

Endovascular Management of the Radial Artery: Success Through Minimal Invasion
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
An 84-year-old man with a history of dyslipidemia and hypertension underwent invasive coronary angiography (ICA) via his right radial artery because of acute coronary syndrome. After the procedure, a palpable pulse was noted in his right forearm, close to the site of the radial artery puncture. Ultrasonography was performed and a radial pseudoaneurysm (RPA) was noted. Ultrasound-guided compression proximal to the neck of the RPA was unsuccessful.
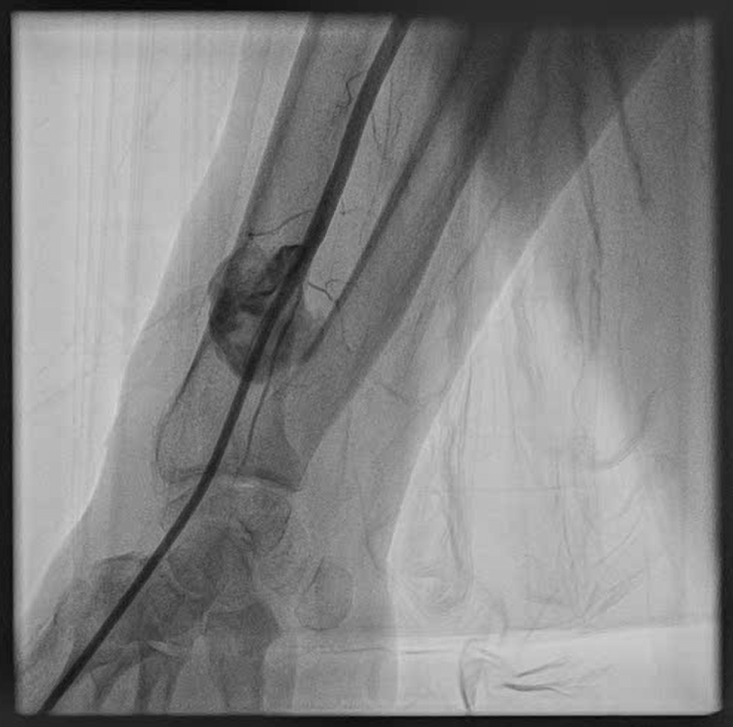
Because of the absence of injectable thrombin solution and the frail condition of the patient, it was decided to proceed with an endovascular approach. A 6F sheath was introduced in the distal radial artery (Figures 1 and 2, Video 1). Using a 6F Judkins catheter, a 0.014-inch guidewire was introduced inside the radial artery through the base of the RPA and distal to the brachial artery. A 3 x 24-mm polytetrafluoroethylene-covered stent was deployed initially, but with residual leak (Figure 3, Video 2). A second 3 x 18-mm covered stent was deployed, with minimal contrast flow inside the RPA. Final post-dilatation was performed with a 3.5 x 15-mm noncompliant balloon, with no residual flow inside the pseudoaneurysm. (Figure 4, Videos 3 and 4).
After the procedure, the palpable pulse of the RPA had disappeared. Ultrasonography of the area 24 hours post-procedure confirmed a thrombosed RPA and a good flow in the radial artery. One month later, the patient had no signs of relapse. Although no formal guidelines define the duration of dual antiplatelet therapy (DAPT) for covered-stent implantation in the radial artery, the patient’s bleeding and ischemic risk should be taken into consideration, and a DAPT duration (combining aspirin and a P2Y12 inhibitor) of up to 6 months is considered reasonable.
Radial artery pseudoaneurysm is a rare complication after ICA; other complications include thrombosis, bleeding, ischemia, and arteriovenous communication. Predisposing factors for RPA are inadequate hemostasis, anticoagulant therapy, multiple efforts of radial artery puncture, and large arterial sheath sizes.



Affiliations and Disclosures
Panagiotis Varelas, MD, MSc; Konstantinos Manousopoulos, MD, PhD; Konstantinos Filippou, MD, MSc; Dimitrios Karelas, MD, MSc; Ioannis Papadopoulos, MD; Ioannis Tsiafoutis, MD, PhD
From the Second Cardiology Department, Hellenic Red Cross Hospital Korgialenio-Benakio, Athens, Greece.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and to the publication of this manuscript, including any and all images.
Address for correspondence: Panagiotis Varelas, MD, MSc, Second Cardiology Department, Hellenic Red Cross Hospital Korgialenio-Benakio, Athens, Greece Athanasaki 1, Athens 11526, Greece. Email: pvarelas@outlook.com; X: @panagiotisvar17











