this device.15 Arteriotomy-site ballooning with concomitant manual compression could represent a valid strategy to optimize toggle and plug apposition to the common femoral artery (CFA) wall and enhance hemostatic efficacy. Thus, the aim of this study was to evaluate the safety and efficacy of this approach in a real-world cohort of patients undergoing transfemoral TAVI.
Methods
Study population
From October 4, 2021 to December 13, 2024, 323 consecutive patients undergoing transfemoral TAVI in the Mediterranea Cardiocentro (Naples, Italy) underwent access closure with the MANTA VCD. Patients were evaluated by the local multidisciplinary heart team and consented to data collection. TAVI was performed according to the current practice and recommendations.16 The main inclusion criteria were the presence of severe aortic stenosis and eligibility for percutaneous treatment through a transfemoral approach. The exclusion criteria were younger than 18 years, the inability to sign an informed consent for the procedure and data collection, the need for surgical access to the femoral artery, and a life expectancy of less than 2 years. Patients received one of the following self-expandable valves: the Evolut R (Medtronic), the Evolut PRO+ (Medtronic), or the ALLEGRA (New Valve Technology). Patients were pre-treated with aspirin (100 mg) and clopidogrel (75 mg) daily. If patients were not on dual antiplatelet therapy, a loading dose of clopidogrel (300 mg) was administered. Oral anticoagulants in patients with atrial fibrillation were interrupted at least 12 hours before the procedure and restarted thereafter. All data were prospectively collected and stored in an anonymized secured database. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the local Ethic Committee, and informed consent was obtained from the patients for the study described in the manuscript and to its publication, including all images.
Study procedure
All patients underwent pre-procedural planning with multi-slice computed tomography scanning. The OsiriX (Pixmeo) or 3mensio (Pie Medical) softwares were used to analyze the iliofemoral arterial tree. Main access features as minimal CFA diameter, calcifications, and distance between the skin and the expected CFA puncture site were collected.
The MANTA VCD is available in 14F and 18F versions for 14F to 18F and 18F to 24.5F outer diameter sheaths, respectively. The device deployment was performed according to the standard recommendations.4 After advancing an 0.018-inch wire and a 5F diagnostic catheter through the left radial artery (or contralateral femoral artery), the CFA puncture was carried out under road-mapping guide. After obtaining femoral artery access, all the patients received unfractionated heparin to achieve an activated clotting time (ACT) of greater than 250 seconds. Next, an 8F puncture location dilator (depth locator) was advanced to measure the arteriotomy depth (ie, the length of the subcutaneous track from the skin to the endovascular lumen). An arteriotomy depth of greater than or equal to 4.0 cm was considered high risk for vascular complications.17 At the end of the procedure, the operative sheath was exchanged for the dedicated MANTA VCD sheath to receive the toggle-plug assembly. The entire unit was then removed up to the selected arteriotomy depth and the puncture site was sandwiched between the toggle and plug, which were connected through a radiopaque stainless steel lock. The recommended “sandwiching” time was 60 seconds. During MANTA VCD deployment, the recommended target ACT is less than 250 seconds, and the systolic blood pressure should be less than 160 mm Hg. Heparin reversal with protamine was left to the operator’s discretion. After deployment of the MANTA VCD, a peripheral balloon was advanced over the 0.018-inch guidewire through the left radial or the contralateral CFA up to the target CFA access site and inflated at low (6-8) atmospheres for up to 1 minute (arteriotomy-site ballooning), which was combined with concomitant manual compression; the balloon/CFA diameter ratio was 0.8:1.0. Finally, a selective femoral angiogram was made using 2 orthogonal projections to confirm hemostasis and rule out vascular complications. A 2-dimensional (2D) color Doppler exam of the femoral access site was performed after the procedure to confirm effective access-site closure and CFA patency.
Primary outcome measures
The primary endpoints were 1) VCD failure, defined as a failed hemostasis at the access site resulting in an alternative treatment (other than manual compression or planned adjunctive endovascular balloon inflation)18; 2) predictors of VCD failure; and 3) access-site and access-related major and minor vascular complications, according to the Valve Academic Research Consortium-3 (VARC-3) definition.18 Hemostasis was defined as cessation of access-site bleeding as determined by visual inspection and angiography. Prolonged manual compression was defined as lasting more than 10 minutes.12 Hematoma with a diameter of greater than 5 cm was defined as large.
Secondary outcome measures
The secondary endpoints were 1) VARC-3 bleeding rate18; 2) acute kidney injury (AKI) rate18; 3) time to hemostasis (TTH), defined as the elapsed time between MANTA VCD deployment (withdrawal of the sheath from the artery) and the first observed and confirmed arterial hemostasis (no or minimal subcutaneous oozing and the absence of expanding or developing hematoma); 4) procedural length; and 5) length of in-hospital stay (LOS). The Society of Thoracic Surgeons Predicted Risk Of Mortality (STS-PROM) and the EuroSCORE II were used to estimate the risk of death at 30 days after surgery. The PREDICT-TAVI score was used to estimate the risk of bleeding.19 Calcification of the CFA at the puncture site was estimated as the absolute value of the circumferential calcium distribution, assessed according to its anterior or posterior location. SFAR was defined as the ratio between the maximum outer diameter of the sheath and the minimal diameter of the CFA. A SFAR greater than 1.05 was considered a predictor of vascular complications.2 Puncture height was the distance (cm) between the bifurcation and arteriotomy, as identified by the radiopaque stainless steel lock of the MANTA VCD.20 A puncture height of less than 0 cm or greater than or equal to 2.0 cm was considered high risk for vascular complications.20
Statistical analysis
Continuous variables are given as mean ± 1 SD or the median and first and third quartiles (Q1-Q3), when appropriate. The Student t test and the nonparametric Mann-Whitney U test were used to determine differences between continuous values for normally and not normally distributed variables, respectively. Normality assumption was verified graphically (ie, QQ plot) and was confirmed using the Shapiro-Wilk test. Equality of variances was tested among groups by the Levene’s test. Categorical variables were reported as percentages and were analyzed by either chi-square or Fisher’s exact test, as appropriate. Receiver operating characteristic (ROC) curve was generated, and the area-under-curve (AUC) was calculated to evaluate the sensitivity and specificity of the CFA minimum diameter for VCD failure. The optimal diameter cutoff was identified by the Youden index.21 Multiple logistic regression analysis was performed to determine independent predictors of VCD failure. Main confounders were selected according to literature and significance (P < .1) at univariate analysis, using the occurrence of VCD failure as a dependent variable. Next, a multivariate model was designed. To increase its stability, 200 bootstrap iterations were computed. Variance Inflation Factor analysis was implemented to exclude collinearity. The Hosmer-Lemeshow goodness-of-fit test was also assessed. These results were reported as odds ratio (OR) and 95% CI. No correction for multiplicity was used for secondary endpoints; therefore, the related findings should be considered exploratory. Sample size estimation was not performed. A P-value of less than 0.05 was considered significant. All analyses were conducted with SPSS v20.0 (IBM).
Results
Patient population
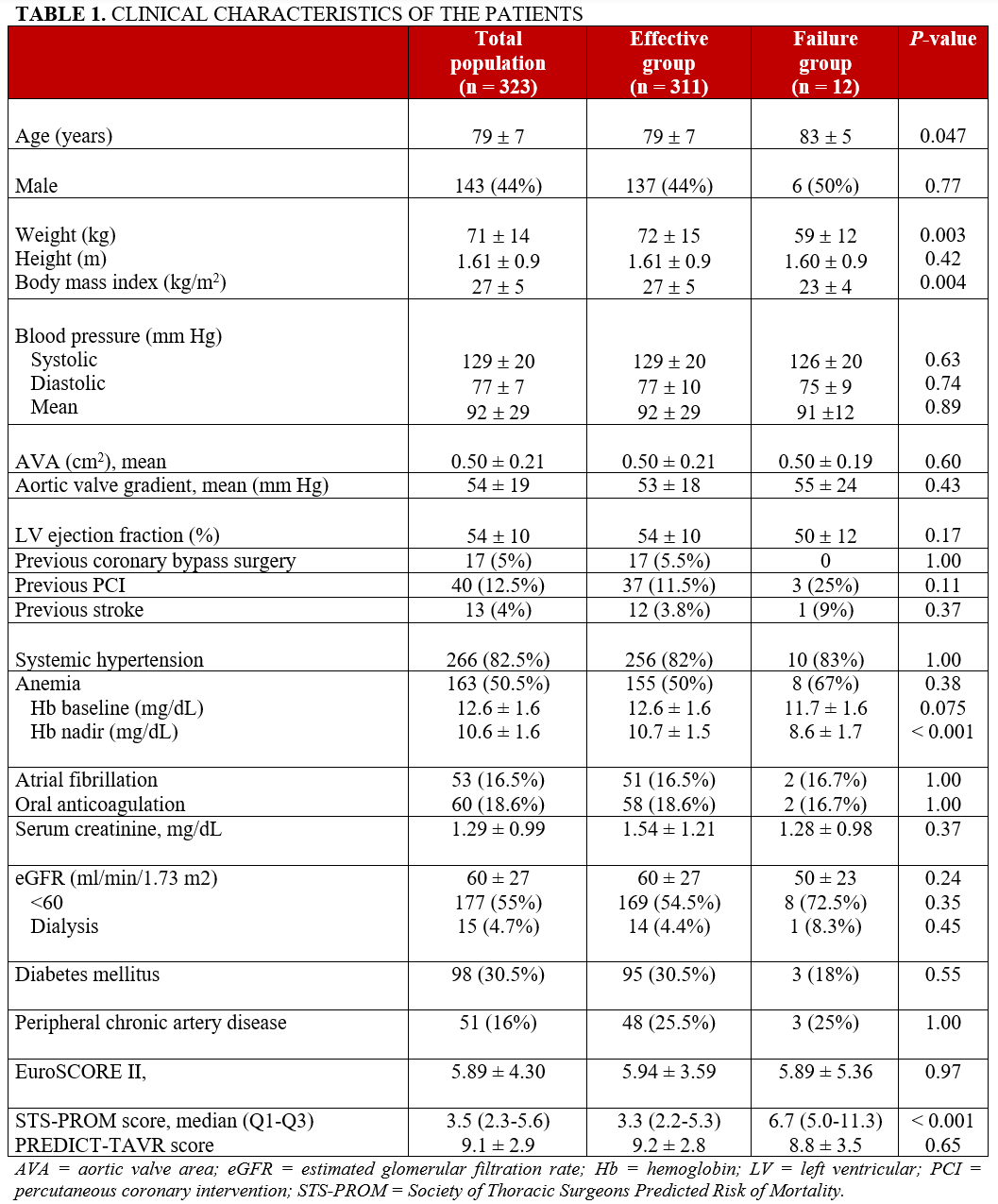
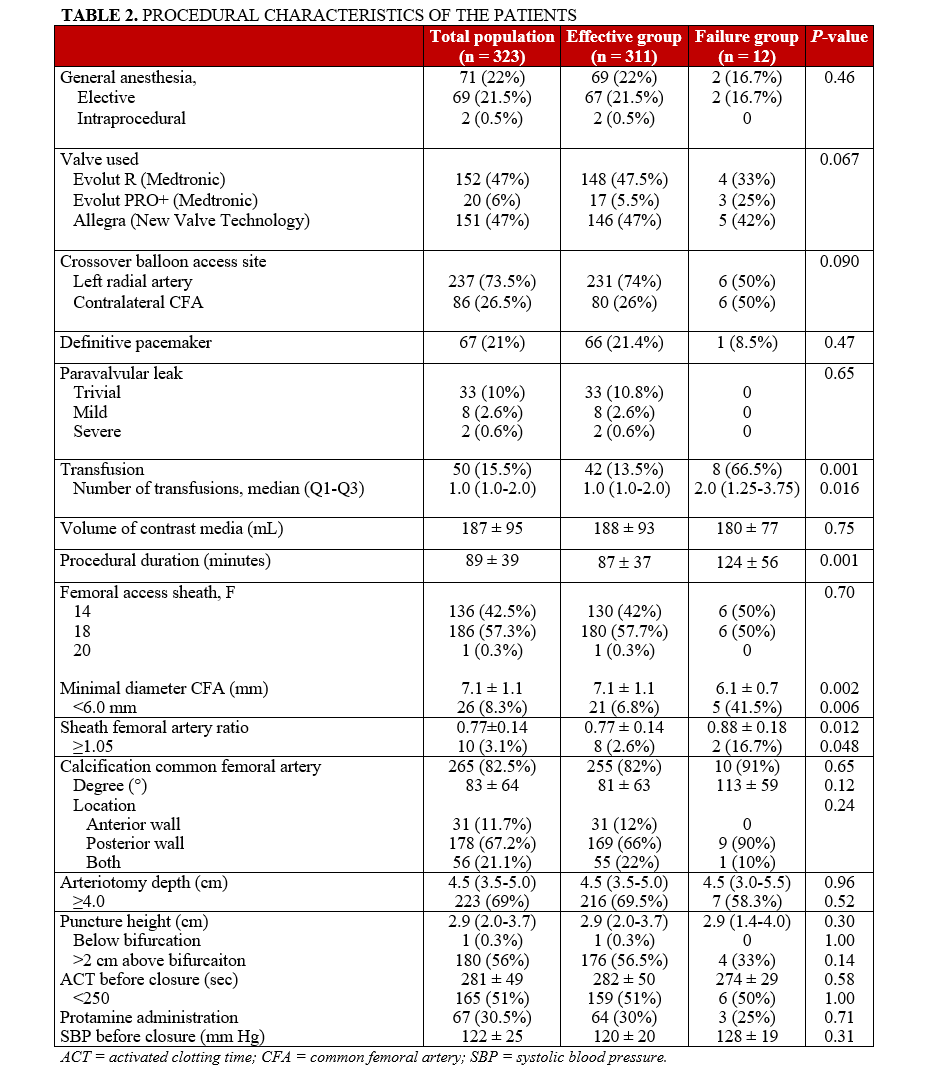
The clinical and procedural characteristics of the included patients are reported in Tables 1 and 2. The Evolut R or Evolut PRO+ was implanted in 172 (53%) patients, and the ALLEGRA in 151 (47%) patients. Moderate-to-severe paravalvular aortic regurgitation was observed in 10 (3.1%) cases, whereas a definite pacemaker was implanted in 67 (21%) patients. The 14F MANTA VCD was used in 136 (42%) patients and the 18F MANTA VCD in 187 (58%). No patient experienced access-related non-vascular complications.
VCD failure
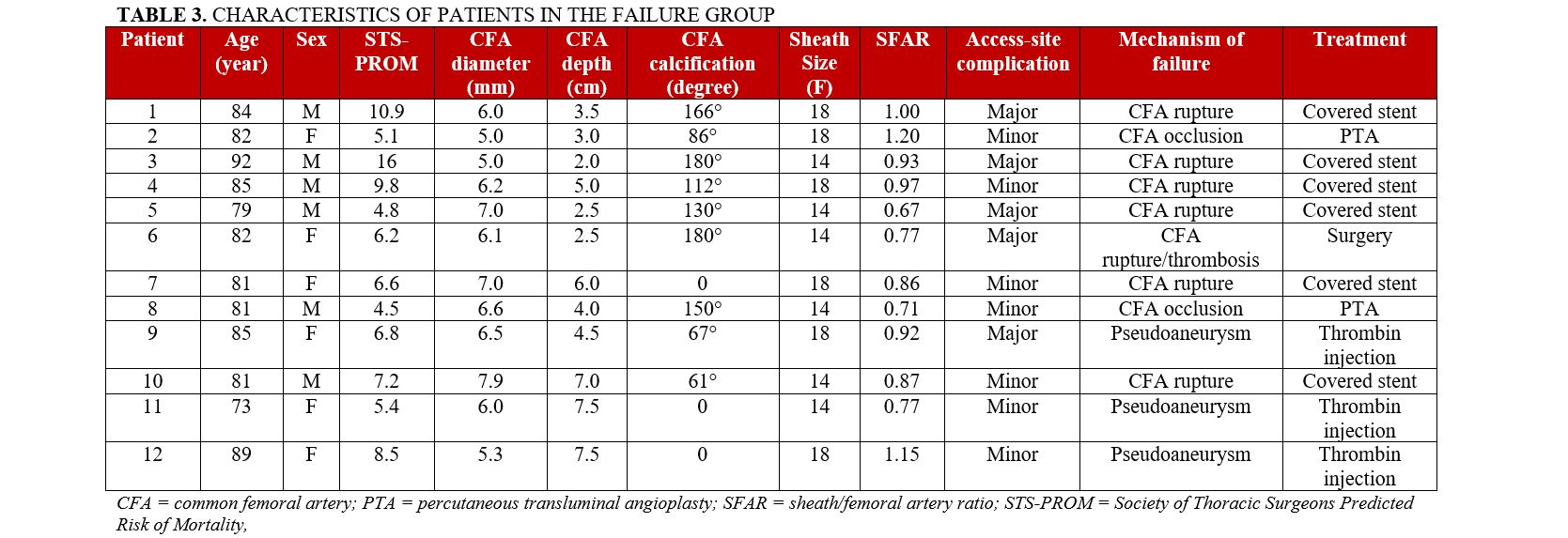
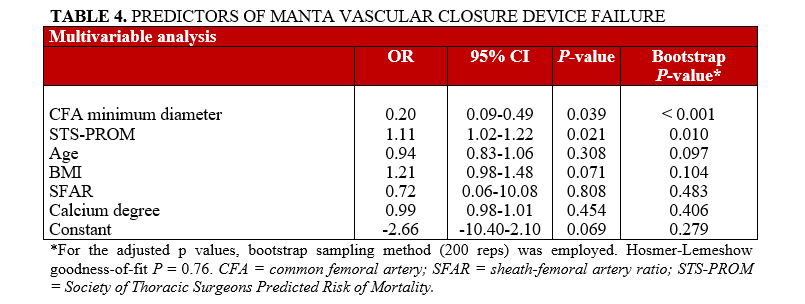
The MANTA-VCD was effective in 311 (96.3%) patients (Effective group) and failed to achieve hemostasis in 12 (3.7%) patients (Failure group). In all patients in the Effective group, post-procedural and discharge 2D eco-color-Doppler exam confirmed effective access-site closure and arterial patency (mean diameter stenosis, 10 ± 8%). Patients in the Failure group were older, with lower body mass index and higher STS-PROM score (Table 1). The characteristics of these subjects, including the potential failure mechanisms and their treatment, are reported in Table 3. The 18F MANTA VCD was applied in 6 (50%) patients in the Failure group and 181 (58%) patients in the Effective group (P = .53). The CFA minimal diameter was smaller in the Failure group (6.1 ± 0.7 mm vs 7.1 ± 1.1 mm; P = .002). The degree of CFA calcification (113° ± 59° vs 81° ± 63°, P = .12) and the arteriotomy depth (4.5 [3.0-5.5] vs 4.5 [3.5-5.0] cm, P = .96) were similar between the 2 groups (Table 2). The SFAR was higher in the Failure group (0.88 ± 0.18 vs 0.77 ± 0.14; P = .012): specifically, the SFAR was greater than or equal to 1.05 in 10 (3.1%) patients: 8 (2.6%) in the Effective group and 2 (16.7%) in the Failure group (P = .048). Independent predictors of VCD failure were minimum CFA diameter and STS-PROM score (Table 4). ROC analysis showed the CFA minimum diameter with an AUC of 0.77 (95% CI, 0.69-0.86; P < .001); the best cutoff was 6.30 mm (sensitivity 83%; specificity 59%; Youden’s index = 0.41; positive predictive value 7%; negative predictive value 99%) (Figure 1).
Access-site vascular complications
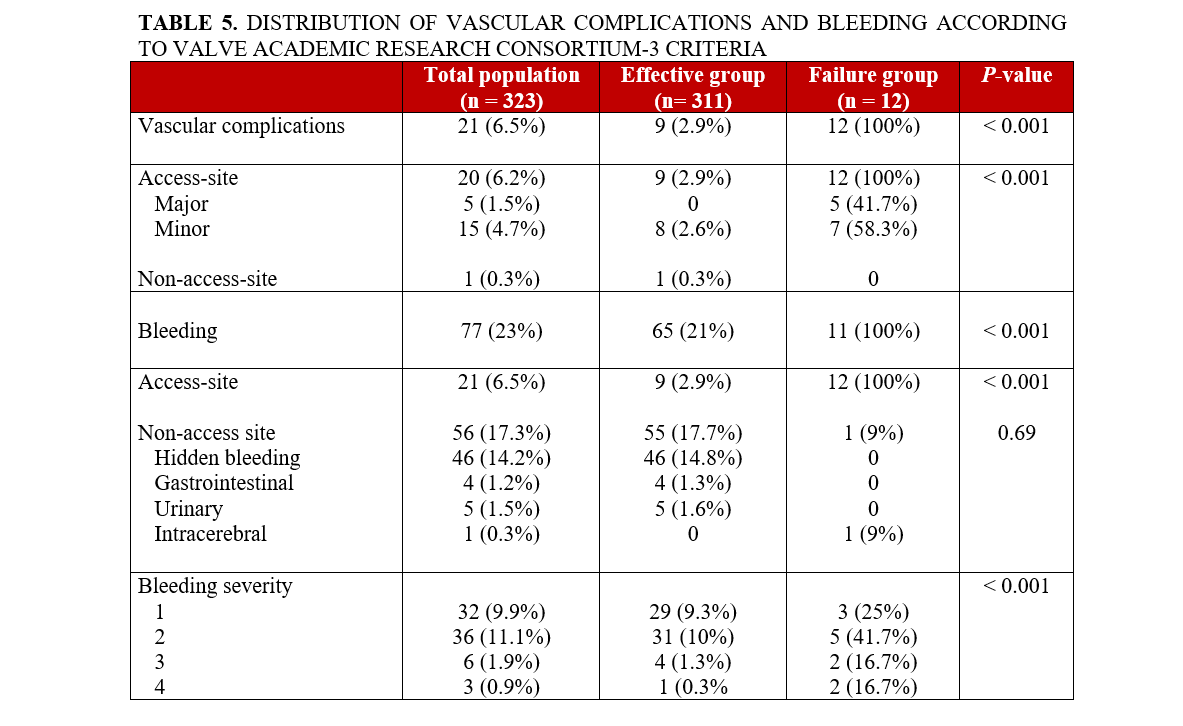
Access-site major and minor vascular complications occurred in 21 (6.5%) patients; this included all 12 patients in the Failure group and 9 patients in the Effective group (Tables 3 and 5). The 9 patients in the Effective group suffered from hematomas: 8 in the TAVI access site and 1 in the contralateral femoral artery (Table 5). Large hematoma occurred in 3 of these 9 patients.
Secondary endpoints
Non-access-site bleeding occurred in 55 (17.7%) patients in the Effective group and in 1 (9%) patient in the Failure group (P = .69; Table 5). One (9%) patient in the Failure group experienced both access-site and non-access-site (intracerebral hemorrhage) complications. The distribution of bleeding severity according to the VARC-3 criteria in the 2 groups is reported in Table 5. The packed red blood cell transfusion rate was higher in the Failure group (66.5% vs 13.5%; P = .001) (Table 2). AKI occurred in 48 of the 308 (15.6%) patients without end-stage renal disease at baseline (6 of 11 [54.5%] in the Failure group and 42 of 297 [14.1%] in the Effective group [OR, 1.12; 95% CI, 1.03-1.12; P = .004]).
The median TTH was 2 (Q1-Q3 = 2-3) minutes in the global population: 2 (Q1-Q3 = 2-5) minutes in the Effective group and 12 (Q1-Q3 = 10-16) minutes in the Failure group (P < .001). Specifically, the TTH was less than 10 minutes in 284 (87.9%) patients (2 [16.7%] in the Failure group and 282 [90.7%] in the Effective group; P < .001).
The procedural duration was 89 ± 39 minutes: 87 ± 37 minutes in the Effective group vs 124 56 minutes in the Failure group (P < .001). In-hospital death occurred in 9 (2.8%) patients: 3 of 12 (25%) in the Failure group and 6 of 311 (2%) in the Effective group (OR, 1.46; 95% CI, 1.06-2.32; P = .002). The average length of stay was 9.5 ± 5.2 days (14.5 ± 7.2 days in the Failure group and 9.4 ± 5.0 days in the Effective group; P = .029).
Discussion
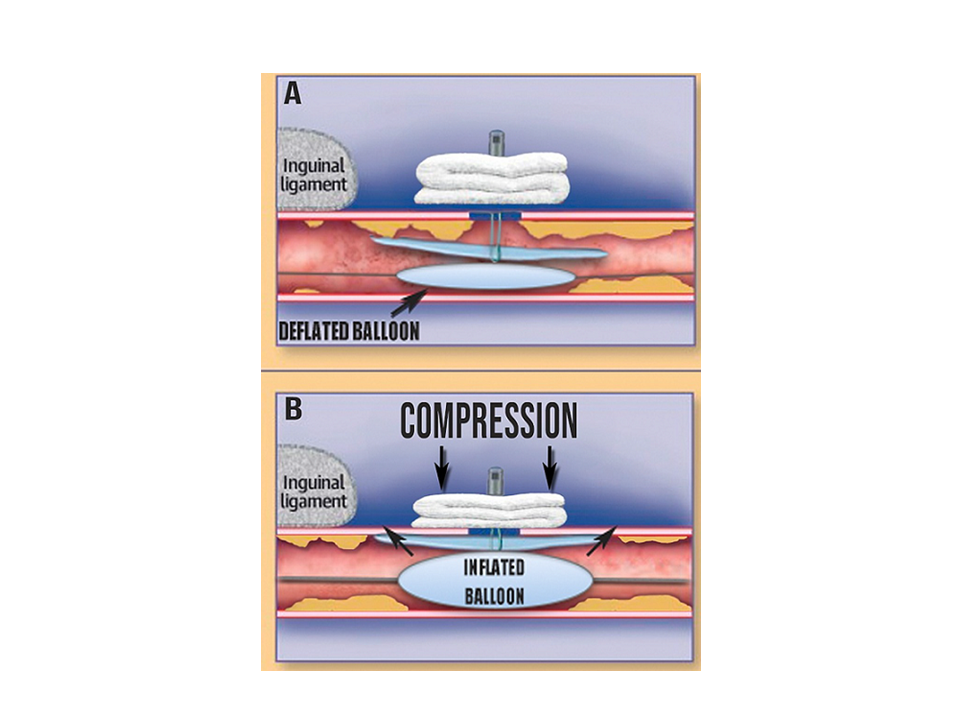
To date, suture-based techniques represent the most widely used approach to achieve hemostasis after transfemoral TAVI; these techniques involve the implantation of 1 or 2 ProGlide VCDs before large-bore access sheath positioning.22-25 This practice is backed by evidence from randomized controlled trials, which do not support the superiority of the plug-based VCD over the suture-based VCD.11,12 Although the MANTA VCD offers the advantage of a single-device use per closure, its major drawback is the inability to use additional devices in case of failure because vessel access is lost after the deployment of the collagen plug. On the contrary, suture-based VCD allows the operator to keep the guidewire inside the CFA throughout the entire closure phase, which allows the possibility of using an additional VCD in case of ineffective hemostasis. Several mechanisms of failure of the MANTA VCD have been previously described: 1) incomplete apposition of toggle-plug assembly, 2) occlusion of the artery by the toggle, or 3) collagen waist in the subcutaneous tract.15 The systematic use of the arteriotomy-site ballooning technique plus concomitant manual compression may counteract at least 2 of those mechanisms and, possibly, optimize toggle-plug unit apposition to the CFA wall (Figure 2). This approach should not be confused with the crossover occlusion-balloon technique, which is indicated to facilitate hemostasis with a suture-based VCD26,27 rather than the plug-based MANTA VCD.
The systematic use of this technique may be supported by the lower rates of both VCD failure and access-site complications observed in our study compared with previous ones (Supplemental Table). Indeed, the reported rate of MANTA VCD failures ranged from 4.7% in the CHOICE-CLOSURE trial12 to 20% in the MASH trial.11 Furthermore, in the MANTA-based group, access site or access-related major and minor vascular complications occurred in 19.4% of cases in the CHOICE-CLOSURE trial12 and 10% in the MASH trial.11 A previous meta-analysis of 9 observational studies and 2 randomized controlled trials (including 3123 patients) reported that the rate of major and minor vascular complications in the plug-based group was 12%.5 In another meta-analysis of 8 observational studies and 1 randomized controlled trial (including 2865 patients), the rate of major and minor vascular complications with the MANTA VCD was 14.5%.3 Similarly, according to the recent PULSE registry, the access-related vascular complications rate was 14.9% in patients treated with the MANTA device.28 In regards to bleeding events, we observed a 6.5% access-site-related bleeding rate in our cohort. In the CHOICE-CLOSURE trial,12 access-site-related bleedings occurred in 11.6% of patients, while this rate was 9% in the MASH trial.11 Notably, this alternative closure strategy may have also contributed to the reduction of both pseudoaneurysms (< 1%) and hematomas (< 3%), compared with previous studies.7,11,12
The systematic use of arteriotomy-site ballooning following MANTA VCD delivery has some drawbacks. First, it can significantly prolong the TTH. In the present study, the median TTH was 2 minutes (Q1-Q3 = 2-3) in the global population, which is longer than previously reported.7,11,12,29,30 Second, this strategy conflicts with the minimalist TAVI approach28,31 routine pre-positioning of a wire in the femoral access site through the radial or contralateral iliofemoral system is not routinely adopted because of the increase in resource use (time and equipment).
According to our findings, independent predictors of MANTA VCD failure were small CFA diameter and high STS-PROM score. The relationship between CFA diameter and the risk of failure in this setting has been previously reported.20 In our work, we confirmed this finding and showed that a CFA diameter of less than or equal to 6.30 mm could be the best cutoff for predicting MANTA VCD failure. The high negative predictive value we observed suggests that this device should be avoided when dealing with small CFA diameters. The presence and amount of calcification, as well as the distance of the puncture site from the bifurcation have been identified as additional predictors of MANTA VCD failure. In our cohort, CFA calcification was present in the majority (86%) of patients. Although not statistically significant, the mean calcification degree was higher in the Failure group, with a prevalent posterior location. Plug opposition in severely calcified vessels can be challenging, as the device’s toggle may interact with calcium. Although we acknowledge that a larger sample size would have probably confirmed the predictive role of CFA posterior calcification, the systematic use of arteriotomy-site ballooning following MANTA VCD delivery may have partially mitigated its detrimental effect on vascular access sealing.
In previous studies, both low (ie, at or below the femoral bifurcation) and high (> 2 cm above the femoral bifurcation) punctures were identified as predictors for clinically relevant vascular complications in previous studies.20,32 However, in our work, CFA puncture below the bifurcation occurred in only 1 patient, whereas CFA puncture was greater than 2 cm above the bifurcation in the majority (56%) of subjects. In the study by van Wiechen et al, CFA puncture below the bifurcation and greater than 2 cm above the bifurcation occurred in 9% and 39% of patients, respectively.19 The different distribution of puncture sites may explain this heterogenous report.
Finally, the present study underscores that a significant proportion (~14%) of patients exhibit drops in hemoglobin levels, despite having no obvious source of bleeding.33,34 Nuis et al reported that the indication of blood transfusion was unrelated to overt bleeding in more than one-half of TAVI patients with anemia.35 This drop is likely multifactorial; hemodilution due to postoperative hydration may result in anemia detection without overt bleeding, and acute stress and catheter exchanges can lead to changes in volume status and consequent hemoglobin decrement. Similarly, while the rates of death events were comparable with those of previous major reports investigating this topic,12,28 we found that the survival rate of patients in the Failure group was notably reduced. While the association between failed vascular sealing and death has been largely demonstrated,1 to the best of our knowledge, previous works did not report the actual mortality rates of patients who underwent a failed closure attempt with MANTA VCD. Therefore, this finding is hardly comparable with previous ones. The fact that a mortality score (STS-PROM) predicted the risk of VCD failure could partially justify this trend; however, this is only hypothetical. Overall, significant efforts should be spent to avoid and carefully manage failed vascular closure attempts with either plug- or suture-based VCDs to reduce the risk of major adverse events and death.
Limitations
The present study has several limitations. First, as a single-center, observational study, our results may be subject to unmeasured confounding and may not be fully generalizable to broader patient populations. The lack of a control group to compare the alternative delivery strategy with standard techniques represents a major limitation. Randomized controlled trials and/or large registries are needed to clarify whether the systematic use of arteriotomy-site ballooning technique following MANTA VCD delivery improves its efficacy and safety. The lack of a Core-Lab adjudication of endpoints represents a further limitation. Moreover, the absence of a pre-specified sample size computation and the low event rate may have exposed our study to the risk of underpowering. In this regard, the small number of VCD failure events limits the robustness of the multivariable regression model, increasing the risk of overfitting, wide confidence intervals, and unstable estimates. As such, the regression-analysis findings should be interpreted as exploratory and hypothesis-generating. Finally, in the present study CFA puncture was carried out by road-mapping guide. Future studies are needed to clarify whether ultrasound-guided arterial punctures may improve MANTA VCD efficacy and safety.
Conclusions
The systematic use of the arteriotomy-site ballooning plus concomitant manual compression following MANTA VCD delivery may optimize toggle-plug assembly apposition to the CFA wall and should be adopted to improve the final hemostatic efficacy. Furthermore, plug-based MANTA VCD should be avoided when dealing with small (< 6.3 mm) CFA diameter.
Affiliations and Disclosures
Carlo Briguori, MD, PhD1; Luca Paolucci, MD1; Mario Scarpelli, MD1; Antonietta Di Iorio, MD1; Valeria Cavaliere, MD1; Amelia Focaccio, MD1; Francesca De Micco, PhD1; Daniele Maselli, MD2
From the 1Interventional Cardiology and 2Cardiac Surgery Units, Mediterranea Cardiocentro, Naples, Italy.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Carlo Briguori, MD, PhD, FACC, FSCAI, Interventional Cardiology Unit, Mediterranea Cardiocentro, Via Orazio 2, Naples 80121, Italy. Email: carlobriguori@clinicamediterranea.it
References
1. van Kesteren F, van Mourik MS, Vendrik J, et al. Incidence, predictors, and impact of vascular complications after transfemoral transcatheter aortic valve implantation with the SAPIEN 3 prosthesis. Am J Cardiol. 2018;121(10):1231-1238. doi:10.1016/j.amjcard.2018.01.050
2. Hayashida K, Lefèvre T, Chevalier B, et al. Transfemoral aortic valve implantation new criteria to predict vascular complications. JACC Cardiovasc Interv. 2011;4(8):851-858. doi:10.1016/j.jcin.2011.03.019
3. Doshi R, Vasudev R, Guragai N, et al. Clinical outcomes of MANTA vs suture-based vascular closure devices after transcatheter aortic valve replacement: an updated meta-analysis. Indian Heart J. 2023;75(1):59-67. doi:10.1016/j.ihj.2023.01.007
4. van Gils L, De Jaegere PP, Roubin G, van Mieghem NM. The MANTA vascular closure device: a novel device for large-bore vessel closure. JACC Cardiovasc Interv. 2016;9(11):1195-1196. doi:10.1016/j.jcin.2016.03.010
5. Al-Abdouh A, Abusnina W, Mhanna M, et al. MANTA versus suture-based closure devices following transcatheter aortic valve replacement: an updated meta-analysis. J Soc Cardiovasc Angiogr Interv. 2022;1(5):100397. doi:10.1016/j.jscai.2022.100397
6. Hoffmann P, Al-Ani A, von Lueder T, et al. Access site complications after transfemoral aortic valve implantation - a comparison of Manta and ProGlide. CVIR Endovasc. 2018;1(1):20. doi:10.1186/s42155-018-0026-0
7. Wood DA, Krajcer Z, Sathananthan J, et al; SAFE MANTA Study Investigators. Pivotal clinical study to evaluate the safety and effectiveness of the MANTA percutaneous vascular closure device: the SAFE MANTA study. Circ Cardiovasc Interv 2019;12(7):e007258. doi:10.1161/CIRCINTERVENTIONS.119.007258
8. Gheorghe L, Brouwer J, Mathijssen H, et al. Early outcomes after percutaneous closure of access site in transfemoral transcatheter valve implantation using the novel vascular closure device collagen plug-based MANTA. Am J Cardiol. 2019;124(8):1265-1271. doi:10.1016/j.amjcard.2019.07.030
9. De Palma R, Settergren M, Rück A, Linder R, Saleh N. Impact of percutaneous femoral arteriotomy closure using the MANTATM device on vascular and bleeding complications after transcatheter aortic valve replacement. Catheter Cardiovasc Interv. 2018;92(5):954-961. doi:10.1002/ccd.27595
10. Moriyama N, Lindström L, Laine M. Propensity-matched comparison of vascular closure devices after transcatheter aortic valve replacement using MANTA versus ProGlide. EuroIntervention. 2019;14(15):e1558-e1565. doi:10.4244/EIJ-D-18-00769
11. van Wiechen MP, Tchétché D, Ooms JF, et al. Suture- or plug-based large-bore arteriotomy closure: a pilot randomized controlled trial. JACC Cardiovasc Interv. 2021;14(2):149-157. doi:10.1016/j.jcin.2020.09.052
12. Abdel-Wahab M, Hartung P, Dumpies O, et al; CHOICE-CLOSURE Investigators. Comparison of a pure plug-based versus a primary suture-based vascular closure device strategy for transfemoral transcatheter aortic valve replacement: the CHOICE-CLOSURE randomized clinical trial. Circulation. 2022;145(3):170-183. doi:10.1161/CIRCULATIONAHA.121.057856
13. Al-Abcha A, Saleh Y, Halboni A, Wang E, Salam MF, Abela G. Meta-analysis investigating the efficacy and safety of the MANTA versus ProGlide vascular closure devices after transcatheter aortic valve implantation. Am J Cardiol. 2022;169:151-154. doi:10.1016/j.amjcard.2022.01.010
14. van Mieghem NM, Tchetche D, Chieffo A, et al. Incidence, predictors, and implications of access site complications with transfemoral transcatheter aortic valve implantation. Am J Cardiol. 2012;110(9):1361-1367. doi:10.1016/j.amjcard.2012.06.042
15. Moccetti F, Brinkert M, Seelos R, et al. Insights from a multidisciplinary introduction of the MANTA vascular closure device. JACC Cardiovasc Interv. 2019;12(17):1730-1736. doi:10.1016/j.jcin.2019.06.049
16. Vahanian A, Beyersdorf F, Praz F, et al; ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43(7):561-632. doi:10.1093/eurheartj/ehab395
17. Nuis RJ, Wood D, Kroon H, et al. Frequency, impact, and predictors of access complications with plug-based large-bore arteriotomy closure - a patient-level meta-analysis. Cardiovasc Revasc Med. 2022;34:69-74. doi:10.1016/j.carrev.2021.02.017
18. Généreux P, Piazza N, Alu MC, et al. Valve Academic Research Consortium 3: updated endpoint definitions for aortic valve clinical research. Eur Heart J. 2021;42(19):1825-1857. doi:10.1093/eurheartj/ehaa799
19. Navarese EP, Zhang Z, Kubica J, et al; a Joint Effort of the Italian and Polish Cardiac Interventional Societies. Development and Validation of a practical model to identify patients at risk of bleeding after TAVR. JACC Cardiovasc Interv. 2021;14(11):1196-1206. doi:10.1016/j.jcin.2021.03.024
20. van Wiechen MP, Kroon H, Hokken TW, et al. Vascular complications with a plug-based vascular closure device after transcatheter aortic valve replacement: predictors and bail-outs. Catheter Cardiovasc Interv. 2021;98(5):E737-E745. doi:10.1002/ccd.29506
21. Ruopp MD, Perkins NJ, Whitcomb BW, Schisterman EF. Youden Index and optimal cut-point estimated from observations affected by a lower limit of detection. Biom J. 2008;50(3):419-430. doi:10.1002/bimj.200710415
22. Rheude T, Ruge H, Altaner N, et al. Comparison of strategies for vascular ACCESS closure after transcatheter aortic valve implantation: the ACCESS-TAVI randomized trial. Eur Heart J. 2025;46(7):635-645. doi:10.1093/eurheartj/ehae784
23. Lata K, Kaki A, Grines C, Blank N, Elder M, Schreiber T. Pre-close technique of percutaneous closure for delayed hemostasis of large-bore femoral sheaths. J Interv Cardiol. 2018;31(4):504-510. doi:10.1111/joic.12490
24. Berti S, Bedogni F, Giordano A, et al; Italian Society of Interventional Cardiology‐GISE. Efficacy and safety of ProGlide versus Prostar XL vascular closure devices in transcatheter aortic valve replacement: the RISPEVA registry. J Am Heart Assoc. 2020;9(21):e018042. doi:10.1161/JAHA.120.018042
25. Genereux P, Kodali S, Leon MB, et al. Clinical outcomes using a new crossover balloon occlusion technique for percutaneous closure after transfemoral aortic valve implantation. JACC Cardiovasc Interv. 2011;4(8):861-867. doi:10.1016/j.jcin.2011.05.019
26. Junquera L, Vilalta V, Trillo R, et al. Transradial crossover balloon occlusion technique for primary access hemostasis during transcatheter aortic valve replacement: initial experience with the Oceanus 140 cm and 200 cm balloon catheters. J Invasive Cardiol. 2020;32(8):283-288. doi:10.25270/jic/20.00037
27. Kastengren M, Svenarud P, Källner G, Settergren M, Franco-Cereceda A, Dalén M. Percutaneous vascular closure device in minimally invasive mitral valve surgery. Ann Thorac Surg. 2020;110(1):85-91. doi:10.1016/j.athoracsur.2019.10.038
28. Grundmann D, Kim W, Kellner C, et al. A propensity-matched comparison of plug- versus suture-based vascular closure after TAVI. EuroIntervention. 2025;21(5):e272-e281. doi:10.4244/EIJ-D-24-00120
29. Krajcer Z, Wood DA, Strickman N, et al. Pivotal clinical study to evaluate the safety and effectiveness of the MANTA vascular closure device during percutaneous EVAR and TEVAR procedures. J Endovasc Ther. 2020;27(3):414-420. doi:10.1177/1526602820912224
30. van Mieghem NM, Latib A, van der Heyden J, et al. Percutaneous plug-based arteriotomy closure device for large-bore access: a multicenter prospective study. JACC Cardiovasc Interv. 2017;10(6):613-619. doi:10.1016/j.jcin.2016.12.277
31. Wood DA, Lauck SB, Cairns JA, et al. The Vancouver 3M (multidisciplinary, multimodality, but minimalist) clinical pathway facilitates safe next-day discharge home at low-, medium-, and high-volume transfemoral transcatheter aortic valve replacement centers: the 3M TAVR study. JACC Cardiovasc Interv. 2019;12(5):459-469. doi:10.1016/j.jcin.2018.12.020
32. Pitta SR, Prasad A, Kumar G, Lennon R, Rihal CS, Holmes DR. Location of femoral artery access and correlation with vascular complications. Catheter Cardiovasc Interv. 2011;78(2):294-299. doi:10.1002/ccd.22827
33. De Larochellière H, Puri R, Eikelboom JW, Rodés-Cabau J. Blood disorders in patients undergoing transcatheter aortic valve replacement: a review. JACC Cardiovasc Interv. 2019;12(1):1-11. doi:10.1016/j.jcin.2018.09.041
34. Tarantini G, Mojoli M, Barioli A, Battistel M, Généreux P. Blood oozing: a cause of life-threatening bleeding without overt source after transcatheter aortic valve replacement. Int J Cardiol. 2016;224:107-111. doi:10.1016/j.ijcard.2016.09.009
35. Nuis RJ, Sinning JM, Rodés-Cabau J, et al. Prevalence, factors associated with, and prognostic effects of preoperative anemia on short- and long-term mortality in patients undergoing transcatheter aortic valve implantation. Circ Cardiovasc Interv. 2013;6(6):625-634. doi:10.1161/CIRCINTERVENTIONS.113.000409










